You might also like
- Advanced Laser Al170: Instruction ManualDocument35 pagesAdvanced Laser Al170: Instruction ManualJuan Camilo100% (1)
- WebpdfDocument276 pagesWebpdfprateekvNo ratings yet
- 6000 Most Common Korean Words - For All TOPIK Levels PDFDocument232 pages6000 Most Common Korean Words - For All TOPIK Levels PDFZac67% (3)
- Exposure Chart Mobile X Ray PDFDocument8 pagesExposure Chart Mobile X Ray PDFlutfiaNo ratings yet
- Patricia Faisca - A Concise Introduction To Thermodynamics For Physicists-CRC Press (2022)Document237 pagesPatricia Faisca - A Concise Introduction To Thermodynamics For Physicists-CRC Press (2022)Piotr Jankowski100% (1)
- صيانة المولدات و المحولات الكهربائيهDocument15 pagesصيانة المولدات و المحولات الكهربائيهMostafa AllamNo ratings yet
- TERTIARY X-RADIATIONâ A PROBLEM FOR STAFF PROTECTION - (Radiation Protection Dosimetry) (2020)Document8 pagesTERTIARY X-RADIATIONâ A PROBLEM FOR STAFF PROTECTION - (Radiation Protection Dosimetry) (2020)Piotr JankowskiNo ratings yet
- Laser Targeting With C-Arm FluorosDocument6 pagesLaser Targeting With C-Arm Fluorosramankarnwal1971No ratings yet
- Awareness of Radiation Hazard in Orthopaedic Residents Surgeon in A Central IndiaDocument5 pagesAwareness of Radiation Hazard in Orthopaedic Residents Surgeon in A Central IndiaIJAR JOURNALNo ratings yet
- JCDR 9 RC01Document4 pagesJCDR 9 RC01Karen MachadoNo ratings yet
- Scatter and Staff Dose Level in Paediatric Intervencionism PDFDocument8 pagesScatter and Staff Dose Level in Paediatric Intervencionism PDFsebastian CarrascoNo ratings yet
- LawsonDocument7 pagesLawsonrodolfo gorveñaNo ratings yet
- Measurement of Scattered and Transmitted Xrays From Intraoral An 2018Document13 pagesMeasurement of Scattered and Transmitted Xrays From Intraoral An 2018MahiraNo ratings yet
- UntitledDocument12 pagesUntitledapi-239502672No ratings yet
- Intraoperative Radiation Safety in Orthopaedics ADocument8 pagesIntraoperative Radiation Safety in Orthopaedics AFlame OrangeNo ratings yet
- European Journal of Radiology: Radiation Protection of Medical StaffDocument4 pagesEuropean Journal of Radiology: Radiation Protection of Medical Staffr_ayuNo ratings yet
- C-Arm Parts and PrinciplesDocument10 pagesC-Arm Parts and PrinciplesErshad SohailNo ratings yet
- Sarti 2012Document12 pagesSarti 2012mariaNo ratings yet
- AUWALDocument34 pagesAUWALYahya MusaNo ratings yet
- Radiation Exposure of Filipino Orthopedic Surgeons A Multi Center Study in Tertiary Level HospitalsDocument5 pagesRadiation Exposure of Filipino Orthopedic Surgeons A Multi Center Study in Tertiary Level HospitalsjojoNo ratings yet
- Dosis Radiasi Dari Tindakan Ct-Scan KepalaDocument9 pagesDosis Radiasi Dari Tindakan Ct-Scan KepalaCahya Budi UtamaNo ratings yet
- Assesment of Entrance Skin Doses For Patients - Abdullah Medical CityDocument4 pagesAssesment of Entrance Skin Doses For Patients - Abdullah Medical CityGeorgiana KokonaNo ratings yet
- Dosis Radiasi Dari Tindakan Ct-Scan Kepala PDFDocument9 pagesDosis Radiasi Dari Tindakan Ct-Scan Kepala PDFVergeen OllshopNo ratings yet
- Radiography Protectn FR Orthodontist Ajo2005Document5 pagesRadiography Protectn FR Orthodontist Ajo2005Dr S KNo ratings yet
- Patient Radiation Dose and Protection From Cone-Beam Computed TomographyDocument7 pagesPatient Radiation Dose and Protection From Cone-Beam Computed TomographydaruNo ratings yet
- Ajnr A5038 FullDocument6 pagesAjnr A5038 FullKevin Pratama PutraNo ratings yet
- Dosis Radiasi Dari Tindakan Ct-Scan Kepala: November 2014Document9 pagesDosis Radiasi Dari Tindakan Ct-Scan Kepala: November 2014wirputNo ratings yet
- Immersive Radiation Experience For Interventional Radiology With Virtual Reality Radiation Dose Visualization Using Fast Monte Carlo Dose EstimationDocument10 pagesImmersive Radiation Experience For Interventional Radiology With Virtual Reality Radiation Dose Visualization Using Fast Monte Carlo Dose EstimationFarimah AbbaspourNo ratings yet
- Ultrasound Guidance - PollardDocument72 pagesUltrasound Guidance - Pollardmasquebolso100% (3)
- Icrp 117Document102 pagesIcrp 117Sari BustillosNo ratings yet
- C-Arm Positioning Is A Significant Source of Radiation in Spine SurgeryDocument4 pagesC-Arm Positioning Is A Significant Source of Radiation in Spine SurgeryPablo IbañezNo ratings yet
- Abstract No. 301 - Angiographic Catheters - A Comprehensive Review For The Interventionalist In-TrainingDocument2 pagesAbstract No. 301 - Angiographic Catheters - A Comprehensive Review For The Interventionalist In-TrainingPeter LiNo ratings yet
- Uji Efektifitas Dinding Ruangan Panoramik Instalasi Radiologi RSUD Prof. Dr. MA Hanafiah SM Batusangkar Menggunakan TLD-100Document10 pagesUji Efektifitas Dinding Ruangan Panoramik Instalasi Radiologi RSUD Prof. Dr. MA Hanafiah SM Batusangkar Menggunakan TLD-100Nanang AdraverycildNo ratings yet
- Electron Beam Total Skin Irradiation PDFDocument1 pageElectron Beam Total Skin Irradiation PDFVictorM.LópezGuadalupeNo ratings yet
- A Comparative Study On The Diagnostic Utility of Ultrasonography With Conventional Radiography and Computed Tomography Scan in DDocument5 pagesA Comparative Study On The Diagnostic Utility of Ultrasonography With Conventional Radiography and Computed Tomography Scan in DGede AnjasmaraNo ratings yet
- Assessment of Occupational Radiation Among Medical Staff in Health Staff at Aminu Kano Teaching Hospital KanoDocument36 pagesAssessment of Occupational Radiation Among Medical Staff in Health Staff at Aminu Kano Teaching Hospital KanoYahya MusaNo ratings yet
- 1 s2.0 S1687850721003289 MainDocument10 pages1 s2.0 S1687850721003289 Mainsouhaila soulNo ratings yet
- Iranjradiol 10 14Document7 pagesIranjradiol 10 14ChristianWicaksonoNo ratings yet
- Chan 2015Document10 pagesChan 2015Innes AndrianiNo ratings yet
- FiltrationDocument16 pagesFiltrationjojokawayNo ratings yet
- Patient Safety in Medical ImagingDocument13 pagesPatient Safety in Medical ImagingC JoanesNo ratings yet
- EMT Medical Imaging Guide and CoP Document Outline-5!26!2021 - revASMDocument27 pagesEMT Medical Imaging Guide and CoP Document Outline-5!26!2021 - revASMDanny MarcilloNo ratings yet
- IJMP - Volume 14 - Issue 2 - Pages 87-91Document5 pagesIJMP - Volume 14 - Issue 2 - Pages 87-91Jojo KawayNo ratings yet
- C Arm Intro NewDocument14 pagesC Arm Intro NewAi ÅiNo ratings yet
- Abat F. 2019. Comparison US Guided vs. Blind Interventions Supraspinatus TendinopathyDocument10 pagesAbat F. 2019. Comparison US Guided vs. Blind Interventions Supraspinatus TendinopathyJavier MartinNo ratings yet
- WorldJNuclMed143189-8541241 234332Document8 pagesWorldJNuclMed143189-8541241 234332arief oktavaNo ratings yet
- Radiation Exposure Optimization During Cryobaloon AblationDocument8 pagesRadiation Exposure Optimization During Cryobaloon AblationfofikoNo ratings yet
- Gamma Factors For XRAYDocument8 pagesGamma Factors For XRAYcindy anggrilitaNo ratings yet
- Applied Radiation and Isotopes: H. Olaya Dávila, J.A. Díaz Merchán, H.R. Vega Carrillo, S.A. Martínez OvalleDocument4 pagesApplied Radiation and Isotopes: H. Olaya Dávila, J.A. Díaz Merchán, H.R. Vega Carrillo, S.A. Martínez OvalleWahyudin husainNo ratings yet
- Evaluation of The Awareness of Radiation Protection Among Urology Doctors in Three Governmental Hospitals in Khartoum CityDocument61 pagesEvaluation of The Awareness of Radiation Protection Among Urology Doctors in Three Governmental Hospitals in Khartoum CitySaeed TebinNo ratings yet
- PR CBCT Minimum Dose For Maximum Safety ENDocument6 pagesPR CBCT Minimum Dose For Maximum Safety ENSam Al AbabNo ratings yet
- Medical Exposures Fact Sheet PDFDocument4 pagesMedical Exposures Fact Sheet PDFSrinivas VenkataramanNo ratings yet
- Radiation in Dental Practice: Awareness, Protection and RecommendationsDocument6 pagesRadiation in Dental Practice: Awareness, Protection and Recommendationschaithra collegeNo ratings yet
- Radiation Doses of Indirect and Direct Digital Cephalometric RadiographyDocument4 pagesRadiation Doses of Indirect and Direct Digital Cephalometric RadiographyMarilyn GonzalesNo ratings yet
- Rsna 2Document5 pagesRsna 2Cecilia BarabinoNo ratings yet
- Indications, Surgical Approach, Reduction, and Stabilization Techniques of Distal Radius FracturesDocument11 pagesIndications, Surgical Approach, Reduction, and Stabilization Techniques of Distal Radius FracturesSylvinho46No ratings yet
- Loose Dan WuchererDocument7 pagesLoose Dan Wucherersaifulmangopo123No ratings yet
- Jurnal RadiasiDocument8 pagesJurnal RadiasiIdham JufriNo ratings yet
- CT Radiation ProtectionDocument8 pagesCT Radiation ProtectionKhush JainNo ratings yet
- Jurnal InternasionalDocument6 pagesJurnal InternasionalBerlianaNo ratings yet
- Skull Base Chordoma: About Two Cases and LiteraturereviewDocument5 pagesSkull Base Chordoma: About Two Cases and LiteraturereviewIJAR JOURNALNo ratings yet
- IVUS (IntraVascular UltraSound) Image Guidance for Treatment of Aorto-Iliac PathologiesFrom EverandIVUS (IntraVascular UltraSound) Image Guidance for Treatment of Aorto-Iliac PathologiesNo ratings yet
- Thoracic Ultrasound and Integrated ImagingFrom EverandThoracic Ultrasound and Integrated ImagingFrancesco FelettiNo ratings yet
- CONSTRUCTION AND APPLICATION OF BREP PHANTOM FOR CHINESE WOMEN OF CHILDBEARING AGE IN RADIATION PROTECTION (Radiation Protection Dosimetry) (2020)Document13 pagesCONSTRUCTION AND APPLICATION OF BREP PHANTOM FOR CHINESE WOMEN OF CHILDBEARING AGE IN RADIATION PROTECTION (Radiation Protection Dosimetry) (2020)Piotr JankowskiNo ratings yet
- J Applied Clin Med Phys - 2023 - Jayarathna - The Effect of Integrating Knowledge Based Planning With MulticriteriaDocument14 pagesJ Applied Clin Med Phys - 2023 - Jayarathna - The Effect of Integrating Knowledge Based Planning With MulticriteriaPiotr JankowskiNo ratings yet
- J Applied Clin Med Phys - 2023 - Tasmara - Photoacoustic Imaging of Hidden Dental Caries Using Visible Light Diode LaserDocument9 pagesJ Applied Clin Med Phys - 2023 - Tasmara - Photoacoustic Imaging of Hidden Dental Caries Using Visible Light Diode LaserPiotr JankowskiNo ratings yet
- J Applied Clin Med Phys - 2023 - Liu - A Two Step Treatment Planning Strategy Incorporating Knowledge Based Planning ForDocument11 pagesJ Applied Clin Med Phys - 2023 - Liu - A Two Step Treatment Planning Strategy Incorporating Knowledge Based Planning ForPiotr JankowskiNo ratings yet
- J Applied Clin Med Phys - 2023 - Ikeda - Impact of CT Scan Parameters On Deformable Image Registration Accuracy UsingDocument9 pagesJ Applied Clin Med Phys - 2023 - Ikeda - Impact of CT Scan Parameters On Deformable Image Registration Accuracy UsingPiotr JankowskiNo ratings yet
- Abani K. Bhuyan - Fundamental Concepts of Molecular Spectroscopy-CRC Press (2023)Document323 pagesAbani K. Bhuyan - Fundamental Concepts of Molecular Spectroscopy-CRC Press (2023)Piotr JankowskiNo ratings yet
- Harish Kumar Banga. Rajesh Kumar. Parveen Kalra. Rajendra M. Belokar - Additive Manufacturing With Medical Applications-CRC Press (2022)Document340 pagesHarish Kumar Banga. Rajesh Kumar. Parveen Kalra. Rajendra M. Belokar - Additive Manufacturing With Medical Applications-CRC Press (2022)Piotr JankowskiNo ratings yet
- Monte-Carlo Simulation An Introduction For Engineers and Scientists (Alan Stevens)Document113 pagesMonte-Carlo Simulation An Introduction For Engineers and Scientists (Alan Stevens)titus KisengaNo ratings yet
- J Applied Clin Med Phys - 2023 - Zaini - Therapeutic Radiation Beam Output and Energy Variation Across ClinicsDocument8 pagesJ Applied Clin Med Phys - 2023 - Zaini - Therapeutic Radiation Beam Output and Energy Variation Across ClinicsPiotr JankowskiNo ratings yet
- Rishabha Malviya, Pramod Kumar Sharma, Sonali Sundram, Balamurugan Balusamy, Rajesh Kumar Dhanaraj - Bioinformatics Tools and Big Data Analytics For Patient Care-CRC Press (2022)Document241 pagesRishabha Malviya, Pramod Kumar Sharma, Sonali Sundram, Balamurugan Balusamy, Rajesh Kumar Dhanaraj - Bioinformatics Tools and Big Data Analytics For Patient Care-CRC Press (2022)Piotr JankowskiNo ratings yet
- J Applied Clin Med Phys - 2023 - Erratum Implementation and Validation of A Beam Current Transformer On A MedicalDocument1 pageJ Applied Clin Med Phys - 2023 - Erratum Implementation and Validation of A Beam Current Transformer On A MedicalPiotr JankowskiNo ratings yet
- Stereotactic Body Radiation Therapy For Metastases in Long BonesDocument1 pageStereotactic Body Radiation Therapy For Metastases in Long BonesPiotr JankowskiNo ratings yet
- Quality Guidelines For Volume Delineation in Radiation Oncology-1 - 230110 - 205912Document19 pagesQuality Guidelines For Volume Delineation in Radiation Oncology-1 - 230110 - 205912Raul Matute MartinNo ratings yet
- 419 Ncs Rapport 11 Quality Control of SimulatorsocrDocument66 pages419 Ncs Rapport 11 Quality Control of SimulatorsocrPiotr JankowskiNo ratings yet
- Radiochromic Film Dosimetry-1Document47 pagesRadiochromic Film Dosimetry-1Piotr JankowskiNo ratings yet
- The First-Fourth Books of The HitopadésaDocument116 pagesThe First-Fourth Books of The HitopadésaMiguel RosaNo ratings yet
- Silenat Berhanu SimaDocument6 pagesSilenat Berhanu SimaSilenat BerhanuNo ratings yet
- Bhaktavatsalam Memorial College For Women: Hand Book 2020 - 21Document37 pagesBhaktavatsalam Memorial College For Women: Hand Book 2020 - 21Anu RsNo ratings yet
- Framework For A Digital Twin in Manufacturing Scope and RequirementsDocument3 pagesFramework For A Digital Twin in Manufacturing Scope and RequirementsJoão Vitor100% (1)
- 3-Storeyed 31-3-2015-Schedule PDFDocument1 page3-Storeyed 31-3-2015-Schedule PDFSi Thu AungNo ratings yet
- How The Audiences Feel Closer and Connected To Their Culture With StorytellingDocument7 pagesHow The Audiences Feel Closer and Connected To Their Culture With Storytellingmarcelo quezadaNo ratings yet
- Instruction Manual: Slit Lamp Bon SL-EDocument20 pagesInstruction Manual: Slit Lamp Bon SL-EVladimir LevchenkoNo ratings yet
- Bibliography and FootnotesDocument2 pagesBibliography and FootnotesHannah de VeraNo ratings yet
- 12 ĀnurũpyenaDocument7 pages12 ĀnurũpyenashuklahouseNo ratings yet
- Of Personality Traits of Only and Sibling School Children in BeijingDocument14 pagesOf Personality Traits of Only and Sibling School Children in BeijingMuhammad Hamza AsgharNo ratings yet
- Literature Review On Parking SpaceDocument6 pagesLiterature Review On Parking Spacefvgy6fn3100% (1)
- Statistical MethodsDocument77 pagesStatistical MethodsGuruKPO100% (1)
- Lithospheric Evolution of The Pre-And Early Andean Convergent Margin, ChileDocument29 pagesLithospheric Evolution of The Pre-And Early Andean Convergent Margin, ChileAbdiel MuñozNo ratings yet
- Chilere - Unitatile de Racire - Technical - Brochures - NX - 0152P - 0812P - EN PDFDocument72 pagesChilere - Unitatile de Racire - Technical - Brochures - NX - 0152P - 0812P - EN PDFDaniel MilosevskiNo ratings yet
- Making Women's Medicine Masculine: OxpordDocument17 pagesMaking Women's Medicine Masculine: OxpordAdolfo Baqueiro100% (1)
- Introduction To Rhetorical Analysis: Week 1Document16 pagesIntroduction To Rhetorical Analysis: Week 1Will KurlinkusNo ratings yet
- Safety Data SheetDocument7 pagesSafety Data SheetJivendra KumarNo ratings yet
- Cambridge International AS & A Level: Biology 9700/21Document18 pagesCambridge International AS & A Level: Biology 9700/21Lavanya EaswarNo ratings yet
- Executive Summary Report Julio13Document8 pagesExecutive Summary Report Julio13exxgineNo ratings yet
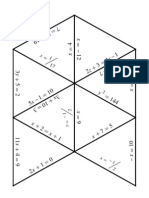
- Algebra1 Review PuzzleDocument3 pagesAlgebra1 Review PuzzleNicholas Yates100% (1)
- Systematic Literature Review SvenskaDocument6 pagesSystematic Literature Review Svenskafihum1hadej2100% (1)
- Cable Systems For High and Extra-High Voltage: Development, Manufacture, Testing, Installation and Operation of Cables and Their AccessoriesDocument1 pageCable Systems For High and Extra-High Voltage: Development, Manufacture, Testing, Installation and Operation of Cables and Their AccessorieseddisonfhNo ratings yet
- LogDocument67 pagesLogRudhi Al GhaisanNo ratings yet
- UnitPlan (P.E) Grade 6Document13 pagesUnitPlan (P.E) Grade 6Lou At CamellaNo ratings yet
- Inglês - Degrees of ComparisonDocument4 pagesInglês - Degrees of ComparisonVersehgi IINo ratings yet