You might also like
- Managing Hipertriglyceridemia in Daily PracticeDocument7 pagesManaging Hipertriglyceridemia in Daily PracticeFrillyDeyanaNo ratings yet
- Endocrinology and Metabolism Clinics-Lípidos 2009Document234 pagesEndocrinology and Metabolism Clinics-Lípidos 2009Tony Miguel Saba SabaNo ratings yet
- Documentare Pagini Facebook: - Culinaria-Sosurile KikkomanDocument5 pagesDocumentare Pagini Facebook: - Culinaria-Sosurile KikkomanLeea LeeNo ratings yet
- Nutrition Care Plan GrandmaDocument7 pagesNutrition Care Plan Grandmaapi-294693710No ratings yet
- 9983FSBH - FSBH 1 E33Document17 pages9983FSBH - FSBH 1 E33rianNo ratings yet
- Polifenoli PDFDocument15 pagesPolifenoli PDFIrinel LunguNo ratings yet
- ProjectDocument116 pagesProjectNaveen VermaNo ratings yet
- Vascular Protection Dyslipidemia: Building Healthy LifestylesDocument31 pagesVascular Protection Dyslipidemia: Building Healthy LifestylesDwi Alfian Junior HasibuanNo ratings yet
- AdaptogensDocument6 pagesAdaptogensJohnny AtmanNo ratings yet
- Hypertriglyceridemia 2012Document21 pagesHypertriglyceridemia 2012Emilia CavalittoNo ratings yet
- Small Terrors - Scorpions of The Middle EastDocument6 pagesSmall Terrors - Scorpions of The Middle EastRobert W. Lebling Jr.100% (1)
- Inflammatory Bowel Disease & Irritable Bowel Syndrome Understanding, Distinguishing and AddressingDocument20 pagesInflammatory Bowel Disease & Irritable Bowel Syndrome Understanding, Distinguishing and AddressingVas RaNo ratings yet
- JCEM Hypertriglyceridemia Endocrinology Society 2012Document36 pagesJCEM Hypertriglyceridemia Endocrinology Society 2012Paz VidaNo ratings yet
- RPB v19n1 MachoteDocument134 pagesRPB v19n1 MachoteLeonardo RomeroNo ratings yet
- Nej MR A 2216691Document15 pagesNej MR A 2216691lakshminivas PingaliNo ratings yet
- Surpass 1Document13 pagesSurpass 1Fernando DominguezNo ratings yet
- Microbial Therapeutics in Neurocognitive and Psychiatric DisordersDocument21 pagesMicrobial Therapeutics in Neurocognitive and Psychiatric Disorderssamira6alvarado6zebaNo ratings yet
- Aging Cell - 2021 - Ogrodnik - Whole Body Senescent Cell Clearance Alleviates Age Related Brain Inflammation and CognitiveDocument16 pagesAging Cell - 2021 - Ogrodnik - Whole Body Senescent Cell Clearance Alleviates Age Related Brain Inflammation and CognitiveMediatheek SGANo ratings yet
- Nutrition and Food Science Unit 3Document44 pagesNutrition and Food Science Unit 3P Harini0% (1)
- Compare and Contrast The Population Dynamic of HICs and LICsDocument9 pagesCompare and Contrast The Population Dynamic of HICs and LICsMegharashi RimjhimNo ratings yet
- Diabetes Clinical Guidelines 2018 Final PDFDocument158 pagesDiabetes Clinical Guidelines 2018 Final PDFNixon KeyaNo ratings yet
- Metabolic Syndrome PDFDocument6 pagesMetabolic Syndrome PDFVanessa HermioneNo ratings yet
- Patogenia TBCDocument49 pagesPatogenia TBCFlavia CatalinaNo ratings yet
- The Quality of Life and The EnvironmentDocument10 pagesThe Quality of Life and The Environmentlila moradoNo ratings yet
- Constructive Phases of The FastDocument53 pagesConstructive Phases of The FastRahulNo ratings yet
- Foreign Gain-of-Function Research Prevention ActDocument3 pagesForeign Gain-of-Function Research Prevention ActBrian MastNo ratings yet
- Persistent and Chronic Diarrhea and Malabsorption - ESPGHAN PDFDocument6 pagesPersistent and Chronic Diarrhea and Malabsorption - ESPGHAN PDFMoises RiveraNo ratings yet
- Introductionto Nutraceuticals MUREDZIBookDocument269 pagesIntroductionto Nutraceuticals MUREDZIBookDenise HernándezNo ratings yet
- Nutritional Considerations in Type 2 Diabetes MellitusDocument39 pagesNutritional Considerations in Type 2 Diabetes MellitusNhiNo ratings yet
- ArthAus GoutDiet 1805Document2 pagesArthAus GoutDiet 1805Nani Handayani RisandiNo ratings yet
- Diet and Thrombosis Risk: Nutrients For Prevention of Thrombotic DiseaseDocument10 pagesDiet and Thrombosis Risk: Nutrients For Prevention of Thrombotic DiseasemrsilNo ratings yet
- Clinical Practice: Ted R. Mikuls, M.D., M.S.P.HDocument11 pagesClinical Practice: Ted R. Mikuls, M.D., M.S.P.HRichy Escobar PNo ratings yet
- EMPEROR PreservedDocument38 pagesEMPEROR PreservedAppu Elias100% (1)
- Lipid MetabolismDocument15 pagesLipid MetabolismMUTHONI IRERINo ratings yet
- Rainbow DietDocument12 pagesRainbow Diet4 Bani Jain I-DNo ratings yet
- Periprocedural Anticoagulation Guidelines - UKDocument14 pagesPeriprocedural Anticoagulation Guidelines - UKjoshNo ratings yet
- Randomized, Placebo-Controlled Trial of Xyloglucan and Gelose For The Treatment of Acute Diarrhea in ChildrenDocument8 pagesRandomized, Placebo-Controlled Trial of Xyloglucan and Gelose For The Treatment of Acute Diarrhea in ChildrenvalenciaNo ratings yet
- Community Nutrition Programs in IndiaDocument10 pagesCommunity Nutrition Programs in Indiayusrah shabbirNo ratings yet
- The Difference Between Semiotics and SemDocument17 pagesThe Difference Between Semiotics and SemNora Natalia LerenaNo ratings yet
- Perioperative Management of Hyperglycemia and Diabetes in Cardiac Surgery PatientsDocument24 pagesPerioperative Management of Hyperglycemia and Diabetes in Cardiac Surgery PatientsRudi HaryantoNo ratings yet
- ArrythmiaDocument31 pagesArrythmialubnaNo ratings yet
- Nutrition in CirrhosisDocument40 pagesNutrition in CirrhosisAuliangi TamayoNo ratings yet
- A Research Proposal HshahshDocument4 pagesA Research Proposal HshahshJaqueline Magno EmraNo ratings yet
- REVIEWCOURSEDocument102 pagesREVIEWCOURSEAjay KhadkaNo ratings yet
- ST-elevation Myocardial Infarction: Straight To The Point of CareDocument238 pagesST-elevation Myocardial Infarction: Straight To The Point of CareMilagros Raysa Carhuapoma SolanoNo ratings yet
- Lipid MetabolismDocument21 pagesLipid MetabolismTooba GhummanNo ratings yet
- Science:, 1253 (2012) Henry J. Haiser and Peter J. TurnbaughDocument4 pagesScience:, 1253 (2012) Henry J. Haiser and Peter J. TurnbaughJing XueNo ratings yet
- Aph 2-Ideal CureDocument32 pagesAph 2-Ideal Cureamarkore3486No ratings yet
- Prebiotic Effect in The Healthy Infant - Recent Update: Yvan - Vandenplas@uzbrussel - BeDocument53 pagesPrebiotic Effect in The Healthy Infant - Recent Update: Yvan - Vandenplas@uzbrussel - BegazalidjawadNo ratings yet
- Curriculumguide 2324Document35 pagesCurriculumguide 2324api-331852116No ratings yet
- Fall 2 Program Guide 2022Document27 pagesFall 2 Program Guide 2022Regional YMCA of Western ConnecticutNo ratings yet
- Innovative Design of Crossflow Hydro Turbine SystemDocument11 pagesInnovative Design of Crossflow Hydro Turbine SystemrD. NgomaNo ratings yet
- The Effects of CovidDocument43 pagesThe Effects of CovidReymark LumingkitNo ratings yet
- Iron DeficiencyDocument16 pagesIron DeficiencyBobby Faisyal RakhmanNo ratings yet
- Saccharomyces Boulardii What Makes It Tick As Successful ProbioticDocument16 pagesSaccharomyces Boulardii What Makes It Tick As Successful ProbioticMonserrat Garduño Fonseca100% (1)
- Nutraceuticals For The Treatment of Hypercholesterolemia 2014 European Journal of Internal MedicineDocument8 pagesNutraceuticals For The Treatment of Hypercholesterolemia 2014 European Journal of Internal MedicineGabriel AndreescuNo ratings yet
- The Role of Diet For Prevention and Management of HTADocument6 pagesThe Role of Diet For Prevention and Management of HTAAngélica SevillaNo ratings yet
- 2 Metabolic - Syndrom - Sherling DHDocument3 pages2 Metabolic - Syndrom - Sherling DHM JNo ratings yet
- Nutrition and Stroke PreventionDocument6 pagesNutrition and Stroke PreventionNhat NamNo ratings yet
- Lifestyle Modification: Weight Control, Exercise, and Smoking CessationDocument12 pagesLifestyle Modification: Weight Control, Exercise, and Smoking CessationsenthilNo ratings yet
- X9C104PDocument11 pagesX9C104PAntonio CesarioNo ratings yet
- Gsas-Cgp Online Exam: (Sample Questions)Document10 pagesGsas-Cgp Online Exam: (Sample Questions)renrama100% (1)
- Tranformasi Pos Indonesia Menjadi Perusahaan Digital - Faizal Rochmad Djoemadi (Watermark)Document30 pagesTranformasi Pos Indonesia Menjadi Perusahaan Digital - Faizal Rochmad Djoemadi (Watermark)Anton Soco100% (5)
- DTI DirectoryDocument17 pagesDTI Directoryryan romeo perezNo ratings yet
- Gulf Cooperation Council (GCC) Sebagai OrganisasiDocument20 pagesGulf Cooperation Council (GCC) Sebagai OrganisasiBigbrother 14No ratings yet
- Samsung Company Documentary ScriptDocument9 pagesSamsung Company Documentary ScriptBunnyy BearNo ratings yet
- Assignment 1 - PROC 8170 - ENGI 91161Document2 pagesAssignment 1 - PROC 8170 - ENGI 91161latifmeijidaNo ratings yet
- L8 - Structure Functions of Various LipidsDocument23 pagesL8 - Structure Functions of Various Lipidsbilawal khanNo ratings yet
- Bussiness Plan Pasarmu Dot IdDocument25 pagesBussiness Plan Pasarmu Dot IdAnand ZidanNo ratings yet
- Problems For Proof of Cash and Bank ReconDocument2 pagesProblems For Proof of Cash and Bank ReconTine Vasiana DuermeNo ratings yet
- Frankland Tube Elect PDFDocument34 pagesFrankland Tube Elect PDFBill PerkinsNo ratings yet
- John DonneDocument27 pagesJohn Donnedunvir100% (2)
- Skin TearsDocument6 pagesSkin TearsMsPocketbook HoarderNo ratings yet
- Hill PPT 13e chp01Document40 pagesHill PPT 13e chp01tatischanho61No ratings yet
- Welcome To: Cooling Water Treatment in Power Plants Recent Trends & Case StudyDocument17 pagesWelcome To: Cooling Water Treatment in Power Plants Recent Trends & Case StudyrpshvjuNo ratings yet
- LogDocument15 pagesLogAngelo VillarNo ratings yet
- EM-Log Sensor FNF I, Types 4040 and 4726 and Preamplifier E, Type 2863 For Electromagnetic Speed Log Systems Naviknot 350 E / 350 EeDocument48 pagesEM-Log Sensor FNF I, Types 4040 and 4726 and Preamplifier E, Type 2863 For Electromagnetic Speed Log Systems Naviknot 350 E / 350 EeGary Gouveia100% (1)
- OMSB Online Residency Application: Physician Applicant Registration TutorialDocument14 pagesOMSB Online Residency Application: Physician Applicant Registration TutorialWayne GonsalvesNo ratings yet
- Current Pharmaceutical & Clinical Research: An Overview On ImmunomodulatorsDocument7 pagesCurrent Pharmaceutical & Clinical Research: An Overview On ImmunomodulatorsElly Eliza100% (1)
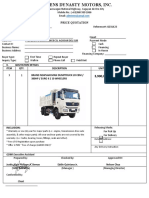
- Price Quotation Shacman H3000 Dump TruckDocument1 pagePrice Quotation Shacman H3000 Dump TruckJustin BernasNo ratings yet
- Gibberish WordsDocument4 pagesGibberish WordsDaniel PopaNo ratings yet
- Balloons and Airships, 1783-197Document120 pagesBalloons and Airships, 1783-197LauraMujdei100% (1)
- User's Manual of Haiwell IoT Cloud HMIDocument39 pagesUser's Manual of Haiwell IoT Cloud HMIRolando NuñezNo ratings yet
- Week 3 MethodsofphilosophizingDocument30 pagesWeek 3 MethodsofphilosophizingShen EugenioNo ratings yet
- TDA1553QDocument10 pagesTDA1553QahmedNo ratings yet
- (SAP) Connector enDocument114 pages(SAP) Connector ensreehana03No ratings yet
- CURRY, Patrick VOSS, Angela. Seeing With Different Eyes - Essays in Astrology and Divination (2007, Cambridge Scholars Publishing) PDFDocument364 pagesCURRY, Patrick VOSS, Angela. Seeing With Different Eyes - Essays in Astrology and Divination (2007, Cambridge Scholars Publishing) PDFRoland100% (1)
- Merck Agency Theory Instructional Case Pages 1 14Document14 pagesMerck Agency Theory Instructional Case Pages 1 14Renuka PrasadNo ratings yet
- IntellectualDocument32 pagesIntellectualChicken Feet Gang86% (7)
- 6662 - ARB - Nurlia Rizky Andri S - 21904101038 - Reza Rahma Tazkia - 21904101039Document4 pages6662 - ARB - Nurlia Rizky Andri S - 21904101038 - Reza Rahma Tazkia - 21904101039Reza Rahma TazkiaNo ratings yet