You might also like
- Implementation of EMRs, NigeriaDocument17 pagesImplementation of EMRs, NigeriaAsmamaw K.No ratings yet
- EHR For ResearchDocument6 pagesEHR For ResearchAsmamaw K.No ratings yet
- Paradigms ResearchDocument1 pageParadigms ResearchAsmamaw K.No ratings yet
- Evolution and Challenges of EMRDocument3 pagesEvolution and Challenges of EMRAsmamaw K.No ratings yet
- Actual Usage of EMRs in CanadaDocument2 pagesActual Usage of EMRs in CanadaAsmamaw K.No ratings yet
- EMR - Access, Sharing and ConfidentialityDocument40 pagesEMR - Access, Sharing and ConfidentialityAsmamaw K.No ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Concept of Lokmitra Kendra in Himachal PradeshDocument2 pagesConcept of Lokmitra Kendra in Himachal PradeshSureshSharmaNo ratings yet
- College of Engineering Cagayan State UniversityDocument16 pagesCollege of Engineering Cagayan State UniversityErika Antonio GutierrezNo ratings yet
- THE BASIC TYPES OF SPEECHES PPTDocument14 pagesTHE BASIC TYPES OF SPEECHES PPTKevin BanezNo ratings yet
- I. Objectives Ii. Content Iii. Learning ResourcesDocument13 pagesI. Objectives Ii. Content Iii. Learning ResourcesZenia CapalacNo ratings yet
- FPGA Implementation For Humidity and Temperature Remote Sensing SystemDocument5 pagesFPGA Implementation For Humidity and Temperature Remote Sensing SystemteekamNo ratings yet
- Most Dangerous City - Mainstreet/Postmedia PollDocument35 pagesMost Dangerous City - Mainstreet/Postmedia PollTessa VanderhartNo ratings yet
- Fiedler1950 - A Comparison of Therapeutic Relationships in PsychoanalyticDocument10 pagesFiedler1950 - A Comparison of Therapeutic Relationships in PsychoanalyticAnca-Maria CovaciNo ratings yet
- Biography Worksheet: Name: Gerardo Angeles MartinezDocument1 pageBiography Worksheet: Name: Gerardo Angeles MartinezAlejandro AngelesNo ratings yet
- Admission: North South University (NSU) Question Bank Summer 2019Document10 pagesAdmission: North South University (NSU) Question Bank Summer 2019Mahmoud Hasan100% (7)
- WicDocument6 pagesWicGonzalo Humberto RojasNo ratings yet
- 2011 Frequency AllocationsDocument1 page2011 Frequency Allocationsculeros1No ratings yet
- n4 HandoutDocument2 pagesn4 HandoutFizzerNo ratings yet
- Ib Psychology - Perfect Saq Examination Answers PDFDocument2 pagesIb Psychology - Perfect Saq Examination Answers PDFzeelaf siraj0% (2)
- 74 Series Logic ICsDocument6 pages74 Series Logic ICsanon-466841No ratings yet
- Application Letter For Promotion T2 T3Document24 pagesApplication Letter For Promotion T2 T3FGacadSabadoNo ratings yet
- Performance Comparison of VxWorks Linux RTAI and Xenomai in A Hard Real-Time ApplicationDocument5 pagesPerformance Comparison of VxWorks Linux RTAI and Xenomai in A Hard Real-Time ApplicationsatyanaryanakNo ratings yet
- Unit 3Document5 pagesUnit 3Narasimman DonNo ratings yet
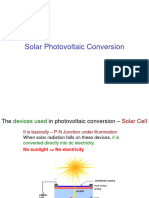
- Slide 7 PV NewDocument74 pagesSlide 7 PV NewPriyanshu AgrawalNo ratings yet
- 3DD5036 Horizontal.2Document6 pages3DD5036 Horizontal.2routerya50% (2)
- Powerplant QuestionsDocument19 pagesPowerplant QuestionsAshok KumarNo ratings yet
- Ateneo de Naga University: Professional Training For Teacher 4.0Document10 pagesAteneo de Naga University: Professional Training For Teacher 4.0Rosemarie BrionesNo ratings yet
- CNC Milling ReportDocument15 pagesCNC Milling ReportStarscream Aisyah78% (37)
- Solutions of Inverse Geodetic Problem in Navigational Applications PDFDocument5 pagesSolutions of Inverse Geodetic Problem in Navigational Applications PDFLacci123No ratings yet
- Manitou 1350RDocument4 pagesManitou 1350RcandlaganNo ratings yet
- GL Career Academy Data AnalyticsDocument7 pagesGL Career Academy Data AnalyticsDeveloper GuideNo ratings yet
- GE Uno Downlight Backlit BLDocument2 pagesGE Uno Downlight Backlit BLChen KengloonNo ratings yet
- Dissertation MA History PeterRyanDocument52 pagesDissertation MA History PeterRyaneNo ratings yet
- Surge Protection Devices CatalogueDocument134 pagesSurge Protection Devices CatalogueNguyen Doan QuyetNo ratings yet
- World English 2ed 1 WorkbookDocument80 pagesWorld English 2ed 1 WorkbookMatheus EdneiNo ratings yet
- ALTS150-12P Datasheet1Document2 pagesALTS150-12P Datasheet1mamloveNo ratings yet