You might also like
- State of The Global Workplace 2021 DownloadDocument191 pagesState of The Global Workplace 2021 DownloadRichard PhoenixNo ratings yet
- Rockford Whitman Interchange ProjectDocument8 pagesRockford Whitman Interchange ProjectShane NicholsonNo ratings yet
- ITAC 100 Implementation Guide For SAP (V2012)Document154 pagesITAC 100 Implementation Guide For SAP (V2012)Othmane Ferroukhi100% (3)
- Otherworld Miniatures - Otherworld Fantasy SkirmishDocument138 pagesOtherworld Miniatures - Otherworld Fantasy SkirmishAlexander Missirian89% (9)
- The Lord of The Rings MapsDocument6 pagesThe Lord of The Rings Mapsapi-3713690100% (1)
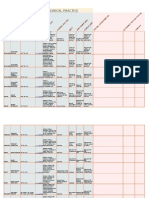
- Goniometry For Clinical PracticeDocument7 pagesGoniometry For Clinical Practicedramitsaini33% (3)
- Fundamentals Strategic Management Navas & Guerras 2013Document18 pagesFundamentals Strategic Management Navas & Guerras 2013Pedro AlmeidaNo ratings yet
- Chapter: Percentage Class WorkDocument6 pagesChapter: Percentage Class WorkRajat GuptaNo ratings yet
- Aborginal Artisan Catalogue Fourth EditionDocument127 pagesAborginal Artisan Catalogue Fourth EditionAndreas D.No ratings yet
- 4495 Tech of Sound Repro Amplifiers PDFDocument268 pages4495 Tech of Sound Repro Amplifiers PDFimrefodorNo ratings yet
- Summer 2020 Strong Runs Newsletter Native Fish SocietyDocument20 pagesSummer 2020 Strong Runs Newsletter Native Fish SocietyMark P. SherwoodNo ratings yet
- Inbar Bru-3-2 en PDFDocument32 pagesInbar Bru-3-2 en PDFSepanta AbdolahpourNo ratings yet
- The Agriculturalist - Jan-Feb 2023Document24 pagesThe Agriculturalist - Jan-Feb 2023Patrick MaitlandNo ratings yet
- HortFlora Research Spectrum, Vol. 2 (1) 2013Document98 pagesHortFlora Research Spectrum, Vol. 2 (1) 2013HortFlora Research SpectrumNo ratings yet
- Marshall 'Blues Breaker': Manual & Assembly GuideDocument27 pagesMarshall 'Blues Breaker': Manual & Assembly GuideAndre OliveiraNo ratings yet
- Royal Commission On Aboriginal PeoplesDocument3,347 pagesRoyal Commission On Aboriginal PeoplesTessa VanderhartNo ratings yet
- Chanute 1983 StudyDocument190 pagesChanute 1983 StudyWashington BureauNo ratings yet
- List of Brand Names and Compostion of Banned DrugsDocument30 pagesList of Brand Names and Compostion of Banned DrugsUdhayakumar VenkataramanNo ratings yet
- Digital modeling of vacuum tube guitar amplifiersDocument16 pagesDigital modeling of vacuum tube guitar amplifiersΔημήτρης ΓκρίντζοςNo ratings yet
- Wwi Who Is To Blame DocumentsDocument7 pagesWwi Who Is To Blame Documentsapi-277818830No ratings yet
- 2022 Capital Outlay Projects by CountyDocument29 pages2022 Capital Outlay Projects by CountyAlgernon D'AmmassaNo ratings yet
- Mi KmaqDocument1 pageMi KmaqBMikeNo ratings yet
- United States v. Frank Church, Carl Louis Coppola, 955 F.2d 688, 11th Cir. (1992)Document24 pagesUnited States v. Frank Church, Carl Louis Coppola, 955 F.2d 688, 11th Cir. (1992)Scribd Government DocsNo ratings yet
- Module 3.trick or Treaty - FINAL PDFDocument31 pagesModule 3.trick or Treaty - FINAL PDFseektherunes24100% (1)
- Seeking The Magic Mushroom Life Magazine 1957Document12 pagesSeeking The Magic Mushroom Life Magazine 1957rebelznNo ratings yet
- Rosin-Rammler Regression from Sieve DataDocument6 pagesRosin-Rammler Regression from Sieve DataRajeshkumar ElangoNo ratings yet
- Primary Petitions 2021Document17 pagesPrimary Petitions 2021News10NBCNo ratings yet
- Handwired HBK ALLDocument49 pagesHandwired HBK ALLtano2265No ratings yet
- Subwoofer: HistoryDocument30 pagesSubwoofer: HistoryRoberto Ortega MicalizziNo ratings yet
- Guitar Electromagnetic InductionDocument5 pagesGuitar Electromagnetic InductionartheriskNo ratings yet
- KEMPER PROFILER Addendum 5.7 (English) PDFDocument145 pagesKEMPER PROFILER Addendum 5.7 (English) PDFAlberto BolocanNo ratings yet
- 2020 Os 3105Document4 pages2020 Os 3105jcdomingo75No ratings yet
- 10-082-01 NEC Brochure ENG MyCalls LRDocument12 pages10-082-01 NEC Brochure ENG MyCalls LRRavneel Kant SharmaNo ratings yet
- Cen-Cenelec WP 2020 enDocument104 pagesCen-Cenelec WP 2020 enSabri GünaydınNo ratings yet
- Unit 7: Extra PracticeDocument12 pagesUnit 7: Extra PracticeVictor PlataNo ratings yet
- Stock prices over timeDocument1 pageStock prices over timeJefferson Auqui OtarolaNo ratings yet
- Industry: The Industrial Sector Over The YearsDocument18 pagesIndustry: The Industrial Sector Over The YearsRon 61No ratings yet
- So 1Document1 pageSo 1MOHAMMED NEHALNo ratings yet
- UPDATE: Whitman Street Interchange ReconfigurationDocument8 pagesUPDATE: Whitman Street Interchange ReconfigurationJeff Kolkey100% (1)
- EG2014 02 Area05-SDocument1 pageEG2014 02 Area05-SMani packageNo ratings yet
- TW-88 Storm Conduit Plan and ProfileDocument5 pagesTW-88 Storm Conduit Plan and Profileinam khanNo ratings yet
- Jr. Miguel Grau: Colegio NacionalDocument1 pageJr. Miguel Grau: Colegio NacionalJhinno MorenoNo ratings yet
- SDR hpch3Document6 pagesSDR hpch3Shubham SharmaNo ratings yet
- Architectural Drawing - OrmocDocument14 pagesArchitectural Drawing - OrmocJin Lee ChuNo ratings yet
- 2009 10 Marguerite MapDocument1 page2009 10 Marguerite Mapaditya81No ratings yet
- SDR hpch5Document28 pagesSDR hpch5Shubham SharmaNo ratings yet
- FILIPO CompressedDocument1 pageFILIPO CompressedCarolina CarrascoNo ratings yet
- Rural Development: Pme NTDocument24 pagesRural Development: Pme NTcool ishanNo ratings yet
- ¿Cómo Te Llamas?: Me LlamøDocument12 pages¿Cómo Te Llamas?: Me LlamøjohnsmithperthNo ratings yet
- Placement 2009Document62 pagesPlacement 2009vipul_patel100% (12)
- 2020 Bird Barrier CatalogDocument64 pages2020 Bird Barrier Cataloggesap35224No ratings yet
- Lake Evendim: A Lost Realm of EnchantmentDocument6 pagesLake Evendim: A Lost Realm of EnchantmentWalter FernándezNo ratings yet
- Pieces of Middle-Earth MapsDocument6 pagesPieces of Middle-Earth Mapserdemsahin55100% (3)
- Lindon: H A RLDocument6 pagesLindon: H A RLGxilleNo ratings yet
- Nwmecampaignmapbw PDFDocument6 pagesNwmecampaignmapbw PDFlocobardoNo ratings yet
- Lindon: H A RLDocument6 pagesLindon: H A RLChristian VikströmNo ratings yet
- Structures Project: Typical Floor Beam LayoutDocument1 pageStructures Project: Typical Floor Beam LayoutAlekhya DeviNo ratings yet
- SDR hpch4Document12 pagesSDR hpch4Shubham SharmaNo ratings yet
- 12 Pearl WiDocument10 pages12 Pearl Wijecelyn mae BaluroNo ratings yet
- EMSL Commercial Lab Services GuideDocument73 pagesEMSL Commercial Lab Services Guideshahriermahmud17No ratings yet
- Selasar Dakwah: Area Drop OFFDocument1 pageSelasar Dakwah: Area Drop OFFMuhammad Irhash MaulanaNo ratings yet
- Introducción: WWW - Edinumen.es WWW - Edinumen.es WWW - Edinumen.esDocument5 pagesIntroducción: WWW - Edinumen.es WWW - Edinumen.es WWW - Edinumen.esjohnsmithperthNo ratings yet
- Solution Manual For Strategic Management A Competitive Advantage Approach Concepts Cases 15 e 15th Edition Fred R David Forest R DavidDocument13 pagesSolution Manual For Strategic Management A Competitive Advantage Approach Concepts Cases 15 e 15th Edition Fred R David Forest R DavidChristinaVillarrealfdqs100% (45)
- Business FinanceDocument8 pagesBusiness FinanceChristine Marie ViscaynoNo ratings yet
- A Study The Compatative of Income Tax For Partnership Firm With Reference To KDMC AreaDocument49 pagesA Study The Compatative of Income Tax For Partnership Firm With Reference To KDMC AreaTasmay EnterprisesNo ratings yet
- Sample Partnership DeedDocument4 pagesSample Partnership DeedShahzad Faisal0% (1)
- Software Product Launch Plan TemplateDocument6 pagesSoftware Product Launch Plan TemplateShady Mohamed El-KhattabyNo ratings yet
- Auditing Problems - 001Document2 pagesAuditing Problems - 001Geoff MacarateNo ratings yet
- Amazon Supply ChainDocument18 pagesAmazon Supply Chainyatendra13288100% (2)
- Crisis Management Final Examination: "PT. Freeport Indonesia Big Gossan Collapsed"Document16 pagesCrisis Management Final Examination: "PT. Freeport Indonesia Big Gossan Collapsed"PavelBondarNo ratings yet
- HR Examiner's Guide to Free Speech at WorkDocument10 pagesHR Examiner's Guide to Free Speech at WorkShiba LodhiNo ratings yet
- PayU Case StudyDocument7 pagesPayU Case Studyajit jogiNo ratings yet
- LEGAL DOSSIER AND LEGAL DOCUMENT IN ENGLISHDocument58 pagesLEGAL DOSSIER AND LEGAL DOCUMENT IN ENGLISHCristian Silva TapiaNo ratings yet
- Asset Location Classification: StandardDocument45 pagesAsset Location Classification: Standardmsaadi717No ratings yet
- Willaware vs Jesichris unfair competition caseDocument1 pageWillaware vs Jesichris unfair competition caseLawiswisNo ratings yet
- Buisness StrategyDocument3 pagesBuisness Strategyrajaroma45No ratings yet
- Updated Blaw Past Papers by RNK-1Document90 pagesUpdated Blaw Past Papers by RNK-1muzamil azizNo ratings yet
- Hair Oil PresentationDocument12 pagesHair Oil Presentationmohan_ved02550% (2)
- TS Grewal Class 11 Accountancy Solutions Chapter 7Document10 pagesTS Grewal Class 11 Accountancy Solutions Chapter 7Vishek kashyap 10 A1 22No ratings yet
- Case DigestsDocument48 pagesCase DigestsHazel Reyes-AlcantaraNo ratings yet
- 39 Different Types of Candlesticks PatternsDocument47 pages39 Different Types of Candlesticks Patternspritesh.tiwariNo ratings yet
- Chapter 5 SolutionDocument47 pagesChapter 5 SolutionJay-PNo ratings yet
- Chapter 9 Caselette Audit of SheDocument26 pagesChapter 9 Caselette Audit of SheBusiness MatterNo ratings yet
- Bank Of Punjab Internship ReportDocument49 pagesBank Of Punjab Internship ReportHussain HadiNo ratings yet
- PUMBA - DSE A - 506 - LDIM - 1.1 Nature and Scope of International Trade Law - PPTDocument34 pagesPUMBA - DSE A - 506 - LDIM - 1.1 Nature and Scope of International Trade Law - PPTTô Mì HakkaNo ratings yet
- Consent LetterDocument1 pageConsent LetterSai KiranNo ratings yet
- VCM Questions PrelimsDocument15 pagesVCM Questions Prelimsnatalie clyde matesNo ratings yet
- Store-Officer-1 QuestionDocument58 pagesStore-Officer-1 QuestionJayakumar VkNo ratings yet
- BF2 - AnswerDocument34 pagesBF2 - AnswerCherielee FabroNo ratings yet