You might also like
- NURS FPX4020 ChiuAmanda Assessment4 1Document14 pagesNURS FPX4020 ChiuAmanda Assessment4 1brinju brianNo ratings yet
- New FIDIC Gold Book Contract GuideDocument4 pagesNew FIDIC Gold Book Contract GuideJama 'Figo' MustafaNo ratings yet
- CH2M EAC EstimateAtCompletionPolicyDocument5 pagesCH2M EAC EstimateAtCompletionPolicynparlance100% (1)
- Communications T-R ManualDocument213 pagesCommunications T-R Manualjahaha100% (1)
- CPOE Systems Success Factors and Implementation IssuesDocument10 pagesCPOE Systems Success Factors and Implementation IssuesRicky ChanNo ratings yet
- Pharmacy Education Article Page 107Document42 pagesPharmacy Education Article Page 107Cristine ChubiboNo ratings yet
- The ROI of Data Loss Prevention: A Websense White PaperDocument16 pagesThe ROI of Data Loss Prevention: A Websense White PaperAdoliu AlexandruNo ratings yet
- Credit Risk QuestionnaireDocument4 pagesCredit Risk QuestionnaireBhaumik Nayak100% (1)
- Imprtant Projects For Six Sigma HospitalDocument12 pagesImprtant Projects For Six Sigma Hospitalشادي الاخرسNo ratings yet
- Hewison NURSES IDENTIFICATION AND REPORTING OF MEDICATION ERRORS Journal Clinical NursingDocument17 pagesHewison NURSES IDENTIFICATION AND REPORTING OF MEDICATION ERRORS Journal Clinical NursingCatrin_HutaurukNo ratings yet
- Evaluating The Application of Failure Mode and Effects Analysis Technique in Hospital Wards: A Systematic ReviewDocument10 pagesEvaluating The Application of Failure Mode and Effects Analysis Technique in Hospital Wards: A Systematic ReviewManuel MesaNo ratings yet
- Jamda: Ali Azeez Al-Jumaili Bs Pharm, MS, William R. Doucette PHDDocument19 pagesJamda: Ali Azeez Al-Jumaili Bs Pharm, MS, William R. Doucette PHDIstyNo ratings yet
- Fmea DispensingDocument13 pagesFmea DispensingFARMASI KLINISNo ratings yet
- 2000, Antonow J. Medication Error Reporting PediatriaDocument7 pages2000, Antonow J. Medication Error Reporting PediatriaFilipa Salvador SalvadorNo ratings yet
- Literature Review Medication ErrorDocument7 pagesLiterature Review Medication Errorfohudenyfeh2100% (1)
- Evidence Based Practice Medication ErrorsDocument6 pagesEvidence Based Practice Medication Errorsapi-302591810No ratings yet
- Improving Patient Safety Through Human-Factor-Based Risk ManagementDocument8 pagesImproving Patient Safety Through Human-Factor-Based Risk ManagementDessy TrisariNo ratings yet
- Abostrofic SytosisDocument17 pagesAbostrofic Sytosisasaad biqaiNo ratings yet
- Barriers and Facilitators of Nursing Error Reporting: Literature Review Ahmed Raja, RN-BSN Student Al Quds University May 2017Document30 pagesBarriers and Facilitators of Nursing Error Reporting: Literature Review Ahmed Raja, RN-BSN Student Al Quds University May 2017مالك مناصرةNo ratings yet
- PSJ - Volume 8 - Issue 1 - Pages 13-23Document11 pagesPSJ - Volume 8 - Issue 1 - Pages 13-23mauliana mardhira fauzaNo ratings yet
- Ori Stojkovic2017Document9 pagesOri Stojkovic2017Nur LaelaNo ratings yet
- Medication Error Factors, Safety Guideline System, Flow of Drug Usage, and Code of Conduct To Prevent Medication ErrorDocument5 pagesMedication Error Factors, Safety Guideline System, Flow of Drug Usage, and Code of Conduct To Prevent Medication ErrorskyNo ratings yet
- 20-4 EditedDocument13 pages20-4 EditedElizabeth GithinjiNo ratings yet
- Pharm Paper FinalDocument8 pagesPharm Paper FinalAnamta AkhtarNo ratings yet
- Minimizing Medication Errors Practical Pointers For PrescribersDocument4 pagesMinimizing Medication Errors Practical Pointers For PrescribersLuciana OliveiraNo ratings yet
- NHS-FPX 4000 Applying Library Research SkillsDocument7 pagesNHS-FPX 4000 Applying Library Research SkillsIrene WafulaNo ratings yet
- Literature Review Medication ErrorsDocument4 pagesLiterature Review Medication Errorsea5zjs6a100% (2)
- Terms Used in Patient Safety Related To Medication A Literature ReviewDocument5 pagesTerms Used in Patient Safety Related To Medication A Literature ReviewckkuzaxgfNo ratings yet
- Jcs 9 1Document8 pagesJcs 9 1kristina dewiNo ratings yet
- Almutary, Hayfa Lewis, Peter: C WilkinsDocument19 pagesAlmutary, Hayfa Lewis, Peter: C Wilkinsمالك مناصرةNo ratings yet
- The Impact of Health Information Technology On Patient SafetyDocument13 pagesThe Impact of Health Information Technology On Patient SafetySaba Abu FarhaNo ratings yet
- Safety and Health at Work: Original ArticleDocument7 pagesSafety and Health at Work: Original ArticleIffa Masruroh2No ratings yet
- Prevalence and Risk Factors of Self-Reported Financial Toxicity in Cancer Survivors A Systematic Review and Meta-AnalysesDocument19 pagesPrevalence and Risk Factors of Self-Reported Financial Toxicity in Cancer Survivors A Systematic Review and Meta-Analysesmrezab1987No ratings yet
- 36470-Article Text-103101-1-10-20200819Document10 pages36470-Article Text-103101-1-10-20200819Tuti DamNo ratings yet
- Patient Safety and Medical ErrorsDocument8 pagesPatient Safety and Medical ErrorsVũ Tuấn TùngNo ratings yet
- Preventing Medication ErrorsDocument26 pagesPreventing Medication ErrorsmrkianzkyNo ratings yet
- Development of A List of High-Risk Perioperative Medications For The Elderly: A Delphi MethodDocument8 pagesDevelopment of A List of High-Risk Perioperative Medications For The Elderly: A Delphi Methodfabian arassiNo ratings yet
- 2019 - Härkänen Et AlDocument8 pages2019 - Härkänen Et AlazeemathmariyamNo ratings yet
- Dionne, 2022 - Which Pharmacists Are Performing Antimicrobial StewardshipDocument7 pagesDionne, 2022 - Which Pharmacists Are Performing Antimicrobial StewardshipThuane SalesNo ratings yet
- EBP Deliverable Module 2Document6 pagesEBP Deliverable Module 2Marian SmithNo ratings yet
- Principle of Medication SafetyDocument8 pagesPrinciple of Medication SafetyChakra PuspitaNo ratings yet
- Medication ErrorsDocument7 pagesMedication ErrorsNelly CheptooNo ratings yet
- Failure Mode and Effects Analysis Drastically Reduced Potential Risks in Clinical Trial ConductDocument10 pagesFailure Mode and Effects Analysis Drastically Reduced Potential Risks in Clinical Trial Conduct2023hb74041No ratings yet
- Relationship Between Patients Perceptions of Care.3Document9 pagesRelationship Between Patients Perceptions of Care.3inno semuNo ratings yet
- Computer Simulation and Six-Sigma Tools Applied To Process Improvement in An Emergency DepartmentDocument0 pagesComputer Simulation and Six-Sigma Tools Applied To Process Improvement in An Emergency DepartmentdeepakjothivelNo ratings yet
- Assessment of Patient Safety Culture Among Doctors Nurses and Midwives in A Public Hospital in AfghanistanDocument8 pagesAssessment of Patient Safety Culture Among Doctors Nurses and Midwives in A Public Hospital in Afghanistantsa638251No ratings yet
- Categorizing and Understanding Medication Errors in Hospital Pharmacy in Relation To Human FactorsDocument12 pagesCategorizing and Understanding Medication Errors in Hospital Pharmacy in Relation To Human FactorskhhhhhNo ratings yet
- Literature Review On Medication Administration ErrorsDocument7 pagesLiterature Review On Medication Administration Errorsea2167raNo ratings yet
- Jurnal Medical SafetyDocument14 pagesJurnal Medical SafetyMARWAH MARWAHNo ratings yet
- Chapter 12 - Patient Safety - APIC Text OnlineDocument30 pagesChapter 12 - Patient Safety - APIC Text OnlineManalAbdelazizNo ratings yet
- Novel Feature Reduction (NFR) Model With Machine Learning and Data Mining Algorithms For Effective Disease Risk PredictionDocument22 pagesNovel Feature Reduction (NFR) Model With Machine Learning and Data Mining Algorithms For Effective Disease Risk Predictioncse bNo ratings yet
- Practice Standard Safety & QualityDocument2 pagesPractice Standard Safety & Qualityssreya80No ratings yet
- Factors Affecting Medication Errors From The Perspective of Nursing StaffDocument5 pagesFactors Affecting Medication Errors From The Perspective of Nursing Staffjose romeroNo ratings yet
- ArticleDocument14 pagesArticlechavadgeniferNo ratings yet
- Review of Related LiteratureDocument6 pagesReview of Related LiteratureRona CabanyogNo ratings yet
- EBMgt 1Document8 pagesEBMgt 1Delelegn EmwodewNo ratings yet
- Incidence, Causes, and Consequences of Preventable Adverse Drug Reactions Occurring in Inpatients - A Systematic Review of Systematic Reviews - PMCDocument39 pagesIncidence, Causes, and Consequences of Preventable Adverse Drug Reactions Occurring in Inpatients - A Systematic Review of Systematic Reviews - PMCimyours9601No ratings yet
- Increasing Adverse Drug Reaction Reporting-How Can We Do BetterDocument15 pagesIncreasing Adverse Drug Reaction Reporting-How Can We Do Betterstacie010429No ratings yet
- 11 ArticuloDocument9 pages11 ArticuloNia MoonNo ratings yet
- CF Rca TemplateDocument8 pagesCF Rca TemplateEsteban García EcheverryNo ratings yet
- 67-1426444406 FinalPublishedVersion PDFDocument16 pages67-1426444406 FinalPublishedVersion PDFSandi BongNo ratings yet
- Jurnal Manajemen Pelayanan Kesehatan: Artikel PenelitianDocument6 pagesJurnal Manajemen Pelayanan Kesehatan: Artikel PenelitiankevinrestuNo ratings yet
- Multifunctional Medication Mishap Rca 1Document4 pagesMultifunctional Medication Mishap Rca 1MUNSIF JAWEEDNo ratings yet
- Assessment of Healthcare Professional Awareness Towards Haemovigilance (HvPI) Programme of India in South IndiaDocument5 pagesAssessment of Healthcare Professional Awareness Towards Haemovigilance (HvPI) Programme of India in South IndiaIOSRjournalNo ratings yet
- Clinical Decision Support System: Fundamentals and ApplicationsFrom EverandClinical Decision Support System: Fundamentals and ApplicationsNo ratings yet
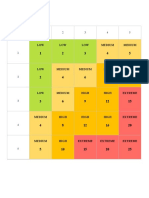
- 5X5 Risk Matrix: LOW LOW LOW Medium MediumDocument2 pages5X5 Risk Matrix: LOW LOW LOW Medium MediumasiyahNo ratings yet
- Risk Management Matrix Template: Acceptable Improbable Acceptable Improbable Tolerable Possible Acceptable ImprobableDocument3 pagesRisk Management Matrix Template: Acceptable Improbable Acceptable Improbable Tolerable Possible Acceptable ImprobableasiyahNo ratings yet
- Risk Evaluation in Failure Mode and Effects Analysis Based On D Numbers TheoryDocument20 pagesRisk Evaluation in Failure Mode and Effects Analysis Based On D Numbers TheoryasiyahNo ratings yet
- 19359-Article Text-35906-1-10-20181211Document18 pages19359-Article Text-35906-1-10-20181211asiyahNo ratings yet
- Medication Safety Strategies in Hospitals - A Systematic ReviewDocument17 pagesMedication Safety Strategies in Hospitals - A Systematic ReviewasiyahNo ratings yet
- FentimansDocument0 pagesFentimanszhenglin0620_2205311No ratings yet
- Risk Assesment For GRP Pipe LayingDocument3 pagesRisk Assesment For GRP Pipe LayingSasi Kumar50% (4)
- Adam Khoo - Get Out of The Rat RaceDocument17 pagesAdam Khoo - Get Out of The Rat RaceRian Kurniawan100% (2)
- 448199Document40 pages448199薇艾No ratings yet
- RISK SHARING IN ISLAMIC FINANCE@UniklDocument20 pagesRISK SHARING IN ISLAMIC FINANCE@UniklLee WongNo ratings yet
- Procedure For HSE Risk Assessments: Suez Oil CompanyDocument13 pagesProcedure For HSE Risk Assessments: Suez Oil Companyeng20072007No ratings yet
- 1-EA in Online GamingDocument2 pages1-EA in Online GamingCharan CvNo ratings yet
- E Ects of The Antibiotics Oxytetracycline and Tylosin On Soil FaunaDocument7 pagesE Ects of The Antibiotics Oxytetracycline and Tylosin On Soil FaunaCarolina Ivon Inostroza HuaracànNo ratings yet
- Deloitte 2016 MADIIMARDocument21 pagesDeloitte 2016 MADIIMARCarlos Belando PastorNo ratings yet
- Wyn032 PDFDocument21 pagesWyn032 PDFWahjudi MuhammadNo ratings yet
- FM Systems Req For Use ISO 41001Document56 pagesFM Systems Req For Use ISO 41001Mohamed ShaabanNo ratings yet
- James Montier - Darwin's Mind: The Evolutionary Foundations of Heuristics and BiasesDocument31 pagesJames Montier - Darwin's Mind: The Evolutionary Foundations of Heuristics and BiasesRaviNo ratings yet
- Risk Management For Projects: Course SyllabusDocument4 pagesRisk Management For Projects: Course Syllabusfreanne_0527No ratings yet
- Risk Assessment For Stone Works: Project NameDocument7 pagesRisk Assessment For Stone Works: Project NameharikrishnaNo ratings yet
- EVENT RISK MGT Full UnitDocument47 pagesEVENT RISK MGT Full Unitjivay33362No ratings yet
- Ebp 650 - 2Document52 pagesEbp 650 - 2Lau AlexNo ratings yet
- Writing Assigment Unit 1 - BUS 5611 - PW - JadiDocument4 pagesWriting Assigment Unit 1 - BUS 5611 - PW - JadiMohamed HelmyNo ratings yet
- Insurance Smart Sampoorna RakshaDocument11 pagesInsurance Smart Sampoorna RakshaRajashekar Reddy SamaNo ratings yet
- HIRACDocument21 pagesHIRACPutera Kd100% (4)
- ADEC EHSMS Handbook V.01-2011-F-E PDFDocument32 pagesADEC EHSMS Handbook V.01-2011-F-E PDFmd sarfaraz khanNo ratings yet
- Luthans10e TB Ch10Document31 pagesLuthans10e TB Ch10Hernan Ochoa MontesNo ratings yet
- Hirarc JKKP ClosingDocument40 pagesHirarc JKKP ClosingThegym le Greene100% (1)
- (25082020 1353) Highfield Level 1 Award in Health and Safety Awareness Qualification Specification v1 August 2020Document11 pages(25082020 1353) Highfield Level 1 Award in Health and Safety Awareness Qualification Specification v1 August 2020NISARNo ratings yet
- Company ProfileDocument4 pagesCompany ProfileArcangel Protection Services100% (1)
- Accident PreventionDocument17 pagesAccident Preventione cubeNo ratings yet