You might also like
- Shanz - Pedia 1.04Document8 pagesShanz - Pedia 1.04Petrina XuNo ratings yet
- Embryology of The EarDocument3 pagesEmbryology of The EarJem MontañaNo ratings yet
- Dengue Virus: DescriptionDocument12 pagesDengue Virus: Descriptionpedia blue bookNo ratings yet
- TRANS - Pediatric Patient ProblemsDocument4 pagesTRANS - Pediatric Patient ProblemsRencel Hope Bañez100% (1)
- Case On Upper GI Bleeding: Interns Chua, EsquidaDocument59 pagesCase On Upper GI Bleeding: Interns Chua, EsquidaJoyce ChuaNo ratings yet
- Pedia Bacte Table 08amDocument25 pagesPedia Bacte Table 08ampedia blue bookNo ratings yet
- PEDIA para 08AMDocument17 pagesPEDIA para 08AMpedia blue bookNo ratings yet
- Internal Medicine - Nephrology: Topic: Cystic Kidney Diseases Lecturer: Dra. Myrna NgoDocument3 pagesInternal Medicine - Nephrology: Topic: Cystic Kidney Diseases Lecturer: Dra. Myrna NgoVon HippoNo ratings yet
- 01-05-21 - 01-12-21 - Fluid & ElectrolytesDocument8 pages01-05-21 - 01-12-21 - Fluid & ElectrolytesJolaine ValloNo ratings yet
- DISC, Drugs, Infection, Thick Basal MembraneDocument5 pagesDISC, Drugs, Infection, Thick Basal MembraneHOPENo ratings yet
- Distal To Ligament of Treitz: CausesDocument8 pagesDistal To Ligament of Treitz: CausesKiara GovenderNo ratings yet
- External Ear DiseasesDocument6 pagesExternal Ear DiseasesJohn Christopher LucesNo ratings yet
- Pedia Finals ReviewerDocument9 pagesPedia Finals ReviewerMarron Jane GanoticeNo ratings yet
- Gyne 2.6 - Benign and Malignant Tumors of The Ovaries and Fallopian TubesDocument8 pagesGyne 2.6 - Benign and Malignant Tumors of The Ovaries and Fallopian TubesVon HippoNo ratings yet
- Herpes Simplex Virus: 2 SerotypesDocument18 pagesHerpes Simplex Virus: 2 Serotypespedia blue bookNo ratings yet
- Derma MegatableDocument21 pagesDerma MegatableCoy NuñezNo ratings yet
- Ent Diseases of The Oral and Pharynx Dr. UyDocument7 pagesEnt Diseases of The Oral and Pharynx Dr. UyAileen EmyNo ratings yet
- Skin PathogensDocument4 pagesSkin PathogensEhi EdialeNo ratings yet
- Approach To Anemia: - Reticulocyte Count Is Most Important TestDocument15 pagesApproach To Anemia: - Reticulocyte Count Is Most Important TestJanella SuerteNo ratings yet
- GYNE 4.01b InfertilityDocument4 pagesGYNE 4.01b InfertilityGray SnellNo ratings yet
- Revalida Reviewer AsmphDocument237 pagesRevalida Reviewer AsmphShey ShocNo ratings yet
- Nephro - CKDDocument6 pagesNephro - CKDCarlos H. AcuñaNo ratings yet
- Cap CPGDocument40 pagesCap CPGMary Joy Oros-VallejeraNo ratings yet
- Diarrhea: WHO and IMCI GuidelinesDocument37 pagesDiarrhea: WHO and IMCI GuidelinesJohn Christopher LucesNo ratings yet
- Finals Trans (Hema)Document16 pagesFinals Trans (Hema)Ayesha CaragNo ratings yet
- Pediatric Surg TransDocument4 pagesPediatric Surg TransSven OrdanzaNo ratings yet
- GYNE 4.01a EndometriosisDocument4 pagesGYNE 4.01a EndometriosisGray SnellNo ratings yet
- UROLOGY 2020 (Doc BarcenasDocument33 pagesUROLOGY 2020 (Doc BarcenasJüdith Marie Reyes BauntoNo ratings yet
- Internal Medicine Finals ReviewerDocument8 pagesInternal Medicine Finals ReviewerRojales FrancisNo ratings yet
- Fammed Family Life CycleDocument3 pagesFammed Family Life CycleTMC PGI GENER MICKONo ratings yet
- (DERMA) 03 TineasDocument9 pages(DERMA) 03 TineasJolaine ValloNo ratings yet
- 1.06 General Pathology - Neoplasia (Part 1) - Dr. Annette SallilasDocument17 pages1.06 General Pathology - Neoplasia (Part 1) - Dr. Annette SallilasCherry RahimaNo ratings yet
- Esophageal Atresia: Name of The Disease Description ManagementDocument4 pagesEsophageal Atresia: Name of The Disease Description ManagementAle SandraNo ratings yet
- (PED2) 3.03 Pediatric Hematology - Castro (Final V.2)Document25 pages(PED2) 3.03 Pediatric Hematology - Castro (Final V.2)Sam MataNo ratings yet
- Medicine 6.1b Approach To Cancer Patients - FernandoDocument7 pagesMedicine 6.1b Approach To Cancer Patients - FernandoAbigail LausNo ratings yet
- Laryngitis: SpasmDocument13 pagesLaryngitis: Spasm44-Shruti paghdalNo ratings yet
- Pedia - Reviewer-AuditDocument9 pagesPedia - Reviewer-AuditJoanna Mae CarolinoNo ratings yet
- HerniaDocument5 pagesHerniasarguss14100% (5)
- Derm ChartDocument109 pagesDerm ChartAlana BolloneNo ratings yet
- m.10b Drugs Used in Gastrointestinal Diseases 03-26-18 (Table)Document3 pagesm.10b Drugs Used in Gastrointestinal Diseases 03-26-18 (Table)Dasha VeeNo ratings yet
- Pathology 5.05b Vagina and Vulva - DR - Dy (Final Edit)Document11 pagesPathology 5.05b Vagina and Vulva - DR - Dy (Final Edit)Dranreb Berylle MasangkayNo ratings yet
- VulvaDocument7 pagesVulvaJose SirittNo ratings yet
- Breast CancerDocument6 pagesBreast Cancersarguss14No ratings yet
- Derma Notes 1Document31 pagesDerma Notes 1KirstinNo ratings yet
- The Normal Kidney: Pediatrics 2 The Urinary System and Urinary Tract InfectionsDocument4 pagesThe Normal Kidney: Pediatrics 2 The Urinary System and Urinary Tract Infectionssarguss14No ratings yet
- Dse Pathogenesis/ Causes Diagnosis Complications TX Prognosis NotesDocument5 pagesDse Pathogenesis/ Causes Diagnosis Complications TX Prognosis NotesLuka Desabelle- JustoNo ratings yet
- Pedia S1Document22 pagesPedia S1betweenNo ratings yet
- (Surg2) 5.1b Introduction To Anesthesia-Part 2Document16 pages(Surg2) 5.1b Introduction To Anesthesia-Part 2AlloiBialbaNo ratings yet
- Vulva CancerDocument2 pagesVulva CancerLim Hui ZhuanNo ratings yet
- (PLM) Oral Cavity Salivary Glands Pharynx and EsophagusDocument9 pages(PLM) Oral Cavity Salivary Glands Pharynx and EsophagusJovilyn SilongaNo ratings yet
- Pediatrics:: History Taking and Physical Examination of AdolescentsDocument14 pagesPediatrics:: History Taking and Physical Examination of AdolescentsJüdith Marie Reyes BauntoNo ratings yet
- Neonatology I: Pediatrics 1.1Document15 pagesNeonatology I: Pediatrics 1.1Kurt ZepedaNo ratings yet
- Small Intestine 01 PDFDocument9 pagesSmall Intestine 01 PDFfadoNo ratings yet
- Review Slides OphthaDocument14 pagesReview Slides OphthaSUSHMITA MAE ROSE CONTRERASNo ratings yet
- Gastrointestinal Diseases Part1Document7 pagesGastrointestinal Diseases Part1sarguss14100% (1)
- Bleeding Disorders 1 - DR - Kamal MokbelDocument13 pagesBleeding Disorders 1 - DR - Kamal MokbelRawan E. SaeedNo ratings yet
- Topic: Asthma and Copd: Internal Medicine IiDocument8 pagesTopic: Asthma and Copd: Internal Medicine IicarlosNo ratings yet
- Neuro General Neuro: Proptosis/ Exophthalmos ChemosisDocument4 pagesNeuro General Neuro: Proptosis/ Exophthalmos ChemosisShakina FareedNo ratings yet
- B - Embyrology HomologuesDocument1 pageB - Embyrology HomologuesS ParekhNo ratings yet
- Malaria: Prima Dewi Yuliani 1210312120 Widyatul Aina Alfioni ParsiskaDocument27 pagesMalaria: Prima Dewi Yuliani 1210312120 Widyatul Aina Alfioni ParsiskaAnonymous Di1zSIkRBHNo ratings yet
- Shanz - Ent 1.07 NoseDocument4 pagesShanz - Ent 1.07 NosePetrina XuNo ratings yet
- Shanz - Pedia 1.03Document16 pagesShanz - Pedia 1.03Petrina XuNo ratings yet
- Shanz - Ent 1.06 Facial Nerve and Traumatic Facial ParalysisDocument3 pagesShanz - Ent 1.06 Facial Nerve and Traumatic Facial ParalysisPetrina XuNo ratings yet
- SHANZ - ENT 1.03c INNER EAR - HEARING LOSS AND REHABDocument5 pagesSHANZ - ENT 1.03c INNER EAR - HEARING LOSS AND REHABPetrina XuNo ratings yet
- Shanz - Ent 1.02 Middle EarDocument3 pagesShanz - Ent 1.02 Middle EarPetrina XuNo ratings yet
- Shanz - Pedia 1.01Document7 pagesShanz - Pedia 1.01Petrina XuNo ratings yet
- SHANZ - ENT 1.03a INNER EAR (PART 1)Document3 pagesSHANZ - ENT 1.03a INNER EAR (PART 1)Petrina XuNo ratings yet
- Shanz - Pedia 1.02 ASD, ADHD, LDDocument5 pagesShanz - Pedia 1.02 ASD, ADHD, LDPetrina XuNo ratings yet
- Shanz - Pedia Ii 2.03Document7 pagesShanz - Pedia Ii 2.03Petrina XuNo ratings yet
- Shanz - Pedia Ii 2.04Document4 pagesShanz - Pedia Ii 2.04Petrina XuNo ratings yet
- Shanz - Pedia Ii 2.02 NewDocument7 pagesShanz - Pedia Ii 2.02 NewPetrina XuNo ratings yet
- Shanz - PEDIA II 2.01 NEWDocument8 pagesShanz - PEDIA II 2.01 NEWPetrina XuNo ratings yet
- Shanz - Commed Le 2Document3 pagesShanz - Commed Le 2Petrina XuNo ratings yet
- Shanz - Comm Med Le 1Document4 pagesShanz - Comm Med Le 1Petrina XuNo ratings yet
- Shanz - Clinpath Le1Document7 pagesShanz - Clinpath Le1Petrina XuNo ratings yet
- Shanz - Clinpath Le 2Document3 pagesShanz - Clinpath Le 2Petrina XuNo ratings yet
- Clinpath PraxDocument4 pagesClinpath PraxPetrina XuNo ratings yet
- Severe Inflammation Acute MOF, Early Death Injury SIRS Hemostasis Normal Recovery Less Inflammation CARS Prolonged ImmunosuppressionDocument3 pagesSevere Inflammation Acute MOF, Early Death Injury SIRS Hemostasis Normal Recovery Less Inflammation CARS Prolonged ImmunosuppressionPetrina XuNo ratings yet
- SHANZ - MED II DIABETES MELLITUS Fixed (Merged)Document11 pagesSHANZ - MED II DIABETES MELLITUS Fixed (Merged)Petrina XuNo ratings yet
- Shanz - Acute Kidney Injury PDFDocument4 pagesShanz - Acute Kidney Injury PDFPetrina XuNo ratings yet
- Shanz - Chronic Kidney DiseaseDocument3 pagesShanz - Chronic Kidney DiseasePetrina XuNo ratings yet
- New - BMP3005 - ABF - Assessment Brief - FDocument5 pagesNew - BMP3005 - ABF - Assessment Brief - Fmilka traykovNo ratings yet
- MFD16I003 FinalDocument16 pagesMFD16I003 FinalAditya KumarNo ratings yet
- Eco EssayDocument3 pagesEco EssaymanthanNo ratings yet
- Sample Valuation ReportDocument15 pagesSample Valuation Reportayush singlaNo ratings yet
- Kamapehmilya: Fitness Through Traditional DancesDocument21 pagesKamapehmilya: Fitness Through Traditional DancesValerieNo ratings yet
- Plant Vs Filter by Diana WalstadDocument6 pagesPlant Vs Filter by Diana WalstadaachuNo ratings yet
- Hansen Aise Im Ch12Document66 pagesHansen Aise Im Ch12Rizki19maretNo ratings yet
- Final Matatag Epp Tle CG 2023 Grades 4 10Document184 pagesFinal Matatag Epp Tle CG 2023 Grades 4 10DIVINE GRACE CABAHUGNo ratings yet
- Planning Effective Advertising and Promotion Strategies For A Target AudienceDocument16 pagesPlanning Effective Advertising and Promotion Strategies For A Target Audiencebakhoo12No ratings yet
- A Summer Training ReportDocument39 pagesA Summer Training ReportShubham SainyNo ratings yet
- Bankers ChoiceDocument18 pagesBankers ChoiceArchana ThirunagariNo ratings yet
- Cad32gd - Contactor ManualDocument28 pagesCad32gd - Contactor Manualhassan karimiNo ratings yet
- Makerere University Is Inviting Applications For Undergraduate Admissions On Private Sponsorship For Academic Year 2015/2016Document9 pagesMakerere University Is Inviting Applications For Undergraduate Admissions On Private Sponsorship For Academic Year 2015/2016The Campus TimesNo ratings yet
- T10 - PointersDocument3 pagesT10 - PointersGlory of Billy's Empire Jorton KnightNo ratings yet
- Indian Traditional Musical InstrumentsDocument3 pagesIndian Traditional Musical InstrumentsPiriya94No ratings yet
- TSC M34PV - TSC M48PV - User Manual - CryoMed - General Purpose - Rev A - EnglishDocument93 pagesTSC M34PV - TSC M48PV - User Manual - CryoMed - General Purpose - Rev A - EnglishMurielle HeuchonNo ratings yet
- Book Review Fiction New HereDocument7 pagesBook Review Fiction New HereFILZAH SYAUQINA BINTI SUBLY Pelajar KPTM IpohNo ratings yet
- Demand Determinants EEMDocument22 pagesDemand Determinants EEMPrabha KaranNo ratings yet
- Lightolier Lytecaster Downlights Catalog 1984Document68 pagesLightolier Lytecaster Downlights Catalog 1984Alan MastersNo ratings yet
- El TontoDocument92 pagesEl TontoRobertNo ratings yet
- March 2023 (v2) INDocument8 pagesMarch 2023 (v2) INmarwahamedabdallahNo ratings yet
- Grammar Practice #2Document6 pagesGrammar Practice #2Constantin OpreaNo ratings yet
- ERP22006Document1 pageERP22006Ady Surya LesmanaNo ratings yet
- SLTMobitel AssignmentDocument3 pagesSLTMobitel AssignmentSupun ChandrakanthaNo ratings yet
- ENG 102 Essay PromptDocument2 pagesENG 102 Essay Promptarshia winNo ratings yet
- Lit 30Document2 pagesLit 30ReemAlashhab81No ratings yet
- Story 1Document3 pagesStory 1api-296631749No ratings yet
- PBPO008E FrontmatterDocument13 pagesPBPO008E FrontmatterParameswararao Billa67% (3)
- II. Put The Verbs in The Correct FormsDocument3 pagesII. Put The Verbs in The Correct FormsNguyễn Bích DiệpNo ratings yet
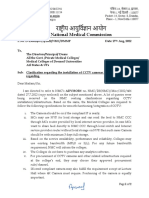
- CCTV Guidelines - Commission Letter Dated 27.08.2022Document2 pagesCCTV Guidelines - Commission Letter Dated 27.08.2022Sumeet TripathiNo ratings yet