You might also like
- ArticleText 23375 1 10 20201114Document10 pagesArticleText 23375 1 10 20201114rizwan.physics83No ratings yet
- Evaluating Surgical Risk Using FMEA and MULTIMOORA Methods Under A Single-Valued Trapezoidal Neutrosophic EnvironmentDocument17 pagesEvaluating Surgical Risk Using FMEA and MULTIMOORA Methods Under A Single-Valued Trapezoidal Neutrosophic Environmentgadhang dewanggaNo ratings yet
- Infections in Surgery: Prevention and ManagementFrom EverandInfections in Surgery: Prevention and ManagementMassimo SartelliNo ratings yet
- Nurses' postoperative wound care practices and factors affecting performanceDocument7 pagesNurses' postoperative wound care practices and factors affecting performanceMagic_OverNo ratings yet
- Risk Management Handbook for Health Care Organizations, 3 Volume SetFrom EverandRisk Management Handbook for Health Care Organizations, 3 Volume SetNo ratings yet
- WaundcareDocument7 pagesWaundcarePaulo Henrique SoaresNo ratings yet
- Disinfectionand Sterilization Related Situationsfor Patient SafetyinDocument8 pagesDisinfectionand Sterilization Related Situationsfor Patient SafetyinLeah Mariz RocaNo ratings yet
- WAP YANA 2 EditDocument41 pagesWAP YANA 2 Editintan1234No ratings yet
- Risk Analysis in Healthcare Organizations: Methodological Framework and Critical VariablesDocument15 pagesRisk Analysis in Healthcare Organizations: Methodological Framework and Critical VariablesIvan PavlovicNo ratings yet
- 86675-334319-3-PBDocument10 pages86675-334319-3-PBmetech8xNo ratings yet
- The Comprehensive Double Loop Activities For.12Document5 pagesThe Comprehensive Double Loop Activities For.12Mishell TelloNo ratings yet
- Research Article: Adaptive Failure Identification For Healthcare Risk Analysis and Its Application On E-HealthcareDocument18 pagesResearch Article: Adaptive Failure Identification For Healthcare Risk Analysis and Its Application On E-HealthcareAlejandro CardonaNo ratings yet
- Hospital Crisis Plan for COVID-19Document17 pagesHospital Crisis Plan for COVID-19خلدون سليمNo ratings yet
- 1 s2.0 S260364792100035XDocument9 pages1 s2.0 S260364792100035XOncología CdsNo ratings yet
- Patient Safety Risk ManagementDocument5 pagesPatient Safety Risk Managementnoor88No ratings yet
- Jepm 2 118Document5 pagesJepm 2 118Joni MokodoNo ratings yet
- IV Therapy Article For ExamDocument10 pagesIV Therapy Article For ExamHui HuangNo ratings yet
- A Model For Reducing Medical ErrorsDocument4 pagesA Model For Reducing Medical ErrorsPinto PintoNo ratings yet
- DRAFT Risk Management in HealthcareDocument6 pagesDRAFT Risk Management in HealthcareAsma Al-FayezNo ratings yet
- Approach To Risk Management in Medical Practice: Standpoint of A HospitalDocument10 pagesApproach To Risk Management in Medical Practice: Standpoint of A HospitalPutra PositifNo ratings yet
- WA Health Clinical Risk Management GuidelinesDocument46 pagesWA Health Clinical Risk Management GuidelinesRuli Nurul Aman100% (1)
- RizkiDocument24 pagesRizkiseviaetika09No ratings yet
- 2564-Article Text-17430-2-10-20231124 (1)Document14 pages2564-Article Text-17430-2-10-20231124 (1)Rhey PrimeNo ratings yet
- Jci WP Med Suction and Fluid Waste MGT FinalDocument16 pagesJci WP Med Suction and Fluid Waste MGT FinalAbhi RajNo ratings yet
- Latest Risk Management Guideline (ISO 14971:2019) & Environmental Aspects of Medical DeviceDocument10 pagesLatest Risk Management Guideline (ISO 14971:2019) & Environmental Aspects of Medical DeviceIjdra Journal Jitendra BadjatyaNo ratings yet
- Ori Stojkovic2017Document9 pagesOri Stojkovic2017Nur LaelaNo ratings yet
- Jce 0000000000000193Document8 pagesJce 0000000000000193jlopezhamdanNo ratings yet
- Evaluating The Application of Failure Mode and Effects Analysis Technique in Hospital Wards: A Systematic ReviewDocument10 pagesEvaluating The Application of Failure Mode and Effects Analysis Technique in Hospital Wards: A Systematic ReviewManuel MesaNo ratings yet
- Imprtant Projects For Six Sigma HospitalDocument12 pagesImprtant Projects For Six Sigma Hospitalشادي الاخرسNo ratings yet
- ADocument4 pagesAphanuel yosefNo ratings yet
- Nursing EmpowermentDocument8 pagesNursing EmpowermentmeityNo ratings yet
- Clinical Risk Management For Anaesthetists - CeaDocument6 pagesClinical Risk Management For Anaesthetists - CeaLucas CabreraNo ratings yet
- NSPG Ambulatory Risk and Patient Safety Manager - Job DescriptionDocument6 pagesNSPG Ambulatory Risk and Patient Safety Manager - Job DescriptionSpi RsiNo ratings yet
- Analysis of A Healthcare Risk Management PlanDocument6 pagesAnalysis of A Healthcare Risk Management PlanGeralds B GeraldNo ratings yet
- Analysis of A Healthcare Risk Management PlanDocument6 pagesAnalysis of A Healthcare Risk Management PlanGeralds B GeraldNo ratings yet
- Application of Risk Management For Dental Implants Based On ISO 14971Document6 pagesApplication of Risk Management For Dental Implants Based On ISO 14971Laura Corrales RicaldezNo ratings yet
- Pressure Ulcers Nurses Knowledge PDFDocument6 pagesPressure Ulcers Nurses Knowledge PDFVar InderNo ratings yet
- Medicine: Patient Safety Culture Perceptions in The College of DentistryDocument5 pagesMedicine: Patient Safety Culture Perceptions in The College of DentistryBassam AlqadasiNo ratings yet
- Iso 14971 8-B2017065Document6 pagesIso 14971 8-B2017065Ica LarissaNo ratings yet
- Cross-Sectional Study On Patient Safety Culture, Patient Safety Competency, and Adverse EventsDocument19 pagesCross-Sectional Study On Patient Safety Culture, Patient Safety Competency, and Adverse EventseswaynedNo ratings yet
- Radiation Safety 1Document3 pagesRadiation Safety 1api-632146706No ratings yet
- COVID-19 orthopaedic surgical protocolsDocument23 pagesCOVID-19 orthopaedic surgical protocolsDoctor's BettaNo ratings yet
- GUIDELINE For IMPROVING OUTCOME After Anaesthesia and Critical Care - 2017 - College of AnaesthesiologistsDocument83 pagesGUIDELINE For IMPROVING OUTCOME After Anaesthesia and Critical Care - 2017 - College of AnaesthesiologistsSanj.etcNo ratings yet
- Analisis Pelaksanaan Manajemen Risiko Di Instalasi Farmasi Rumah Sakit Umum Daerah Tugurejo Semarang TAHUN 2018Document9 pagesAnalisis Pelaksanaan Manajemen Risiko Di Instalasi Farmasi Rumah Sakit Umum Daerah Tugurejo Semarang TAHUN 2018Sadam HusenRaNo ratings yet
- Risk Management Implementation Analysis at Tugurejo Hospital Pharmacy InstallationDocument9 pagesRisk Management Implementation Analysis at Tugurejo Hospital Pharmacy InstallationAnonymous FLInViNo ratings yet
- Patient Safety To Prevent Bad Ulcer1sDocument19 pagesPatient Safety To Prevent Bad Ulcer1sMo7med YasserNo ratings yet
- Peer Reviwed Article Risk AssessmentDocument14 pagesPeer Reviwed Article Risk AssessmentAyesha HamdanNo ratings yet
- Dental Infection and Prevention Control GuidelineDocument7 pagesDental Infection and Prevention Control GuidelineMega ArfiyantiNo ratings yet
- Iso 14971 8-B2017065Document6 pagesIso 14971 8-B2017065gabigardasNo ratings yet
- Roils 1Document4 pagesRoils 1api-574059920No ratings yet
- Radiation SafetyDocument4 pagesRadiation Safetybraith7811No ratings yet
- FMECA - Cytotoxic DrugDocument6 pagesFMECA - Cytotoxic DrugRizqy AnandaNo ratings yet
- 10.1016/j.prro.2017.08.005: Practical Radiation OncologyDocument23 pages10.1016/j.prro.2017.08.005: Practical Radiation OncologyRosliana MahardhikaNo ratings yet
- 10 12968@bjon 2020 29 1 28Document7 pages10 12968@bjon 2020 29 1 28diah fitriNo ratings yet
- 2022-06-15 EIT-Medidee - 04 Clinical EvidenceDocument33 pages2022-06-15 EIT-Medidee - 04 Clinical EvidenceJugurtha BoutlikhetNo ratings yet
- 2022-06-14 EIT-Medidee - 02 US RegulationsDocument65 pages2022-06-14 EIT-Medidee - 02 US RegulationsJugurtha BoutlikhetNo ratings yet
- 2022-06-15 EIT-Medidee - 03 V&V-TDDocument49 pages2022-06-15 EIT-Medidee - 03 V&V-TDJugurtha BoutlikhetNo ratings yet
- IEC 62304 - A Thorough Yet Simple GuideDocument47 pagesIEC 62304 - A Thorough Yet Simple GuideJugurtha BoutlikhetNo ratings yet
- Medical Device Technical Documentation 1671293832 PDFDocument6 pagesMedical Device Technical Documentation 1671293832 PDFJugurtha BoutlikhetNo ratings yet
- RAPS Regulatory Competency Framework 2021Document17 pagesRAPS Regulatory Competency Framework 2021Jugurtha BoutlikhetNo ratings yet
- Iso 13405 3 2015 PDFDocument11 pagesIso 13405 3 2015 PDFJugurtha BoutlikhetNo ratings yet
- LPI PH PDFDocument4 pagesLPI PH PDFHumberto Tapias CutivaNo ratings yet
- Text 1 Is For No 1 - 4 The Rabbit Revenge: I. Pilihlah Salah Satu Jawaban Yang Benar!Document4 pagesText 1 Is For No 1 - 4 The Rabbit Revenge: I. Pilihlah Salah Satu Jawaban Yang Benar!Diandra MomentNo ratings yet
- Regina Downtown Community Support Team ReportDocument28 pagesRegina Downtown Community Support Team ReportJeremy SimesNo ratings yet
- DNA Discoveries Reveal Human DNA as a Biological InternetDocument7 pagesDNA Discoveries Reveal Human DNA as a Biological InternetUmbrielNo ratings yet
- Legalism QuotesDocument14 pagesLegalism QuotesfruittinglesNo ratings yet
- Structural Stainless Steel Designing With Stainless Steel: Ing. Maarten FortanDocument153 pagesStructural Stainless Steel Designing With Stainless Steel: Ing. Maarten FortanJohn Philip Neri BesedillasNo ratings yet
- Presentation - On SVAMITVADocument18 pagesPresentation - On SVAMITVAPraveen PrajapatiNo ratings yet
- Queen'S University Midterm Examination Department of EconomicsDocument7 pagesQueen'S University Midterm Examination Department of EconomicsAsif Ahmed NeloyNo ratings yet
- Balanced Scorecard ThesisDocument59 pagesBalanced Scorecard Thesisapi-3825626100% (5)
- Capstone Presentation 2020Document12 pagesCapstone Presentation 2020api-539629427No ratings yet
- 01 A Beginner's Guide To TajikiDocument384 pages01 A Beginner's Guide To Tajikitaryuman100% (1)
- 1Document5 pages1qweqweNo ratings yet
- 5.1 Advanced Pattern Making - IDocument9 pages5.1 Advanced Pattern Making - IRisul Islam EmonNo ratings yet
- PR & PublicityDocument16 pagesPR & PublicityVipul Partap100% (2)
- Brfo193 Radiotherapy Dose Fractionation Third-Edition PDFDocument137 pagesBrfo193 Radiotherapy Dose Fractionation Third-Edition PDFMed MedNo ratings yet
- Award 34509Document43 pagesAward 34509Brendon ChiaNo ratings yet
- Earned Value Analysis 8 StepsDocument8 pagesEarned Value Analysis 8 StepsHira RazzaqNo ratings yet
- Human Ear and Role of Hearing in HCIDocument4 pagesHuman Ear and Role of Hearing in HCIrafia0% (1)
- Revised Bsy Elementary Siatonwest 2 and Pio-Macahig - 2014-15 As of June 6 2014Document31 pagesRevised Bsy Elementary Siatonwest 2 and Pio-Macahig - 2014-15 As of June 6 2014api-273918959No ratings yet
- Vivekananda's Role as Revivalist Reformer and His Ideas of Equality and Spiritual RevolutionDocument2 pagesVivekananda's Role as Revivalist Reformer and His Ideas of Equality and Spiritual RevolutionMartin VanlalhlimpuiaNo ratings yet
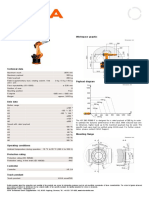
- KR 280 R3080 F technical specificationsDocument1 pageKR 280 R3080 F technical specificationsDorobantu CatalinNo ratings yet
- Practical File ON Programming For Problem Solving Lab (: 21BTCS181)Document15 pagesPractical File ON Programming For Problem Solving Lab (: 21BTCS181)Vaibhavi SinghNo ratings yet
- Vessel and Conveyors - VPDDocument4 pagesVessel and Conveyors - VPDAntonio Mizraim Magallon SantanaNo ratings yet
- Strategic Planning Assignment - TescoDocument16 pagesStrategic Planning Assignment - TescoKayode Trinity Omosebi100% (1)
- VW Crafter 2f Component Locations EngDocument118 pagesVW Crafter 2f Component Locations EngHugo Emilio Garcia Gonzalez100% (2)
- Faktor OrganisasiDocument9 pagesFaktor OrganisasiNur Fatin NabilahNo ratings yet
- SIHI - Control Narrative Proc Compressor UnitDocument5 pagesSIHI - Control Narrative Proc Compressor Unitman_y2k100% (1)
- Last Lesson: How Did Franz Feelings About M Hamel and School Change ?Document4 pagesLast Lesson: How Did Franz Feelings About M Hamel and School Change ?RitikaNo ratings yet