You might also like
- Victory Over PainDocument366 pagesVictory Over PainadimantoNo ratings yet
- @literaturamedica BLS 2021Document94 pages@literaturamedica BLS 2021siracue22No ratings yet
- Mitral StenosisDocument67 pagesMitral StenosisNamithaNo ratings yet
- Paediatric Anaesthesia PDFDocument33 pagesPaediatric Anaesthesia PDFMarcelitaTaliaDuwiriNo ratings yet
- Enhanced Recovery After Surgery (ERAS) in Emergency Abdominal Surgery: Background, Preoperative Components of ERAS, Intraoperative Components of ERASDocument9 pagesEnhanced Recovery After Surgery (ERAS) in Emergency Abdominal Surgery: Background, Preoperative Components of ERAS, Intraoperative Components of ERASAndre F SusantioNo ratings yet
- Anesthesia For Hepatic Resection and Laparascopic SurgeryDocument64 pagesAnesthesia For Hepatic Resection and Laparascopic SurgeryBiserat GetnetNo ratings yet
- 9 Hypertension (1)Document36 pages9 Hypertension (1)shemo hayatNo ratings yet
- Pulmonary Hypertension in The CICUDocument50 pagesPulmonary Hypertension in The CICUCardiacCareCenterMCHNo ratings yet
- Management of Acute PainDocument76 pagesManagement of Acute PainAnonymous nruHyuwtJ100% (1)
- Anesthesia For Genitourinary SurgeryDocument76 pagesAnesthesia For Genitourinary SurgeryWenny Eka FildayantiNo ratings yet
- 1.05 (Surgery) General Anesthesia - Airway ManagementDocument3 pages1.05 (Surgery) General Anesthesia - Airway ManagementLeo Mari Go LimNo ratings yet
- Anesthesia Management of AdenotonsillectomyDocument5 pagesAnesthesia Management of Adenotonsillectomypradini sugihartoNo ratings yet
- Anaesthetic Management of Joint Replacement SurgeriesDocument55 pagesAnaesthetic Management of Joint Replacement SurgeriesRaguNo ratings yet
- Race Topics SystemwiseDocument17 pagesRace Topics SystemwisemickeyNo ratings yet
- InhalationalDocument87 pagesInhalationalsourabh jakharNo ratings yet
- OSA and Periop Complications 2012Document9 pagesOSA and Periop Complications 2012cjbae22No ratings yet
- Anaesthesia For Trauma PatientsDocument5 pagesAnaesthesia For Trauma Patientscahya candraNo ratings yet
- Anesthesia For Patients With Diabetes Mellitus - UpToDateDocument31 pagesAnesthesia For Patients With Diabetes Mellitus - UpToDateEduardoNo ratings yet
- Failed Spinal AnaesthesiaDocument10 pagesFailed Spinal Anaesthesian12345678n100% (1)
- 75 MW Lab Test InfoDocument295 pages75 MW Lab Test InfoMd Suzon MahmudNo ratings yet
- Anesthesia EquipmentDocument51 pagesAnesthesia EquipmentVeronica ChavezNo ratings yet
- Ventricular Assist DeviceDocument12 pagesVentricular Assist DevicesamadonyNo ratings yet
- (ANES) Sat 02 Anesthesia Machine and Equipment (A2021)Document3 pages(ANES) Sat 02 Anesthesia Machine and Equipment (A2021)Ricky Justin NgoNo ratings yet
- Prediction of Fluid ResponsivenessDocument4 pagesPrediction of Fluid ResponsivenessSANTOSH KUMAR BHASKARNo ratings yet
- MS-HKSS-Pigging Testing Drying Rev A - YNB 16''Document64 pagesMS-HKSS-Pigging Testing Drying Rev A - YNB 16''AAISATNo ratings yet
- Awareness Under AnesthesiaDocument27 pagesAwareness Under AnesthesiaagatakassaNo ratings yet
- Chemistry Note PDFDocument123 pagesChemistry Note PDFAiman MazlanNo ratings yet
- Guideline Title: Intra-Aortic Balloon Pump ManagementDocument16 pagesGuideline Title: Intra-Aortic Balloon Pump ManagementJansen ChNo ratings yet
- Ethylene ProcessDocument8 pagesEthylene Processkapil1979No ratings yet
- Anesthesia and Analgesia Book 1 PDFDocument112 pagesAnesthesia and Analgesia Book 1 PDFDiana NiculaeNo ratings yet
- Lectire-Hypoxia 2020Document21 pagesLectire-Hypoxia 2020Bol Dhalbeny Malual100% (1)
- Anaesthesia For Infants and ChildrenDocument9 pagesAnaesthesia For Infants and Childrenapi-142637023No ratings yet
- APA Guidelines On The Prevention of Postoperative Vomiting in ChildrenDocument35 pagesAPA Guidelines On The Prevention of Postoperative Vomiting in ChildrenMaria Lucia RossiNo ratings yet
- MODERATOR: DR Shreesh Mehrotra PRESENTER: DR Medha BhardwajDocument55 pagesMODERATOR: DR Shreesh Mehrotra PRESENTER: DR Medha BhardwajMilind Kothiyal100% (1)
- CHAPTER 2 - Material BalanceDocument30 pagesCHAPTER 2 - Material BalanceEvelyn100% (1)
- Rmtnotes AnesthesiologyDocument31 pagesRmtnotes AnesthesiologyCamille MagatNo ratings yet
- Icu 2Document57 pagesIcu 2AMIT KUMAR DEYNo ratings yet
- Obs and dlt-1Document74 pagesObs and dlt-1paru100% (1)
- ICU Ventilator - Group 4Document26 pagesICU Ventilator - Group 4Anh TrầnNo ratings yet
- Infections in ICUDocument7 pagesInfections in ICUNikolay ToméNo ratings yet
- Scalp Block and Cervical Plexus Block Techniques - UpToDateDocument28 pagesScalp Block and Cervical Plexus Block Techniques - UpToDateAna Belén Artero CastañoNo ratings yet
- Total Intravenous Anaesthesia in Children-1 PDFDocument6 pagesTotal Intravenous Anaesthesia in Children-1 PDFAurora TrifaNo ratings yet
- SAQ Past PaediatricDocument59 pagesSAQ Past PaediatricNurul Izzah AzmiNo ratings yet
- Anesthesia in Day Care PDFDocument15 pagesAnesthesia in Day Care PDFHKN nairNo ratings yet
- Electrofisiologia Cardiaca Guia Viasual 2 PDFDocument82 pagesElectrofisiologia Cardiaca Guia Viasual 2 PDFMiguel LizarragaNo ratings yet
- Neuroanesthesiology UpdateDocument23 pagesNeuroanesthesiology UpdateAhida VelazquezNo ratings yet
- Principles of Drug Therapy in DentistryDocument159 pagesPrinciples of Drug Therapy in Dentistryandrija PopovicNo ratings yet
- Lidocain and BuvipacainDocument6 pagesLidocain and BuvipacaintinahermantoNo ratings yet
- Pain AssessmentDocument5 pagesPain AssessmentLyssa KateNo ratings yet
- Drugs and Dosage Drugs and Dosage: Atropine Sulfate 1Mg/MlDocument3 pagesDrugs and Dosage Drugs and Dosage: Atropine Sulfate 1Mg/MlIna RamosNo ratings yet
- Abstract Dexmed Vs Lignocaine Final Abstract and ArticleDocument25 pagesAbstract Dexmed Vs Lignocaine Final Abstract and ArticleDr.S.Easwaramoorthy IAGES Secretary 2020No ratings yet
- Effect of Magnesium Sulphate On Intraoperative Hemodynamic Responses in Laparoscopic CholecystectomyDocument10 pagesEffect of Magnesium Sulphate On Intraoperative Hemodynamic Responses in Laparoscopic CholecystectomyIOSRjournalNo ratings yet
- ECMO (Extracorporeal Membrane Oxygenation) Services in NSWDocument40 pagesECMO (Extracorporeal Membrane Oxygenation) Services in NSWMarckus BrownNo ratings yet
- GMC Sponsorship TrustsDocument6 pagesGMC Sponsorship TrustsAsfar AzimeeNo ratings yet
- DR - Rajalakshmi.C: Emergency Physician MMHRC Institute of Emergency MedicineDocument22 pagesDR - Rajalakshmi.C: Emergency Physician MMHRC Institute of Emergency MedicineP Vinod KumarNo ratings yet
- Noninvasive Ventilator Devices and ModesDocument11 pagesNoninvasive Ventilator Devices and ModesISABEL SOFIA CABARCAS COGOLLONo ratings yet
- Procedural Sedation in Children - Preparation - UpToDateDocument26 pagesProcedural Sedation in Children - Preparation - UpToDaterogelio cruzNo ratings yet
- One Shot RevisionDocument171 pagesOne Shot RevisionKuldip PatelNo ratings yet
- Journal ClubDocument26 pagesJournal Clubysindhura23gmailcom100% (1)
- Drug Guideline Title: Remifentanil: SummaryDocument11 pagesDrug Guideline Title: Remifentanil: SummaryyafetNo ratings yet
- Moe Final Result 2069-05-02Document72 pagesMoe Final Result 2069-05-02MADAN BASNETNo ratings yet
- Obstetrics AnesthesiaDocument31 pagesObstetrics AnesthesiaNorfarhanah ZakariaNo ratings yet
- Assessment of Postoperative Fever BMJDocument40 pagesAssessment of Postoperative Fever BMJMario Guzmán GutiérrezNo ratings yet
- Liverpool Ni Modi PineDocument5 pagesLiverpool Ni Modi Pinerachmat fajar noor kNo ratings yet
- Bier Block (Intravenous Regional Anesthesia), Handout PDFDocument8 pagesBier Block (Intravenous Regional Anesthesia), Handout PDFjahangirealamNo ratings yet
- History of MassageDocument36 pagesHistory of Massagewww.sasionline.com100% (2)
- Anesthesia and Analgesia Book 2Document186 pagesAnesthesia and Analgesia Book 2Diana NiculaeNo ratings yet
- The Evolution of Veterinary Anaesthesia: "Shell" R S Arch Limited, Tunstall Laboratory Sittingbourne KentDocument7 pagesThe Evolution of Veterinary Anaesthesia: "Shell" R S Arch Limited, Tunstall Laboratory Sittingbourne KentDiana NiculaeNo ratings yet
- 10-GAZDIĆ CompressedDocument8 pages10-GAZDIĆ CompressedDiana NiculaeNo ratings yet
- A History of Veterinary AnaesthesiaDocument10 pagesA History of Veterinary AnaesthesiaDiana NiculaeNo ratings yet
- Anne - 2014 - Market Projections of Cellulose Nanomaterial-Enabled Products - Part 1 ApplicationsDocument8 pagesAnne - 2014 - Market Projections of Cellulose Nanomaterial-Enabled Products - Part 1 Applicationskrishnakant bholeNo ratings yet
- Corrosion Behaviour of CIDocument1 pageCorrosion Behaviour of CIBaher ElsheikhNo ratings yet
- Dehydrative Etherification of Carbohydrates To 5-Ethoxymethylfurfural Over SBA-15-supported Sn-Modified Heteropolysilicate CatalystsDocument12 pagesDehydrative Etherification of Carbohydrates To 5-Ethoxymethylfurfural Over SBA-15-supported Sn-Modified Heteropolysilicate Catalystsbruno barrosNo ratings yet
- Pergopak M3 Matting and Effect Agent Technical Data SheetDocument2 pagesPergopak M3 Matting and Effect Agent Technical Data SheetAdhvik PuriNo ratings yet
- Effect On Superhydrophobic Surfaces On ElectricalDocument12 pagesEffect On Superhydrophobic Surfaces On Electricalhadi ebrahimfathNo ratings yet
- Black SoilDocument26 pagesBlack SoilPatel DipanNo ratings yet
- Vaibhav Project PDF PrintDocument22 pagesVaibhav Project PDF Printshubham shindeNo ratings yet
- Exploring The Potential and Opportunities of Current Tools For Removal of Hazardous Materials From EnvironmentsDocument3 pagesExploring The Potential and Opportunities of Current Tools For Removal of Hazardous Materials From EnvironmentsAli ShanNo ratings yet
- Heat Treatment of SteelsDocument29 pagesHeat Treatment of SteelsJay ChoudharyNo ratings yet
- Anamet CatalogDocument69 pagesAnamet CatalogMario Landeta PérezNo ratings yet
- FixationDocument5 pagesFixationMargalet Aguinaldo100% (1)
- Flocon MC3: Membrane Cleaner For InorganicsDocument2 pagesFlocon MC3: Membrane Cleaner For InorganicsCyrilDepalomaNo ratings yet
- Production of Hydrocarbons by Catalytic Upgrading of A Fast Pyrolysis Bio-Oil. Part II: Comparative Catalyst Performance and Reaction PathwaysDocument18 pagesProduction of Hydrocarbons by Catalytic Upgrading of A Fast Pyrolysis Bio-Oil. Part II: Comparative Catalyst Performance and Reaction PathwaysBP PattanaikNo ratings yet
- On The Hydrodesulfurization of FCC Gasoline: A ReviewDocument30 pagesOn The Hydrodesulfurization of FCC Gasoline: A ReviewargirotopNo ratings yet
- San Lu Case StudyDocument9 pagesSan Lu Case StudyJue Yadanar WinNo ratings yet
- Manual - MilleniumDocument165 pagesManual - MilleniumHumberto HernánmdezNo ratings yet
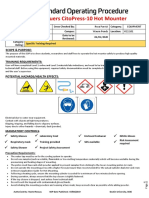
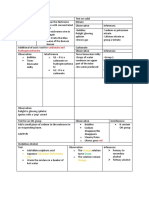
- Hot Mounting On CitoPress 10 SOPDocument2 pagesHot Mounting On CitoPress 10 SOPMạnh Đức NguyễnNo ratings yet
- MSDS - Terralin Chlorine TabletsDocument8 pagesMSDS - Terralin Chlorine TabletsRista JayantiNo ratings yet
- Hyprox 500 MSDSDocument16 pagesHyprox 500 MSDSkurniawanNo ratings yet
- Flame TestDocument2 pagesFlame Testfreedom5345No ratings yet
- STPG370 - SteelJIS - Datasheet, Chemical Composition, Standards and PropertiesDocument1 pageSTPG370 - SteelJIS - Datasheet, Chemical Composition, Standards and PropertiesSali Purwandi サリNo ratings yet
- 469 G Kola GbedemDocument4 pages469 G Kola GbedemStephen Yao GbedemaNo ratings yet
- Reactions of Aldehydes and KetonesDocument12 pagesReactions of Aldehydes and KetonespramodpsmpharmNo ratings yet
- Msds ANSI Format 16-Section Blank Form Word 97 - 2003Document4 pagesMsds ANSI Format 16-Section Blank Form Word 97 - 2003PremVikash SV100% (1)
- Medicine Indent For The May-Month 2023Document8 pagesMedicine Indent For The May-Month 2023Nagendrakumar NagendraNo ratings yet