You might also like
- Estudio FRS Diabetes Tipo 2Document7 pagesEstudio FRS Diabetes Tipo 2ps.silviaghioneNo ratings yet
- DHD - L1 - Anthropometry and Clinical AssessmentDocument69 pagesDHD - L1 - Anthropometry and Clinical Assessmentgp5d7nfjjpNo ratings yet
- GerantologyDocument6 pagesGerantologyusmanNo ratings yet
- A Low-Cost Automatic Body Mass Index Machine: The Design, Development, Calibration, Testing and AnalysisDocument20 pagesA Low-Cost Automatic Body Mass Index Machine: The Design, Development, Calibration, Testing and Analysis10aet cadNo ratings yet
- Promoting Healthy WeightDocument16 pagesPromoting Healthy WeightJose Fernando Díez ConchaNo ratings yet
- Obesity in Children: Definition, Etiology and Approach: Review ArticleDocument9 pagesObesity in Children: Definition, Etiology and Approach: Review Articleanang fajarNo ratings yet
- Infant Nutrition: of For Optimum andDocument35 pagesInfant Nutrition: of For Optimum andm mNo ratings yet
- Skim Fold Medical Students MalaysiaDocument7 pagesSkim Fold Medical Students MalaysiaKalesware MuniandyNo ratings yet
- Body CompositionDocument28 pagesBody CompositionRohitNo ratings yet
- Review of Childhood Obesity: From Epidemiology, Etiology, and Comorbidities To Clinical Assessment and TreatmentDocument15 pagesReview of Childhood Obesity: From Epidemiology, Etiology, and Comorbidities To Clinical Assessment and TreatmentDouglas castroNo ratings yet
- Safira Ar Rahmah Ramadani S - AntroDocument30 pagesSafira Ar Rahmah Ramadani S - AntroFira RamadhaniNo ratings yet
- UzogaraSG UnderweighttheLessDiscussedTypeofUnhealthyWeight - AReviewDocument18 pagesUzogaraSG UnderweighttheLessDiscussedTypeofUnhealthyWeight - AReviewAshik HaqueNo ratings yet
- ObesityDocument32 pagesObesityRao MehakNo ratings yet
- Nutritional Assessment of Schools Children of Six Years Old in Aldora Family Medical Center in Baghdadiraq 2327 4972 1000223Document5 pagesNutritional Assessment of Schools Children of Six Years Old in Aldora Family Medical Center in Baghdadiraq 2327 4972 1000223Pooja SahuNo ratings yet
- Altura Promedio en México Estudio de CasoDocument8 pagesAltura Promedio en México Estudio de CasoEddy HarosNo ratings yet
- Nutritional Assesment: Phoenix Research Institute Nursing Dip. 1 Year Nutrition by P.M Banda M.D (BSC HB, MBCHB)Document33 pagesNutritional Assesment: Phoenix Research Institute Nursing Dip. 1 Year Nutrition by P.M Banda M.D (BSC HB, MBCHB)Penias Max100% (1)
- Chapter Four: - Assessments of CommunityDocument37 pagesChapter Four: - Assessments of CommunityAbdurohaman BelayNo ratings yet
- Chapter II Literature ReviewDocument12 pagesChapter II Literature ReviewVictoria Husadani100% (3)
- 534622Document51 pages534622Diah WerdiiastutiiNo ratings yet
- Laboratory Activity 4.2Document5 pagesLaboratory Activity 4.2Paolo CampanoNo ratings yet
- Child HealthDocument5 pagesChild HealthRaju NiraulaNo ratings yet
- Nutrition Care ProcessDocument7 pagesNutrition Care ProcessALYSSA NICOLE GINESNo ratings yet
- Undesirable Body Mass Index Profiles in Young Adults: No One Is Immune To Obesity Epidemic in PakistanDocument5 pagesUndesirable Body Mass Index Profiles in Young Adults: No One Is Immune To Obesity Epidemic in PakistanDr Alamzeb JadoonNo ratings yet
- 14 NutritionalDocument57 pages14 NutritionalMulugeta EmiruNo ratings yet
- Project B EdDocument17 pagesProject B EdAnju VijayanNo ratings yet
- Healthy Status and Energy Balance in Pediatrics: Acta Bio-Medica: Atenei Parmensis February 2006Document8 pagesHealthy Status and Energy Balance in Pediatrics: Acta Bio-Medica: Atenei Parmensis February 2006zahfira edwardNo ratings yet
- Measuring Obesity 2Document11 pagesMeasuring Obesity 2Maged AllamNo ratings yet
- Group 1 (Alfeche, Bag-Ao, Cagatan, and Dela Cruz)Document4 pagesGroup 1 (Alfeche, Bag-Ao, Cagatan, and Dela Cruz)Faatoots FatsNo ratings yet
- Measuring Body CompositionDocument6 pagesMeasuring Body CompositionKamruzzaman Manik100% (1)
- 002 Pediatric Obesity An IntroductionDocument24 pages002 Pediatric Obesity An IntroductionAnurag BhatejaNo ratings yet
- Jebeile, 2022Document15 pagesJebeile, 2022cassio.mouraNo ratings yet
- Assessment of Nutritional Status of Children in Al Hilla CityDocument8 pagesAssessment of Nutritional Status of Children in Al Hilla CityKamruzzaman ManikNo ratings yet
- Childhood: EndingDocument68 pagesChildhood: EndingGiorgi KordzayaNo ratings yet
- Anthropometric Measurement To Identify Undernutrition in Cerabral PalsyDocument8 pagesAnthropometric Measurement To Identify Undernutrition in Cerabral PalsyPam Travezani MiyazakiNo ratings yet
- Lifetime Risk Childhood Obesity and CardiovascularDocument8 pagesLifetime Risk Childhood Obesity and CardiovascularLuis David Herrera MolinaresNo ratings yet
- Nutritional AssessmentDocument18 pagesNutritional AssessmentAliza ThakurNo ratings yet
- Moderate MalnutritionDocument10 pagesModerate MalnutritionReeya Delos SantosNo ratings yet
- JCDR - 2021Document4 pagesJCDR - 2021anbarasirajkumarNo ratings yet
- Nutrition AssessmentDocument47 pagesNutrition AssessmentMohamed F. Nada100% (6)
- Use of Nutrition Screening Initiative For Older AdultsDocument1 pageUse of Nutrition Screening Initiative For Older AdultsJoyce Kathreen Ebio LopezNo ratings yet
- Cardiometabolik Risk Jurnal (Terjemahan)Document10 pagesCardiometabolik Risk Jurnal (Terjemahan)kyoazaNo ratings yet
- Nutritional Assessement Anthropometric MethodsDocument77 pagesNutritional Assessement Anthropometric MethodsElias Libay100% (1)
- Midterm Module 4.1Document20 pagesMidterm Module 4.1angelaaapalingNo ratings yet
- Nutritional Status AssessmentDocument9 pagesNutritional Status AssessmentAna Paula SimplícioNo ratings yet
- Nutritional AssessmentDocument8 pagesNutritional AssessmentOutour KhNo ratings yet
- Methodology of Nns 2013Document13 pagesMethodology of Nns 2013Olive FactorizaNo ratings yet
- Assessment of Nutritional Status FinalDocument94 pagesAssessment of Nutritional Status FinalKasnhaNo ratings yet
- EatinghabitsobesityDocument10 pagesEatinghabitsobesityAngel GonzagaNo ratings yet
- Studies On The Correlation of Anthropometric Measurement With Health Outcome in ElderlyDocument8 pagesStudies On The Correlation of Anthropometric Measurement With Health Outcome in ElderlyAnis RanisNo ratings yet
- Body Mass Index:: Risks of Being Overweight (High BMI) and Physically InactiveDocument4 pagesBody Mass Index:: Risks of Being Overweight (High BMI) and Physically InactiveHuzaifa CHNo ratings yet
- 2 PDFDocument17 pages2 PDFnoerNo ratings yet
- How Can We Assess The Nutritional Status of An Individual 2155 9600 1000640Document2 pagesHow Can We Assess The Nutritional Status of An Individual 2155 9600 1000640alkhwarizmianinNo ratings yet
- Arid Agriculture University, Rawalpindi: Mid Exam / Spring 2021 (Paper Duration 12 Hours) To Be Filled by TeacherDocument30 pagesArid Agriculture University, Rawalpindi: Mid Exam / Spring 2021 (Paper Duration 12 Hours) To Be Filled by TeacherLaila LailaNo ratings yet
- Normal Weight Obesity SyndromeDocument13 pagesNormal Weight Obesity SyndromeMarcelo SabbatiniNo ratings yet
- Lab-Ncm 105-Learn-Mat Topic 2 2022-2023 1st SemDocument19 pagesLab-Ncm 105-Learn-Mat Topic 2 2022-2023 1st SemDobby AsahiNo ratings yet
- 121 Short Stature or at Risk of Short StatureDocument3 pages121 Short Stature or at Risk of Short Statureramadhanu100% (1)
- Literature Review of Overweight and Obese Children and Adults RevisionDocument11 pagesLiterature Review of Overweight and Obese Children and Adults RevisionIlyas BalochNo ratings yet
- A.N Unit 03Document26 pagesA.N Unit 03Hira KhanNo ratings yet
- Father Saturnino Urios University: San Francisco St. Butuan City 8600, Region XIII Caraga, PhilippinesDocument2 pagesFather Saturnino Urios University: San Francisco St. Butuan City 8600, Region XIII Caraga, PhilippinesChrizley Shawn DeroniaNo ratings yet
- MAJOR-SET Operating RoomDocument3 pagesMAJOR-SET Operating RoomChrizley Shawn DeroniaNo ratings yet
- Fluid and Electrolytes Cram SheetDocument8 pagesFluid and Electrolytes Cram SheetChrizley Shawn DeroniaNo ratings yet
- DRUG STUDY EldersDocument1 pageDRUG STUDY EldersChrizley Shawn DeroniaNo ratings yet
- Drug StudyDocument8 pagesDrug StudyChrizley Shawn DeroniaNo ratings yet
- Types of Sutures and LayersDocument4 pagesTypes of Sutures and LayersChrizley Shawn DeroniaNo ratings yet
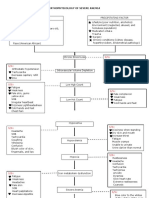
- Pathophysiology of Severe AnemiaDocument3 pagesPathophysiology of Severe AnemiaChrizley Shawn DeroniaNo ratings yet
- Nursing Care Plan Cues Diagnosis Planning Implementation Rationale EvaluationDocument3 pagesNursing Care Plan Cues Diagnosis Planning Implementation Rationale EvaluationChrizley Shawn DeroniaNo ratings yet
- EBR (CE Ward) 1 PDFDocument3 pagesEBR (CE Ward) 1 PDFChrizley Shawn DeroniaNo ratings yet
- Nursing Care Plan Cues Diagnosis Planning Implementation Rationale EvaluationDocument4 pagesNursing Care Plan Cues Diagnosis Planning Implementation Rationale EvaluationChrizley Shawn DeroniaNo ratings yet
- Drug Study: and Blurred VisionDocument2 pagesDrug Study: and Blurred VisionChrizley Shawn DeroniaNo ratings yet
- Nursing Care Plan: Cues Diagnosis Planning Implementation Rationale EvaluationDocument3 pagesNursing Care Plan: Cues Diagnosis Planning Implementation Rationale EvaluationChrizley Shawn DeroniaNo ratings yet
- Drug Study 1Document4 pagesDrug Study 1Chrizley Shawn DeroniaNo ratings yet
- Evidence - Based - Report No. 1 (CHN)Document3 pagesEvidence - Based - Report No. 1 (CHN)Chrizley Shawn DeroniaNo ratings yet
- Evidence - Based - Report No. 2 (CHN Duty Day 5)Document3 pagesEvidence - Based - Report No. 2 (CHN Duty Day 5)Chrizley Shawn DeroniaNo ratings yet
- Drug Study 1 (Postpartum Duty)Document3 pagesDrug Study 1 (Postpartum Duty)Chrizley Shawn DeroniaNo ratings yet
- Father Saturnino Urios University Nursing Program Urian Health Center Individual Treatment RecordDocument6 pagesFather Saturnino Urios University Nursing Program Urian Health Center Individual Treatment RecordChrizley Shawn DeroniaNo ratings yet
- NCP No. 1 (Postpartum Duty)Document2 pagesNCP No. 1 (Postpartum Duty)Chrizley Shawn DeroniaNo ratings yet
- EBR No. 1 - Antepartum Duty (DERONIA)Document2 pagesEBR No. 1 - Antepartum Duty (DERONIA)Chrizley Shawn DeroniaNo ratings yet
- Final Chapter Research Abm 1Document10 pagesFinal Chapter Research Abm 1Lemuel Umpad VillacortaNo ratings yet
- A Successful Occupational Health Nurse-Driven Health Promotion Program To Support Corporate SustainabilityDocument8 pagesA Successful Occupational Health Nurse-Driven Health Promotion Program To Support Corporate SustainabilitysriNo ratings yet
- Baked Oatmeal Cups With Cinnamon and RaisinsDocument2 pagesBaked Oatmeal Cups With Cinnamon and RaisinsJane Dela SernaNo ratings yet
- Grandjean A., Campbell S. - Hydration Fluids For Life PDFDocument50 pagesGrandjean A., Campbell S. - Hydration Fluids For Life PDFDumitru SimonovNo ratings yet
- Barking Dogs Seldom BiteDocument14 pagesBarking Dogs Seldom BiteChirag BansalNo ratings yet
- Pertemuan 11Document13 pagesPertemuan 11Siti NurjanahNo ratings yet
- Relationship Between Food, Nutrition and HealthDocument7 pagesRelationship Between Food, Nutrition and HealthSHAHIN67% (3)
- Hematocrit AnemiaDocument1 pageHematocrit Anemiadoppler_No ratings yet
- 12-3-13 Rodney RundownDocument5 pages12-3-13 Rodney Rundownapi-238851288No ratings yet
- Metformin-Induced Vitamin B12 Deficiency Presenting As A Peripheral NeuropathyDocument3 pagesMetformin-Induced Vitamin B12 Deficiency Presenting As A Peripheral NeuropathyPhil MassinNo ratings yet
- Help Us To Help You Manual - Juice Plus PDFDocument14 pagesHelp Us To Help You Manual - Juice Plus PDFheafelNo ratings yet
- Essay 1: Causes of AneroxiaDocument6 pagesEssay 1: Causes of Aneroxiakehan luNo ratings yet
- WIC Case StudyDocument3 pagesWIC Case Studydsaitta108No ratings yet
- 5 6102753493703984120-1Document206 pages5 6102753493703984120-1Mohammad Faizan MansooriNo ratings yet
- Research Proposal PaperDocument15 pagesResearch Proposal Paperapi-311724010No ratings yet
- PsychosisSelfCareJune22 V2DDocument115 pagesPsychosisSelfCareJune22 V2DLindseyRae ParkerNo ratings yet
- SeaCell Brochure en 20140826Document12 pagesSeaCell Brochure en 20140826Puneet SingalNo ratings yet
- Determination of Chemical Composition of Carob Pod (Ceratonia Siliqua LDocument6 pagesDetermination of Chemical Composition of Carob Pod (Ceratonia Siliqua LalhachmiNo ratings yet
- Comparison of Moringa Leaves and Elephant Grass Nutrition and Their Effect On Animal FeedingDocument17 pagesComparison of Moringa Leaves and Elephant Grass Nutrition and Their Effect On Animal FeedingNadiaNo ratings yet
- Cysticare Utipro Plus Urinary Infections 15 CapsulesDocument1 pageCysticare Utipro Plus Urinary Infections 15 CapsulesAnnapurna HirematNo ratings yet
- Tmp50a TMPDocument3 pagesTmp50a TMPFrontiersNo ratings yet
- bổ sung bột hạnh nhật và stevia trong hỗn hợp bột gạo làm bánh quyDocument12 pagesbổ sung bột hạnh nhật và stevia trong hỗn hợp bột gạo làm bánh quyQuangHiệpNo ratings yet
- Antenatal CareDocument11 pagesAntenatal CareManasi ChaskarNo ratings yet
- Overview of Food and Beverage IndustryDocument4 pagesOverview of Food and Beverage IndustryJack Chew67% (3)
- Health Psychology 1st Edition Frazier Test Bank 1Document36 pagesHealth Psychology 1st Edition Frazier Test Bank 1josephphillipskxscpqtazi100% (26)
- Nutrition Repaired)Document10 pagesNutrition Repaired)Brylle MirandaNo ratings yet
- DysphagiaDocument14 pagesDysphagiaLisbeth TurraNo ratings yet
- VegetarianismDocument3 pagesVegetarianismRadha K dasNo ratings yet
- A Nutrition and Conditioning Intervention For Natural Bodybuilding Contest Preparation: Case StudyDocument12 pagesA Nutrition and Conditioning Intervention For Natural Bodybuilding Contest Preparation: Case StudyTHIMMAPPANo ratings yet
- Living Things VocabularyDocument12 pagesLiving Things VocabularymonicatindallNo ratings yet