You might also like
- Acog Practice Bulletin: Antepartum Fetal SurveillanceDocument12 pagesAcog Practice Bulletin: Antepartum Fetal SurveillanceMariana Hernandez100% (10)
- 2.03B Fetal Assessment Part 2 (Dr. Candelario) PDFDocument7 pages2.03B Fetal Assessment Part 2 (Dr. Candelario) PDFjay lorenz joaquinNo ratings yet
- A Cog Practice Bulletin 175 Ultrasound in PregnancyDocument16 pagesA Cog Practice Bulletin 175 Ultrasound in Pregnancyansel7No ratings yet
- High Risk PregnancyDocument113 pagesHigh Risk PregnancyVivian Lajara100% (2)
- NCP - Gestational HypertensionDocument3 pagesNCP - Gestational HypertensionCameron De GuzmanNo ratings yet
- Antepartum Fetal Surveillance ACOG Bulletin 2014 PDFDocument11 pagesAntepartum Fetal Surveillance ACOG Bulletin 2014 PDFDanNo ratings yet
- Fetal Movements As A Predictor of HealthDocument8 pagesFetal Movements As A Predictor of HealthWordtreader PtNo ratings yet
- Post-Term Labor - NCPDocument8 pagesPost-Term Labor - NCPCameron De GuzmanNo ratings yet
- Instructional Learning Guide: Course Audit in Maternal and Child NursingDocument18 pagesInstructional Learning Guide: Course Audit in Maternal and Child NursingMaynard PascualNo ratings yet
- Lecture Notes AnatomyDocument18 pagesLecture Notes AnatomyFau Fau DheoboNo ratings yet
- Intraabdominal Mass in NewbornDocument8 pagesIntraabdominal Mass in NewbornSridhar KaushikNo ratings yet
- Smith - Diagnosis and Management of Female InfertilityDocument4 pagesSmith - Diagnosis and Management of Female InfertilityAmanda SaphiraNo ratings yet
- Fetal Biophysical Profile: Antepartum and Intrapartum Fetal Assessment $8.00 .OODocument21 pagesFetal Biophysical Profile: Antepartum and Intrapartum Fetal Assessment $8.00 .OOFabricio EguíaNo ratings yet
- Abdominal Masses in The Newborn: Marshall Z. Schwartz, MD, and Donald B. Shaul, MDTDocument10 pagesAbdominal Masses in The Newborn: Marshall Z. Schwartz, MD, and Donald B. Shaul, MDTAditya Rahman RYNo ratings yet
- NCP On Postpartum MotherDocument9 pagesNCP On Postpartum MotherM.S.H Tube100% (1)
- NCP Gestational HypertensionDocument3 pagesNCP Gestational HypertensionCameron De GuzmanNo ratings yet
- Altered Uteroplacental Tissue PerfusionDocument5 pagesAltered Uteroplacental Tissue PerfusionArielle BajalaNo ratings yet
- Post-Term Pregnancy Emergency C-Section Due to Non-Reassuring Fetal Heart RateDocument7 pagesPost-Term Pregnancy Emergency C-Section Due to Non-Reassuring Fetal Heart RateCameron De GuzmanNo ratings yet
- Evaluation of Fetal Well Being ZİYA KALEMDocument49 pagesEvaluation of Fetal Well Being ZİYA KALEMSal TlsNo ratings yet
- Antenatal Fetal SurveillanceDocument115 pagesAntenatal Fetal SurveillanceNargis1000100% (1)
- Altered Tissue Perfusion UteroplacentalDocument4 pagesAltered Tissue Perfusion UteroplacentalAlyNo ratings yet
- 11-Evaluation of Fetal Well-Being Nov2000Document7 pages11-Evaluation of Fetal Well-Being Nov2000api-3703352No ratings yet
- Manning ScoreDocument10 pagesManning ScoreYurike Natalie LengkongNo ratings yet
- Non-invasive assessment of fetal well-beingDocument7 pagesNon-invasive assessment of fetal well-beingCT Johara MusorNo ratings yet
- Antepartum Fetal MonitoringDocument9 pagesAntepartum Fetal MonitoringDoc Prince CaballeroNo ratings yet
- 1 s2.0 S0002937822000424 MainDocument12 pages1 s2.0 S0002937822000424 MainHillary AchachNo ratings yet
- MALPRESENTATIONDocument13 pagesMALPRESENTATIONLady Jane CaguladaNo ratings yet
- Au Ca1-Clp - 01-Dexel Lorren R. Valdez Ob DownloadableDocument2 pagesAu Ca1-Clp - 01-Dexel Lorren R. Valdez Ob DownloadableDexel Lorren ValdezNo ratings yet
- Profil Biofisik High RiskDocument5 pagesProfil Biofisik High RiskbebekbebekNo ratings yet
- Ecoobstetrica Acog2016Document16 pagesEcoobstetrica Acog2016John VegaNo ratings yet
- First Page PDFDocument1 pageFirst Page PDFtirusew beleNo ratings yet
- Case Stud1.editedDocument12 pagesCase Stud1.editedNahshon UnsimilarNo ratings yet
- Client Initials: Medical Diagnosis: Cephalopelvic Disproportion Eu DEFINITION: The RelationshipDocument2 pagesClient Initials: Medical Diagnosis: Cephalopelvic Disproportion Eu DEFINITION: The RelationshipLyssa Monique67% (3)
- Task IncomingDocument14 pagesTask Incomingmonica mittiamNo ratings yet
- Ovarian Reserve Testing: A User's Guide: Expert ReviewsDocument12 pagesOvarian Reserve Testing: A User's Guide: Expert ReviewsYosep SutandarNo ratings yet
- Ultrasound in Infertility PDFDocument11 pagesUltrasound in Infertility PDFDrFarah Emad AliNo ratings yet
- Cervical Mucus Analysis: A Major Component in Evaluation of InfertilityDocument4 pagesCervical Mucus Analysis: A Major Component in Evaluation of InfertilityfifahcantikNo ratings yet
- Fetal Biophysical Profile: Decreased Fetal BreathingDocument5 pagesFetal Biophysical Profile: Decreased Fetal BreathingYuly Andrea Marquez CastañedaNo ratings yet
- 1 - Antenatal AssessmentDocument44 pages1 - Antenatal AssessmentIbrahim RamizNo ratings yet
- Fetal DistressDocument10 pagesFetal DistressLady Jane CaguladaNo ratings yet
- 2017-Journal of Paediatrics and Child HealthDocument1 page2017-Journal of Paediatrics and Child HealthAna SopaNo ratings yet
- Abdominal Masses in The NewbornDocument9 pagesAbdominal Masses in The NewbornBella MesantikaNo ratings yet
- 175 Ultrasound in Pregnancy PDFDocument16 pages175 Ultrasound in Pregnancy PDFNestor FerrerNo ratings yet
- Evidence-Based Labor Management - Induction of Labor (II) AJOG Nov-2020Document11 pagesEvidence-Based Labor Management - Induction of Labor (II) AJOG Nov-2020Andrea SerranoNo ratings yet
- Evidence-Based Guidelines for Induction of LaborDocument11 pagesEvidence-Based Guidelines for Induction of LaborAndrea SerranoNo ratings yet
- Resume Jurnal: No. Jurnal Objectives Design Materials and Methods Result or ConclusionDocument20 pagesResume Jurnal: No. Jurnal Objectives Design Materials and Methods Result or ConclusionJhati Degal SacioNo ratings yet
- 20 BPPDocument23 pages20 BPPbenNo ratings yet
- Ramos-2bn NCP Delivery RoomDocument2 pagesRamos-2bn NCP Delivery RoomLouwella RamosNo ratings yet
- Antepartum Fetal Well Being AssessmentDocument14 pagesAntepartum Fetal Well Being AssessmentIsrael WoseneNo ratings yet
- Medical management of abnormal uterine bleedingDocument14 pagesMedical management of abnormal uterine bleedingdiegoesteban1234No ratings yet
- Evaluation of Fetal Well BeingDocument22 pagesEvaluation of Fetal Well BeingJoanah Mae AsuncionNo ratings yet
- VASA Previa CaseDocument3 pagesVASA Previa CasewijeNo ratings yet
- Menstrual Cycle Related Disorders: Volume 7: Frontiers in Gynecological EndocrinologyFrom EverandMenstrual Cycle Related Disorders: Volume 7: Frontiers in Gynecological EndocrinologySarah L. BergaNo ratings yet
- Leptin: Regulation and Clinical ApplicationsFrom EverandLeptin: Regulation and Clinical ApplicationsSam Dagogo-Jack, MDNo ratings yet
- Ovulation Induction and Controlled Ovarian Stimulation: A Practical GuideFrom EverandOvulation Induction and Controlled Ovarian Stimulation: A Practical GuideNo ratings yet
- Hormones and Embryonic Development: Advances in the BiosciencesFrom EverandHormones and Embryonic Development: Advances in the BiosciencesG. RaspéNo ratings yet
- Diminished Ovarian Reserve and Assisted Reproductive Technologies: Current Research and Clinical ManagementFrom EverandDiminished Ovarian Reserve and Assisted Reproductive Technologies: Current Research and Clinical ManagementOrhan BukulmezNo ratings yet
- Dental Management of the Pregnant PatientFrom EverandDental Management of the Pregnant PatientChristos A. SkouterisNo ratings yet
- Medical School Companion Obstetrics and Gynecology Practice Question BookFrom EverandMedical School Companion Obstetrics and Gynecology Practice Question BookNo ratings yet
- MAJOR-SET Operating RoomDocument3 pagesMAJOR-SET Operating RoomChrizley Shawn DeroniaNo ratings yet
- DRUG STUDY EldersDocument1 pageDRUG STUDY EldersChrizley Shawn DeroniaNo ratings yet
- Father Saturnino Urios University: San Francisco St. Butuan City 8600, Region XIII Caraga, PhilippinesDocument2 pagesFather Saturnino Urios University: San Francisco St. Butuan City 8600, Region XIII Caraga, PhilippinesChrizley Shawn DeroniaNo ratings yet
- Electrolyte and Fluid Imbalances ChartDocument8 pagesElectrolyte and Fluid Imbalances ChartChrizley Shawn DeroniaNo ratings yet
- Types of Sutures and LayersDocument4 pagesTypes of Sutures and LayersChrizley Shawn DeroniaNo ratings yet
- Reducing heavy menstrual bleeding with Tranexamic AcidDocument8 pagesReducing heavy menstrual bleeding with Tranexamic AcidChrizley Shawn DeroniaNo ratings yet
- Drug Study: and Blurred VisionDocument2 pagesDrug Study: and Blurred VisionChrizley Shawn DeroniaNo ratings yet
- EBR (CE Ward) 1 PDFDocument3 pagesEBR (CE Ward) 1 PDFChrizley Shawn DeroniaNo ratings yet
- NCP Samples Related To NutritionDocument15 pagesNCP Samples Related To NutritionChrizley Shawn DeroniaNo ratings yet
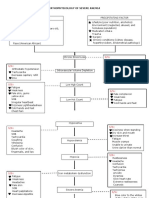
- Pathophysiology of Severe AnemiaDocument3 pagesPathophysiology of Severe AnemiaChrizley Shawn DeroniaNo ratings yet
- Nursing Care Plan: Cues Diagnosis Planning Implementation Rationale EvaluationDocument3 pagesNursing Care Plan: Cues Diagnosis Planning Implementation Rationale EvaluationChrizley Shawn DeroniaNo ratings yet
- Drug Study 1Document4 pagesDrug Study 1Chrizley Shawn DeroniaNo ratings yet
- Evidence - Based - Report No. 1 (CHN)Document3 pagesEvidence - Based - Report No. 1 (CHN)Chrizley Shawn DeroniaNo ratings yet
- Nursing Care Plan Cues Diagnosis Planning Implementation Rationale EvaluationDocument3 pagesNursing Care Plan Cues Diagnosis Planning Implementation Rationale EvaluationChrizley Shawn DeroniaNo ratings yet
- Evidence - Based - Report No. 2 (CHN Duty Day 5)Document3 pagesEvidence - Based - Report No. 2 (CHN Duty Day 5)Chrizley Shawn DeroniaNo ratings yet
- EBR No. 1 - Antepartum Duty (DERONIA)Document2 pagesEBR No. 1 - Antepartum Duty (DERONIA)Chrizley Shawn DeroniaNo ratings yet
- NCP No. 1 (Postpartum Duty)Document2 pagesNCP No. 1 (Postpartum Duty)Chrizley Shawn DeroniaNo ratings yet
- Father Saturnino Urios University Nursing Program Urian Health Center Individual Treatment RecordDocument6 pagesFather Saturnino Urios University Nursing Program Urian Health Center Individual Treatment RecordChrizley Shawn DeroniaNo ratings yet
- Drug Study 1 (Postpartum Duty)Document3 pagesDrug Study 1 (Postpartum Duty)Chrizley Shawn DeroniaNo ratings yet
- Ultrasound - A GuideDocument9 pagesUltrasound - A GuideDebasish KunduNo ratings yet
- BreastfeedingDocument19 pagesBreastfeedingShubhankar KatariyaNo ratings yet
- IX. Drug StudyDocument11 pagesIX. Drug StudyRizza ReyesNo ratings yet
- Group 2B Case Study On Ectopic PregnancyDocument36 pagesGroup 2B Case Study On Ectopic PregnancyANGEL GADONo ratings yet
- Obstetrics and GynaecologyDocument7 pagesObstetrics and GynaecologyCherry KolaNo ratings yet
- KRCRC VFC Summer2021Document8 pagesKRCRC VFC Summer2021Carol SavkovichNo ratings yet
- Laporan Data Barang PT MONDY INTI PERSADADocument25 pagesLaporan Data Barang PT MONDY INTI PERSADARomandaniNo ratings yet
- Early Marrige Practices and Perception of Badjao in Inognong Bataraza PalawanDocument38 pagesEarly Marrige Practices and Perception of Badjao in Inognong Bataraza PalawanJonalyn Adjarani DiazNo ratings yet
- Medical Termination of Pregnancy (MTP) Act DR Seema Mehrotra Associate Professor Dept of OB&GYNDocument48 pagesMedical Termination of Pregnancy (MTP) Act DR Seema Mehrotra Associate Professor Dept of OB&GYNMasuma YesminNo ratings yet
- Wernestrup Syndrome or Variant of Vacterl Association - Case ReportDocument2 pagesWernestrup Syndrome or Variant of Vacterl Association - Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
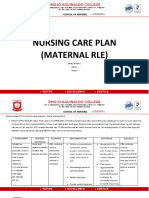
- Nursing Care Plan (Maternal Rle) : Emilio Aguinaldo CollegeDocument9 pagesNursing Care Plan (Maternal Rle) : Emilio Aguinaldo CollegeKyle De Sagun Oteda100% (2)
- Embryology, Pathophysiology, and Ultrasound Characteristics of The Placenta ObjectivesDocument13 pagesEmbryology, Pathophysiology, and Ultrasound Characteristics of The Placenta ObjectivesAudrey100% (5)
- The Development of FrogDocument13 pagesThe Development of FrogRhonnel Manatad AlburoNo ratings yet
- Surrogacy Laws in India Through YearsDocument16 pagesSurrogacy Laws in India Through YearsAngel GeorgeNo ratings yet
- Perpetuation of Life ExamDocument2 pagesPerpetuation of Life ExamLouise Meara Severo100% (1)
- BBLRDocument14 pagesBBLRDhevi NiaNo ratings yet
- Garbhaprada Yogas PDFDocument6 pagesGarbhaprada Yogas PDFprasadNo ratings yet
- q3 Sci10 Unit1 Feedback MechanismsDocument125 pagesq3 Sci10 Unit1 Feedback MechanismsIvann EboraNo ratings yet
- CLASSIFICATION OF MILKING COWS For FeedingDocument6 pagesCLASSIFICATION OF MILKING COWS For FeedingJahanzeb SafdarNo ratings yet
- Antenatal Corticosteroids in Preterm Labour PDFDocument3 pagesAntenatal Corticosteroids in Preterm Labour PDFSanjay RabdeNo ratings yet
- Pre Gestational ConditionsDocument68 pagesPre Gestational ConditionsQuinonez Anna MarieNo ratings yet
- Cflga 2022Document9 pagesCflga 2022Hedjarah MulokNo ratings yet
- Science PTDocument9 pagesScience PTorpillaleah27No ratings yet
- POSTPARTUM CARE HandoutsDocument3 pagesPOSTPARTUM CARE HandoutsJulia Rae Delos SantosNo ratings yet
- Down SyndromeDocument9 pagesDown Syndromeapi-479463379No ratings yet
- Embryo MCQ 9 ItemsDocument2 pagesEmbryo MCQ 9 ItemsBeda MalecdanNo ratings yet
- Dysmenorrhoea in Adult WomenDocument16 pagesDysmenorrhoea in Adult Womenfarmasi_hm100% (1)
- NCM109 RLE 1st Term ReviewerDocument40 pagesNCM109 RLE 1st Term ReviewerCarelle Faith Serrano AsuncionNo ratings yet
- Placenta and Amniotic Fluid Structure FunctionDocument66 pagesPlacenta and Amniotic Fluid Structure FunctionmadyNo ratings yet
- Class-XII Biology (Theory) Design of The Question Paper: 1. Weightage of Contents / Subject Units Units Content MarkDocument99 pagesClass-XII Biology (Theory) Design of The Question Paper: 1. Weightage of Contents / Subject Units Units Content MarkMahaNo ratings yet