You might also like
- Medical School Companion Obstetrics and Gynecology Practice Question BookFrom EverandMedical School Companion Obstetrics and Gynecology Practice Question BookNo ratings yet
- 02-History-Taking-In-OBGYN-DrAyman - Copy - PpsDocument26 pages02-History-Taking-In-OBGYN-DrAyman - Copy - PpsSworupKhadkaNo ratings yet
- Practical of Arterial Pulse For 1st Year Mbbs StudentsDocument7 pagesPractical of Arterial Pulse For 1st Year Mbbs StudentsMudassar Roomi0% (2)
- (4X - A5) - 08161373182 - Shelf-Life Obgyn 2015 PDFDocument358 pages(4X - A5) - 08161373182 - Shelf-Life Obgyn 2015 PDFcmbhganteng80% (5)
- Anatomy For The Gynecologic OncologistDocument70 pagesAnatomy For The Gynecologic OncologistjroshsperlingNo ratings yet
- Pregnancy Tests Explained (2Nd Edition): Current Trends of Antenatal TestsFrom EverandPregnancy Tests Explained (2Nd Edition): Current Trends of Antenatal TestsNo ratings yet
- Acog Practice Bulletin: Antepartum Fetal SurveillanceDocument12 pagesAcog Practice Bulletin: Antepartum Fetal SurveillanceMariana Hernandez100% (10)
- Subjetive: Long Term: Independent:: RationaleDocument1 pageSubjetive: Long Term: Independent:: RationaleRyann BuayaNo ratings yet
- Opioid-Free Anesthesia - JaDocument29 pagesOpioid-Free Anesthesia - JanitaNo ratings yet
- Lecture On Cardiac Cycle by DR RoomiDocument43 pagesLecture On Cardiac Cycle by DR RoomiMudassar Roomi100% (2)
- Michigan Manual of Neonatal Intejnsive Care 3rd Ed NBDocument559 pagesMichigan Manual of Neonatal Intejnsive Care 3rd Ed NBeugazz8980% (5)
- Induction of LaborDocument8 pagesInduction of LaborwiwimbakNo ratings yet
- PID Treatment and CausesDocument17 pagesPID Treatment and CausesGhaliey AzizNo ratings yet
- Feton FillingDocument8 pagesFeton Fillingkunalprabhu148No ratings yet
- A Novel of Typhoid Mary: FEVER by Mary Beth KeaneDocument16 pagesA Novel of Typhoid Mary: FEVER by Mary Beth KeaneSimon and Schuster95% (19)
- Marconi 2008Document6 pagesMarconi 2008Sri HariNo ratings yet
- Zhao2015 PDFDocument9 pagesZhao2015 PDFmavarthavaNo ratings yet
- Knee Chest Position To Reduce The Incidence of Breech PresentationDocument5 pagesKnee Chest Position To Reduce The Incidence of Breech PresentationNoviaNo ratings yet
- Supported By: None.: AbstractsDocument1 pageSupported By: None.: AbstractsFerry DimyatiNo ratings yet
- 1OudGvy8RaUCS I6Ynenp qqBDDAJMOPoDocument13 pages1OudGvy8RaUCS I6Ynenp qqBDDAJMOPoJan Rey G. PelagioNo ratings yet
- Safety and Efficacy of Misoprostol in Induction of Labour in Prelabour Rupture of Fetal Membrane in Nigerian Women: A Multicenter StudyDocument6 pagesSafety and Efficacy of Misoprostol in Induction of Labour in Prelabour Rupture of Fetal Membrane in Nigerian Women: A Multicenter StudyAnonymous GssdN5No ratings yet
- Assessment of Labor Progression by Intrapartum Ultrasonography Among Term Nulliparous WomenDocument5 pagesAssessment of Labor Progression by Intrapartum Ultrasonography Among Term Nulliparous WomenFrancesca Doreen VegaNo ratings yet
- Poster Session II: ConclusionDocument2 pagesPoster Session II: ConclusionFahmi Nur SuwandiNo ratings yet
- Diagnosis of PTL IGF Seth GS Med College 2017Document6 pagesDiagnosis of PTL IGF Seth GS Med College 2017Pinky RanwaNo ratings yet
- Original Article Symphysio Fundal Height (SFH) Measurement As A Predictor of Birth WeightDocument5 pagesOriginal Article Symphysio Fundal Height (SFH) Measurement As A Predictor of Birth Weightyudha adi saputaNo ratings yet
- Baseline variability in normal term births and neonatal depressionDocument2 pagesBaseline variability in normal term births and neonatal depressionKathleenNo ratings yet
- The Preterm Labor Index and Fetal Fibronectin For.24Document6 pagesThe Preterm Labor Index and Fetal Fibronectin For.24bombonlrNo ratings yet
- Perinatal Outcomes of Pregnancies Wâth Borderline Amniotic Xuid IndexDocument3 pagesPerinatal Outcomes of Pregnancies Wâth Borderline Amniotic Xuid IndexDiana SchlittlerNo ratings yet
- Comparison Between Three Methods of Fetal Weight Estimation During The Active Stage of Labor Performed by Residents: A Prospective Cohort StudyDocument7 pagesComparison Between Three Methods of Fetal Weight Estimation During The Active Stage of Labor Performed by Residents: A Prospective Cohort StudyMahida El shafiNo ratings yet
- Intrapartum Ultrasound Assessment of FetDocument8 pagesIntrapartum Ultrasound Assessment of FetXymon ZubietaNo ratings yet
- Cervical Ripening Methods Compared for Labor InductionDocument5 pagesCervical Ripening Methods Compared for Labor InductionSri HariNo ratings yet
- Manning ScoreDocument10 pagesManning ScoreYurike Natalie LengkongNo ratings yet
- Piis0015028211013112 PDFDocument2 pagesPiis0015028211013112 PDFGayathriMaranNo ratings yet
- Persistence of Fetal Memory Into Neonatal LifeDocument5 pagesPersistence of Fetal Memory Into Neonatal LifeRodrigo LeãoNo ratings yet
- MF 07038Document9 pagesMF 07038Tuan PhanNo ratings yet
- Medicine: A Double-Blinded, Randomized, Placebo-Controlled Trial Assessing The Effects of Nifedipine On Embryo TransferDocument5 pagesMedicine: A Double-Blinded, Randomized, Placebo-Controlled Trial Assessing The Effects of Nifedipine On Embryo TransferAkbar Rabani MugayatNo ratings yet
- Fetal Movements As A Predictor of HealthDocument8 pagesFetal Movements As A Predictor of HealthWordtreader PtNo ratings yet
- Usg ObstetrikDocument22 pagesUsg ObstetrikPutri Aini DaulayNo ratings yet
- 2017-Journal of Paediatrics and Child HealthDocument1 page2017-Journal of Paediatrics and Child HealthAna SopaNo ratings yet
- Treatment With Piroxicam Before Embryo Transfer Increases The Pregnancy Rate After in Vitro Fertilization and Embryo TransferDocument5 pagesTreatment With Piroxicam Before Embryo Transfer Increases The Pregnancy Rate After in Vitro Fertilization and Embryo TransferVasantham HospitalNo ratings yet
- PROFILE OF INDUCED LABOUR IN UNCOMPLICATED PREGNANCIES WITH UNFAVOURABLE MODIFIEDS BISHOP SCORE IN A TERTIARY CARE CENTREDocument8 pagesPROFILE OF INDUCED LABOUR IN UNCOMPLICATED PREGNANCIES WITH UNFAVOURABLE MODIFIEDS BISHOP SCORE IN A TERTIARY CARE CENTREIJAR JOURNALNo ratings yet
- Día Transfer. Labarta 1Document6 pagesDía Transfer. Labarta 1AnaNo ratings yet
- Relation of maternal positions on NST results and comfortDocument6 pagesRelation of maternal positions on NST results and comfortzaenab anissaNo ratings yet
- Procedures and Techniques-Clinical: ArtDocument2 pagesProcedures and Techniques-Clinical: ArtGeos KarNo ratings yet
- 2006 Cephalopelvic Disproportion Is Associated With An Altered Uterine Contraction Shape in The Active Phase of Labor. AJOGDocument4 pages2006 Cephalopelvic Disproportion Is Associated With An Altered Uterine Contraction Shape in The Active Phase of Labor. AJOGayupurnamasariiNo ratings yet
- Single Versus Double Intrauterine Insemination in Controlled Ovarian Stimulation Cycles For Subfertile MalesDocument6 pagesSingle Versus Double Intrauterine Insemination in Controlled Ovarian Stimulation Cycles For Subfertile MalesmasdipoNo ratings yet
- Dawes 2019Document10 pagesDawes 2019Marco Julcamoro AsencioNo ratings yet
- Evaluation of Fetal Well Being ZİYA KALEMDocument49 pagesEvaluation of Fetal Well Being ZİYA KALEMSal TlsNo ratings yet
- 2017 Julio Comunidad y SaludDocument3 pages2017 Julio Comunidad y SaludremediosisabelNo ratings yet
- Does Acupuncture Influence the Endometrium and IVF OutcomesDocument7 pagesDoes Acupuncture Influence the Endometrium and IVF OutcomesdirkvandeweyerNo ratings yet
- Impact of Oligohydramnios On Maternal and PerinataDocument6 pagesImpact of Oligohydramnios On Maternal and PerinataDiana SchlittlerNo ratings yet
- Misoprostol SL Vs VAGDocument5 pagesMisoprostol SL Vs VAGAgus WijayaNo ratings yet
- Acta Obstet Gynecol Scand - 2011 - MARIA PATERNOSTER - Cervical phIGFBP 1 in The Evaluation of The Risk of Preterm deDocument5 pagesActa Obstet Gynecol Scand - 2011 - MARIA PATERNOSTER - Cervical phIGFBP 1 in The Evaluation of The Risk of Preterm dePriscilla GeraldineNo ratings yet
- Natural History of Fetal Position During Pregnancy.11Document6 pagesNatural History of Fetal Position During Pregnancy.11PutriNo ratings yet
- Tugas Kelompok Kegawatdaruratan (Pre-Eklamsi)Document6 pagesTugas Kelompok Kegawatdaruratan (Pre-Eklamsi)FeniNo ratings yet
- Deh 001Document4 pagesDeh 001syid rosyidNo ratings yet
- The NeoUpdates - DecDocument7 pagesThe NeoUpdates - DecDr Satish MishraNo ratings yet
- Induction of Labor With Misoprostol For Premature Rupture of Membranes Beyond Thirty-Six Weeks' GestationDocument6 pagesInduction of Labor With Misoprostol For Premature Rupture of Membranes Beyond Thirty-Six Weeks' GestationFebrinata MahadikaNo ratings yet
- Valor Predictivo Monitoreo FetalDocument6 pagesValor Predictivo Monitoreo FetalElena ZepedaNo ratings yet
- Doppler and Biophysical Assessment in Growth Restricted Fetuses: Distribution of Test ResultsDocument7 pagesDoppler and Biophysical Assessment in Growth Restricted Fetuses: Distribution of Test ResultslalimdNo ratings yet
- International Journal of Gynecology and ObstetricsDocument6 pagesInternational Journal of Gynecology and ObstetricsmerawatidyahsepitaNo ratings yet
- Low Antimullerian Hormone Levels Improve Fertility Outcome in Patients With Polycystic Ovary Syndrome 1665Document5 pagesLow Antimullerian Hormone Levels Improve Fertility Outcome in Patients With Polycystic Ovary Syndrome 1665GayathriMaranNo ratings yet
- Retrospective Analysis of Risk Factors For Low 1-Minute Apgar Scores in Term NeonatesDocument10 pagesRetrospective Analysis of Risk Factors For Low 1-Minute Apgar Scores in Term Neonatesputri vinia /ilove cuteNo ratings yet
- Theriogenology: Elaine M.U. Gil, Daniela A.A. Garcia, Tilde R. FroesDocument6 pagesTheriogenology: Elaine M.U. Gil, Daniela A.A. Garcia, Tilde R. FroesIngrid MachadoNo ratings yet
- Estimated Fetal Weight: Comparison of Clinical Versus Ultrasound EstimateDocument6 pagesEstimated Fetal Weight: Comparison of Clinical Versus Ultrasound EstimateNadia AyuningtiasNo ratings yet
- 33219-Article Text-97197-1-10-20201204Document6 pages33219-Article Text-97197-1-10-20201204ZisuhNo ratings yet
- Third Trimester Ultrasound Scan Combined With A Clinical Method For Accurate Birthweight Prediction at Term: A Cohort Study in SpainDocument12 pagesThird Trimester Ultrasound Scan Combined With A Clinical Method For Accurate Birthweight Prediction at Term: A Cohort Study in SpainRegina PizanNo ratings yet
- Lukaszuk Et Al. - 2005 - Optimization of Estradiol Supplementation During The Luteal Phase Improves The Pregnancy Rate in Women UnderDocument5 pagesLukaszuk Et Al. - 2005 - Optimization of Estradiol Supplementation During The Luteal Phase Improves The Pregnancy Rate in Women UnderKrzysztof ŁukaszukNo ratings yet
- Comparison of Nifedipine and Bed Rest For Inhibiting Threatened Preterm Labour 2161 0932.1000131Document4 pagesComparison of Nifedipine and Bed Rest For Inhibiting Threatened Preterm Labour 2161 0932.1000131muhammad maadaNo ratings yet
- Esteves2 PDFDocument4 pagesEsteves2 PDFGunther MirandaNo ratings yet
- Diminished Ovarian Reserve and Assisted Reproductive Technologies: Current Research and Clinical ManagementFrom EverandDiminished Ovarian Reserve and Assisted Reproductive Technologies: Current Research and Clinical ManagementOrhan BukulmezNo ratings yet
- Perinatal Hypoxia Ischemia and Brain InjuryDocument2 pagesPerinatal Hypoxia Ischemia and Brain InjurybebekbebekNo ratings yet
- Precancerous Lesions in Gynecology: Prof. Herman Susanto, DR., Spog (K) - OnkDocument29 pagesPrecancerous Lesions in Gynecology: Prof. Herman Susanto, DR., Spog (K) - OnkbebekbebekNo ratings yet
- Antibiotic Prophylaxis in Obstetric Procedures PDFDocument7 pagesAntibiotic Prophylaxis in Obstetric Procedures PDFHallaHisanHartotoNo ratings yet
- Peashooter Life CycleDocument23 pagesPeashooter Life CyclebebekbebekNo ratings yet
- Management of The Obstetric Antiphospholipid Syndrome: ReviewDocument12 pagesManagement of The Obstetric Antiphospholipid Syndrome: ReviewbebekbebekNo ratings yet
- Holmes and Rahe Stress ScaleDocument7 pagesHolmes and Rahe Stress ScalebebekbebekNo ratings yet
- Postpartum Pain Management PDFDocument9 pagesPostpartum Pain Management PDFYovinus DenyNo ratings yet
- Assessment of Fetal Lung MaturityDocument2 pagesAssessment of Fetal Lung MaturitybebekbebekNo ratings yet
- The Cause and Treatment of Recurrent Pregnancy LossDocument6 pagesThe Cause and Treatment of Recurrent Pregnancy LossbebekbebekNo ratings yet
- Fetal Biophysical Profile. A Critical Appraisal PDFDocument11 pagesFetal Biophysical Profile. A Critical Appraisal PDFchronos6534No ratings yet
- Antiphospholipid SyndromeDocument12 pagesAntiphospholipid SyndromebebekbebekNo ratings yet
- Antiphospholipid SyndromeDocument12 pagesAntiphospholipid SyndromebebekbebekNo ratings yet
- Time To Say GodbyeDocument7 pagesTime To Say GodbyebebekbebekNo ratings yet
- Adhesion Development and Morbidity After Repeat Cesarean DeliveryDocument6 pagesAdhesion Development and Morbidity After Repeat Cesarean DeliverybebekbebekNo ratings yet
- XF-30A-30 (Veterinary) User ManualDocument40 pagesXF-30A-30 (Veterinary) User ManualMai Thanh SơnNo ratings yet
- Ibnu Sina Hospital, Tuesday, April 19th, 2022 (Period April 10th - 17th, 2022)Document4 pagesIbnu Sina Hospital, Tuesday, April 19th, 2022 (Period April 10th - 17th, 2022)MirahAvishaNo ratings yet
- Medicine: Bachelor of Medicine and Bachelor of Surgery (MBBS)Document32 pagesMedicine: Bachelor of Medicine and Bachelor of Surgery (MBBS)nidaNo ratings yet
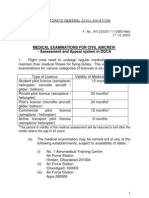
- Medical - Appeal Procedure DGCADocument6 pagesMedical - Appeal Procedure DGCAБисвас АнупамNo ratings yet
- Abdul Malik Hassim Lecturer DMA Management & Science UniversityDocument21 pagesAbdul Malik Hassim Lecturer DMA Management & Science UniversitykimmgizelleNo ratings yet
- New Case StudyDocument26 pagesNew Case Studyfaisal saifNo ratings yet
- Curriculum Vitae Summary for Orthopaedic SpecialistDocument5 pagesCurriculum Vitae Summary for Orthopaedic SpecialistShaoran AuliaNo ratings yet
- Twins Identical and FraternalDocument3 pagesTwins Identical and Fraternalteju2812No ratings yet
- The Construction of Medical Disposal Medical Sociology and Medical Problem Solving in Practice CareDocument31 pagesThe Construction of Medical Disposal Medical Sociology and Medical Problem Solving in Practice CareCronopialmenteNo ratings yet
- Cirrus 4000Document8 pagesCirrus 4000Francisco GomezNo ratings yet
- 100 ThoughtsDocument3 pages100 Thoughtsraju_pnNo ratings yet
- NucRadSHARE Kamal Singh USDocument9 pagesNucRadSHARE Kamal Singh USFurman BorstNo ratings yet
- Application and Resignation LetterDocument5 pagesApplication and Resignation LetterEricka Jordan AberinNo ratings yet
- Epithelial Tumours - SreejaDocument184 pagesEpithelial Tumours - SreejaaakiNo ratings yet
- Gail Luskin ResumeDocument3 pagesGail Luskin Resumeapi-260548731No ratings yet
- Prof. Dr. Markolf Niemz Lecture Notes Exam PrepDocument35 pagesProf. Dr. Markolf Niemz Lecture Notes Exam PrepSanaa Numan MohammedNo ratings yet
- Scientific TeamDocument4 pagesScientific TeampriyadikkalaNo ratings yet
- 245-Medcfgen-07-20-C - Clinical Fellow Gen Med JD PSDocument7 pages245-Medcfgen-07-20-C - Clinical Fellow Gen Med JD PSMohammad LouayNo ratings yet
- Latihan Tangan Untuk CTSDocument6 pagesLatihan Tangan Untuk CTStrioNo ratings yet
- Electrosurgery Catalog 9757RevJDocument42 pagesElectrosurgery Catalog 9757RevJFlorentina Delca BealcuNo ratings yet