You might also like
- WEEK 15 Pediatric Neuro and Muskuloskeletal DisordersDocument91 pagesWEEK 15 Pediatric Neuro and Muskuloskeletal Disordersrising starNo ratings yet
- Peripheral NeuropathiesDocument25 pagesPeripheral NeuropathieslabertoNo ratings yet
- NCM 209 PediaDocument76 pagesNCM 209 PediaJohn Cyprian AbeloNo ratings yet
- FCPS Surgery 26 Aug 2023 (M)Document16 pagesFCPS Surgery 26 Aug 2023 (M)Tauseef AfridiNo ratings yet
- Multiple SlerosisDocument3 pagesMultiple SlerosisTrishia GuillermoNo ratings yet
- Medical-Surgical Nursing: Primary Brain TumorDocument20 pagesMedical-Surgical Nursing: Primary Brain TumorYejiNo ratings yet
- Responses To Altered PerceptionDocument74 pagesResponses To Altered PerceptionANDREA JUSTINE CARDEÑONo ratings yet
- Medical Surgical Nursing Review NotesDocument76 pagesMedical Surgical Nursing Review Notesnot your medz duranNo ratings yet
- Neurologic AssessmentDocument8 pagesNeurologic AssessmentHNo ratings yet
- Medical Surgical Nursing Review NotesDocument81 pagesMedical Surgical Nursing Review NotesBernadeth Josefa BorelaNo ratings yet
- Nervous System Path (MSN) PDFDocument150 pagesNervous System Path (MSN) PDFRodrigoMendozaNo ratings yet
- Autonomic DiseasesDocument3 pagesAutonomic DiseasesAli 10No ratings yet
- History Taking in Nervous SystemDocument18 pagesHistory Taking in Nervous Systemdrvinodg2000No ratings yet
- Cancer of The ProstateDocument3 pagesCancer of The ProstateCamille Joy BaliliNo ratings yet
- Clase Cefalea 2016Document60 pagesClase Cefalea 2016Juliana AndradeNo ratings yet
- PRM EkortsDocument3 pagesPRM EkortsAmira Vianca RiveraNo ratings yet
- Brain AbscessDocument1 pageBrain AbscesscelladorapNo ratings yet
- Cerebrovascular Accident CVADocument40 pagesCerebrovascular Accident CVAjaphethNo ratings yet
- Eent DisordersDocument5 pagesEent DisordersalctheyNo ratings yet
- Cerebrovascular Accident CVADocument40 pagesCerebrovascular Accident CVAAndrea IlaidaNo ratings yet
- Sesi 1 - 02 - Emergency in Spine InjuryDocument34 pagesSesi 1 - 02 - Emergency in Spine Injurydr.gunturadwiNo ratings yet
- Assessment and Diagnostic ExamsDocument21 pagesAssessment and Diagnostic ExamsNicole AlcoberNo ratings yet
- Nervous CompiledDocument18 pagesNervous CompiledGeraldine MaeNo ratings yet
- Alt. Communication/ Motor FunctionDocument11 pagesAlt. Communication/ Motor Functionapi-3822433No ratings yet
- NCM118 TransesDocument11 pagesNCM118 TransesAlejandro Saclolo, IIINo ratings yet
- CNSDocument16 pagesCNSnarjesNo ratings yet
- NIRVE Main CaseDocument52 pagesNIRVE Main CaseGerald PagalingNo ratings yet
- Unconscious and Comatose Patients DR Moses KazevuDocument17 pagesUnconscious and Comatose Patients DR Moses KazevuMoses Jr KazevuNo ratings yet
- Prion Diseases: Dinusha Yagama de Silva Group 11 Semester 7Document30 pagesPrion Diseases: Dinusha Yagama de Silva Group 11 Semester 7Tom perryNo ratings yet
- Disorders of ConsciousnessDocument6 pagesDisorders of ConsciousnessJessa BuenoNo ratings yet
- Oral SURGERY REVALIDA1Document27 pagesOral SURGERY REVALIDA1Bea Y. Bas-ongNo ratings yet
- Lumbar Puncture-2Document24 pagesLumbar Puncture-2Aditya rajNo ratings yet
- Nervous System Booklet by Win Nursing Coaching - 240301 - 210829Document46 pagesNervous System Booklet by Win Nursing Coaching - 240301 - 210829kanimozhithirugnanamNo ratings yet
- NEURODocument10 pagesNEUROreooooNo ratings yet
- Head Injury: Closed Head Injury EG: Falls, Motor Vehicle Crashes, Bicycle InjuriesDocument13 pagesHead Injury: Closed Head Injury EG: Falls, Motor Vehicle Crashes, Bicycle InjuriesJudy HandlyNo ratings yet
- Temporaledh 1Document14 pagesTemporaledh 1Atikah PurnamasariNo ratings yet
- 03 Anatomo-Physiological Peculiarities of The Nervous SystemDocument88 pages03 Anatomo-Physiological Peculiarities of The Nervous SystemashishanandaakNo ratings yet
- NeurologyDocument37 pagesNeurologyDevangkumar PatelNo ratings yet
- 9 5神經系統Document59 pages9 5神經系統陳姿螢No ratings yet
- Clinical Therapeutics Case No.16: Presented By: Maria Cristina CastroDocument65 pagesClinical Therapeutics Case No.16: Presented By: Maria Cristina CastroMichelle Vera GabunNo ratings yet
- Health Assessment HandoutDocument4 pagesHealth Assessment HandoutRoselily Flores CoquillaNo ratings yet
- Group 1.2 Case StudyDocument19 pagesGroup 1.2 Case Studychandria0026No ratings yet
- Neuro - Sir Chavez - AS OF 12PMDocument5 pagesNeuro - Sir Chavez - AS OF 12PMCarl JustineNo ratings yet
- Elective - Neurologic Reporting 1Document23 pagesElective - Neurologic Reporting 1GenEsis CarandangNo ratings yet
- Autoimmune DisordersDocument13 pagesAutoimmune Disordersinah krizia lagueNo ratings yet
- 2 Af 5 VERTIGODocument35 pages2 Af 5 VERTIGOmuneceNo ratings yet
- UNCONSCIOUSNESSDocument61 pagesUNCONSCIOUSNESSVidhuma VidhumaNo ratings yet
- Birth Trauma IN Newborns: DR Vanessa Lee Wan Mun Paediatrician Hospital Melaka 23 OCTOBER 2018Document28 pagesBirth Trauma IN Newborns: DR Vanessa Lee Wan Mun Paediatrician Hospital Melaka 23 OCTOBER 2018Cupin DeNo ratings yet
- Neurocutaneous Syndromes & CPDocument5 pagesNeurocutaneous Syndromes & CPMahmoud emadNo ratings yet
- Handouts - Neurological Assessment & Spinal TapDocument8 pagesHandouts - Neurological Assessment & Spinal TapGodfrey Bag-aoNo ratings yet
- Podział Diagnostyka PDFDocument9 pagesPodział Diagnostyka PDFMagda KupczyńskaNo ratings yet
- Head InjuriesDocument7 pagesHead Injuriesapi-3822433100% (1)
- Case 5 SeizureDocument17 pagesCase 5 SeizureGrace Tanajura100% (2)
- Brain Tumor.Document19 pagesBrain Tumor.Mission JupiterNo ratings yet
- Neuroradiology: Dr. Dhanti Erma, SP - RadDocument64 pagesNeuroradiology: Dr. Dhanti Erma, SP - RadizzkibipNo ratings yet
- Respiratory Term 2Document13 pagesRespiratory Term 2Abegail QuintoNo ratings yet
- Neurology ExaminationDocument31 pagesNeurology ExaminationEtana AdamNo ratings yet
- Care of Clients With Neurologic Deficit: By: Elmer G. Organia, RNDocument233 pagesCare of Clients With Neurologic Deficit: By: Elmer G. Organia, RNTina TalmadgeNo ratings yet
- How The Brain Works: Understanding Brain Function, Thought and PersonalityFrom EverandHow The Brain Works: Understanding Brain Function, Thought and PersonalityNo ratings yet
- Being Fiercely Present: Overcoming Trauma Difficulties in Mindfulness PracticeFrom EverandBeing Fiercely Present: Overcoming Trauma Difficulties in Mindfulness PracticeNo ratings yet
- CDN Post Test Answer KeyDocument5 pagesCDN Post Test Answer KeyCharme Jean Raygon100% (1)
- Cardio Post TestDocument13 pagesCardio Post TestCharme Jean RaygonNo ratings yet
- NURSING PHARMACOLOGY REVIEW Mix GroupDocument47 pagesNURSING PHARMACOLOGY REVIEW Mix GroupCharme Jean RaygonNo ratings yet
- Trancu NotesDocument4 pagesTrancu NotesCharme Jean RaygonNo ratings yet
- Drugs 1Document5 pagesDrugs 1Charme Jean RaygonNo ratings yet
- LABORATORYDocument6 pagesLABORATORYCharme Jean RaygonNo ratings yet
- Gastro Meningitis NCPDocument8 pagesGastro Meningitis NCPCharme Jean RaygonNo ratings yet
- Normal and Critical Lab ValuesDocument14 pagesNormal and Critical Lab ValuesCharme Jean RaygonNo ratings yet
- Pa-2 0Document3 pagesPa-2 0Charme Jean RaygonNo ratings yet
- TOP DRUGS - Doc Version 1Document12 pagesTOP DRUGS - Doc Version 1Charme Jean RaygonNo ratings yet
- NCM 119 Final ReviewerDocument15 pagesNCM 119 Final ReviewerCharme Jean RaygonNo ratings yet
- Mental HealthDocument3 pagesMental HealthCharme Jean RaygonNo ratings yet
- Theoretical Framework StrokeDocument1 pageTheoretical Framework StrokeCharme Jean RaygonNo ratings yet
- Leadership Final ReviewerDocument16 pagesLeadership Final ReviewerCharme Jean RaygonNo ratings yet
- ETOH Case StudyDocument5 pagesETOH Case StudyCharme Jean RaygonNo ratings yet
- Area To Be Assesed Normal Findings Actual Findings AnalysisDocument3 pagesArea To Be Assesed Normal Findings Actual Findings AnalysisCharme Jean RaygonNo ratings yet
- IV Flow Computation QuizDocument7 pagesIV Flow Computation QuizCharme Jean RaygonNo ratings yet
- Operating Room Instruments Delivery Room InstrumentsDocument5 pagesOperating Room Instruments Delivery Room InstrumentsCharme Jean RaygonNo ratings yet
- Supplementary Table 6. Severity of Solicited Adverse EventsDocument1 pageSupplementary Table 6. Severity of Solicited Adverse EventsCharme Jean RaygonNo ratings yet
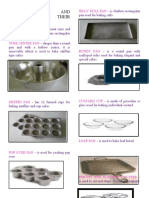
- Baking Tools and Equipment and Their Uses: Cake PanDocument6 pagesBaking Tools and Equipment and Their Uses: Cake PanCharme Jean RaygonNo ratings yet
- Vaccine: SciencedirectDocument6 pagesVaccine: SciencedirectCharme Jean RaygonNo ratings yet
- Index: Crit Care Nurs Clin N Am 18 (2006) 433-439Document7 pagesIndex: Crit Care Nurs Clin N Am 18 (2006) 433-439Charme Jean RaygonNo ratings yet
- 2DMT MT639 LEC - Third ShiftingDocument68 pages2DMT MT639 LEC - Third ShiftingKAREN DELA CRUZNo ratings yet
- Carotid Artery Disease FlyerDocument2 pagesCarotid Artery Disease Flyerdinh son myNo ratings yet
- Candida VulvovaginitisDocument20 pagesCandida VulvovaginitisVicobeingoNo ratings yet
- DAV Public School, Hehal, Ranchi Monday Test, Class-XI M.M-25 Subject-English Time - 1 HourDocument3 pagesDAV Public School, Hehal, Ranchi Monday Test, Class-XI M.M-25 Subject-English Time - 1 HourSHIVAM KUMAR SINGHNo ratings yet
- Movie Analysis A Moment To RememberDocument7 pagesMovie Analysis A Moment To RememberJoia De LeonNo ratings yet
- Sas 15 MCN Lec 2Document3 pagesSas 15 MCN Lec 2Jhoanna Marie VillaverdeNo ratings yet
- Why Is Alcohol An Instigator of ViolenceDocument4 pagesWhy Is Alcohol An Instigator of Violencearniel somilNo ratings yet
- DR Ackermans Display Clinical Case Dez12Document29 pagesDR Ackermans Display Clinical Case Dez12Kollinz ZfNo ratings yet
- Hemorrhagic Unilateral RetinopathyDocument7 pagesHemorrhagic Unilateral RetinopathyHanna_RNo ratings yet
- National Adult Clozapine Titration ChartDocument2 pagesNational Adult Clozapine Titration ChartCarla VieiraNo ratings yet
- Blood Questions 2Document6 pagesBlood Questions 2Omar HNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument2 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationKim SungaNo ratings yet
- Article Trailer Script and Sources. ScriptDocument2 pagesArticle Trailer Script and Sources. ScriptEvol 9897No ratings yet
- Cefotaxime 1Document3 pagesCefotaxime 1DidikNo ratings yet
- Argumentative Text (Graphic Organizer) - LauretaDocument1 pageArgumentative Text (Graphic Organizer) - LauretaPaul Vincent LauretaNo ratings yet
- Proposal RawDocument12 pagesProposal RawSedem StanisloveNo ratings yet
- IV. Modul 10 - Pengelolaan NyeriDocument97 pagesIV. Modul 10 - Pengelolaan NyeriGrace Noviyanthi SinambelaNo ratings yet
- Rhinitis AllergicDocument9 pagesRhinitis AllergicWiny Ch'amhada TtarudaNo ratings yet
- What Is AutismDocument2 pagesWhat Is AutismTimothy Teh Ewe TimNo ratings yet
- Pathology DKDocument367 pagesPathology DKAshok DaukiyaNo ratings yet
- Clinical Manifestations and Assessment of Respiratory Disease 5th Edition Jardins Test BankDocument9 pagesClinical Manifestations and Assessment of Respiratory Disease 5th Edition Jardins Test Banksarahpalmerotpdkjcwfq100% (26)
- Confronting and Coping With Multidrug-Resistant TuDocument9 pagesConfronting and Coping With Multidrug-Resistant TuDWI HERU CAHYONONo ratings yet
- Bag Valve Mask Ventilation: Topic OutlineDocument4 pagesBag Valve Mask Ventilation: Topic OutlineDan Dan ManaoisNo ratings yet
- 162 - 4187 - Hermina Novida - GalleyDocument5 pages162 - 4187 - Hermina Novida - Galleyaulia fikriNo ratings yet
- Impact of Covid 19 On EnvironmentDocument20 pagesImpact of Covid 19 On EnvironmentRamkishan JaiswarNo ratings yet
- Emmanuel A Etim 2017Document4 pagesEmmanuel A Etim 2017Shafici CqadirNo ratings yet
- CNS DrugsDocument57 pagesCNS DrugsHussein Al-jmrawiNo ratings yet
- Clincial Quetsions Urinary and Bowel Reterntion Student VersionDocument4 pagesClincial Quetsions Urinary and Bowel Reterntion Student VersionDesha Gelles-SotoNo ratings yet
- Co-Occurring Disorders: Substance Use and Mental HealthDocument52 pagesCo-Occurring Disorders: Substance Use and Mental HealthElisyah MarsiahNo ratings yet
- Patofisiologi VenaDocument5 pagesPatofisiologi VenaNisa AriyantiiNo ratings yet