You might also like
- Pharmacology SummaryDocument16 pagesPharmacology Summaryshenric16No ratings yet
- Systolic Dysfunction:: Types of Heart FailureDocument13 pagesSystolic Dysfunction:: Types of Heart FailureElisabeth F. OjhaNo ratings yet
- L7 Heart Failure Practice EssayDocument2 pagesL7 Heart Failure Practice EssaymoshlingmomoNo ratings yet
- Cvs DrugsDocument106 pagesCvs DrugsIkoona ivanNo ratings yet
- Cardiac Care and COVID-19: Perspectives in Medical PracticeFrom EverandCardiac Care and COVID-19: Perspectives in Medical PracticeNo ratings yet
- Heart Failure: Low Output HF High Output HFDocument7 pagesHeart Failure: Low Output HF High Output HFJake BurrNo ratings yet
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtFrom EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtRating: 5 out of 5 stars5/5 (1)
- CVPR Prototype Drugs TableDocument27 pagesCVPR Prototype Drugs TablethommyvaNo ratings yet
- 4 - Anti-AnginaDocument6 pages4 - Anti-AnginaJericho De GuzmanNo ratings yet
- Pharm Guide Quiz 1 Parasyp and Symp Nervous SystemDocument5 pagesPharm Guide Quiz 1 Parasyp and Symp Nervous SystemMaryNguyenNo ratings yet
- Mechanism of Action: Cerebral VasospasmDocument1 pageMechanism of Action: Cerebral VasospasmArjay Oamil GuerreroNo ratings yet
- CarvedilolDocument4 pagesCarvedilolGoNo ratings yet
- CombinepdfDocument27 pagesCombinepdfMICHAEL ANGELO CUBIONo ratings yet
- Cardio Lab MedsDocument11 pagesCardio Lab MedsDianne Erika MeguinesNo ratings yet
- Heart Failure: Mohammad DiahDocument50 pagesHeart Failure: Mohammad DiahAdityaNo ratings yet
- Cardiotonics - DR Anoosha BhandarkarDocument60 pagesCardiotonics - DR Anoosha BhandarkaranooshabhandarkarNo ratings yet
- HypertensionDocument43 pagesHypertensionAbin PNo ratings yet
- CVS & Hypolipidemic Drugs-NursingDocument71 pagesCVS & Hypolipidemic Drugs-NursingManikanta Guptha100% (1)
- Cardiac ReflexesDocument2 pagesCardiac ReflexesfeliciaNo ratings yet
- 6 Beta Adrenergic BlockersDocument19 pages6 Beta Adrenergic Blockersmatchees-gone rogue100% (1)
- Pharm 00 B14Document2 pagesPharm 00 B14DonkeyManNo ratings yet
- Department of Clinical Pharmacology: Pharmacotherapy of Chronic Ischemic Heart DiseaseDocument84 pagesDepartment of Clinical Pharmacology: Pharmacotherapy of Chronic Ischemic Heart DiseasePatty ReyesNo ratings yet
- Congestive Heart FailureDocument30 pagesCongestive Heart FailurePh OmarNo ratings yet
- Anti Anginal Drugs - Wards HandooutDocument24 pagesAnti Anginal Drugs - Wards HandooutDharun RanganathanNo ratings yet
- Drugs Used in HF IIDocument40 pagesDrugs Used in HF IIJamal LudinNo ratings yet
- PharmaAntianginal DrugsDocument175 pagesPharmaAntianginal DrugsNidal AbboudNo ratings yet
- 11A Drugs Acting On The Cardiovascular SystemDocument85 pages11A Drugs Acting On The Cardiovascular SystemJaps De la CruzNo ratings yet
- Pharmacologyofccf 181227034555Document43 pagesPharmacologyofccf 181227034555MohammedMujahedNo ratings yet
- Heart Failure: Kalaiselvan OtDocument46 pagesHeart Failure: Kalaiselvan Otplayme_nowNo ratings yet
- Beta-Adrenergic BlockersDocument14 pagesBeta-Adrenergic BlockersAnonymous NVAWeVWNo ratings yet
- Cardiology Review: HTN: Julia Akaah M.DDocument40 pagesCardiology Review: HTN: Julia Akaah M.DJose LunaNo ratings yet
- Vasodilators and The Treatment of Angina PectorisDocument39 pagesVasodilators and The Treatment of Angina PectorisRose AnnNo ratings yet
- Meds #1 NotesDocument4 pagesMeds #1 NotesAnh TrinhNo ratings yet
- Controlled Hypotension: Moderator: DR V. Y. Srinivas Presenter: Dr. Ann Susan MathewDocument49 pagesControlled Hypotension: Moderator: DR V. Y. Srinivas Presenter: Dr. Ann Susan MathewAnn Susan MathewNo ratings yet
- Calcium Channel BlockersDocument4 pagesCalcium Channel BlockersHarold LinNo ratings yet
- Drugs For Heart Failure & Angina: Department of Pharmacology Liming Zhou 2010,3Document47 pagesDrugs For Heart Failure & Angina: Department of Pharmacology Liming Zhou 2010,3DR Muhammad Abdul BasitNo ratings yet
- شDocument16 pagesشhqzcgdh6gvNo ratings yet
- Heart Failure: S. Soliman MDDocument46 pagesHeart Failure: S. Soliman MDRamli HusenNo ratings yet
- Heart Failure New SlidesDocument41 pagesHeart Failure New SlidesjawadNo ratings yet
- Heart FailureDocument9 pagesHeart Failuregmqkxq6wshNo ratings yet
- Beta Blockers BPTHDocument45 pagesBeta Blockers BPTHjyb5kcxbgtNo ratings yet
- Heart Failure: DR - Liu LixinDocument46 pagesHeart Failure: DR - Liu LixinsanjivdasNo ratings yet
- Antihypertensive DrugsDocument7 pagesAntihypertensive Drugshamadadodo7No ratings yet
- Cardio CHF Angina Drugs MegDocument3 pagesCardio CHF Angina Drugs MegJhonny pingolNo ratings yet
- Lecture #12Document3 pagesLecture #12yeeticusfinchlmaoNo ratings yet
- 4.heart Failure HandoutDocument108 pages4.heart Failure HandoutGetachewNo ratings yet
- Pharmacotherapy of Hypertention TerbaruDocument45 pagesPharmacotherapy of Hypertention TerbarulisaNo ratings yet
- Calcium Channel BlockersDocument28 pagesCalcium Channel Blockershap hazardNo ratings yet
- USMLE Step 1 NotesDocument5 pagesUSMLE Step 1 NotesMarie SantoroNo ratings yet
- Inotropic Agents - Blockers Renin InhibitorsDocument19 pagesInotropic Agents - Blockers Renin InhibitorsTanyir MarieClaireNo ratings yet
- Inotropic Agents - Blockers Renin InhibitorsDocument19 pagesInotropic Agents - Blockers Renin InhibitorslitaNo ratings yet
- Pharmacology RCR1 RenalDocument6 pagesPharmacology RCR1 RenaleamcrawleyNo ratings yet
- SyncopeDocument44 pagesSyncopeSap ModulesNo ratings yet
- Anti-Arrhythmic Agents For Pharmacy PDFDocument41 pagesAnti-Arrhythmic Agents For Pharmacy PDFKelvinTMaikanaNo ratings yet
- 5 Hypertension Handout PDFDocument20 pages5 Hypertension Handout PDFMd Sakil AminNo ratings yet
- Cardio, Otis, Ortho, and GI Drug ListsDocument4 pagesCardio, Otis, Ortho, and GI Drug ListsJodi Gugel DeMarrowNo ratings yet
- CEACCP - Intrathecal Opioids in The Management of Acute Postoperative PainDocument5 pagesCEACCP - Intrathecal Opioids in The Management of Acute Postoperative PainDonkeyManNo ratings yet
- Pharm 02 A10Document2 pagesPharm 02 A10DonkeyManNo ratings yet
- CEACCP - Latex AllergyDocument4 pagesCEACCP - Latex AllergyDonkeyManNo ratings yet
- Physiol 93 B3Document1 pagePhysiol 93 B3DonkeyManNo ratings yet
- CEACCP - KetamineDocument5 pagesCEACCP - KetamineDonkeyManNo ratings yet
- CEACCP - Illegal Substances in Anaesthetic and Intensive Care PracticesDocument5 pagesCEACCP - Illegal Substances in Anaesthetic and Intensive Care PracticesDonkeyManNo ratings yet
- Pharm 00 B15Document2 pagesPharm 00 B15DonkeyManNo ratings yet
- Pharm 00 B14Document2 pagesPharm 00 B14DonkeyManNo ratings yet
- Pharm 02 A11Document4 pagesPharm 02 A11DonkeyManNo ratings yet
- Pharm 00 A15Document2 pagesPharm 00 A15DonkeyManNo ratings yet
- Pharm 00 A12Document1 pagePharm 00 A12DonkeyManNo ratings yet
- Compare and Contrast Neostigmine and The Organophosphate CompoundsDocument1 pageCompare and Contrast Neostigmine and The Organophosphate CompoundsDonkeyManNo ratings yet
- Pharm 00 A14Document2 pagesPharm 00 A14DonkeyManNo ratings yet
- Outline The Physiological Consequences of Hyperosmolar Diabetic KetoacidosisDocument2 pagesOutline The Physiological Consequences of Hyperosmolar Diabetic KetoacidosisDonkeyManNo ratings yet
- Compare and Contrast The Pharmacology of Esmolol and PropanololDocument1 pageCompare and Contrast The Pharmacology of Esmolol and PropanololDonkeyManNo ratings yet
- Pharm 00 B11Document1 pagePharm 00 B11DonkeyManNo ratings yet
- Pharm 00 A9Document2 pagesPharm 00 A9DonkeyManNo ratings yet
- Compare and Contrast Atropine and Glycopyrulate, and Discuss The Clinical ImplicationsDocument2 pagesCompare and Contrast Atropine and Glycopyrulate, and Discuss The Clinical ImplicationsDonkeyManNo ratings yet
- Compare and Contrast The Pharamcology of Ephedrine and NoradrenalineDocument1 pageCompare and Contrast The Pharamcology of Ephedrine and NoradrenalineDonkeyManNo ratings yet
- VOLATILEAGENTSDocument4 pagesVOLATILEAGENTSDonkeyManNo ratings yet
- FS Antimicrobial Dosing Obesity AMS Updates Issue4 - Nov2018Document4 pagesFS Antimicrobial Dosing Obesity AMS Updates Issue4 - Nov2018DonkeyManNo ratings yet
- Palliative Care HandbookDocument82 pagesPalliative Care HandbookDonkeyManNo ratings yet
- The Physiology of The GIT and The Liver QuestionsDocument44 pagesThe Physiology of The GIT and The Liver QuestionsDonkeyManNo ratings yet
- Comparative Pharmacokinetics of Fentanyl and Alfentanil: Br. J. Anaesth. (1982), 54, 871Document7 pagesComparative Pharmacokinetics of Fentanyl and Alfentanil: Br. J. Anaesth. (1982), 54, 871DonkeyManNo ratings yet
- Cholinergic Agents: Cholinergic Receptors Types of Receptor Muscarinic Receptor Nicotinic ReceptorDocument4 pagesCholinergic Agents: Cholinergic Receptors Types of Receptor Muscarinic Receptor Nicotinic ReceptorDonkeyManNo ratings yet
- Base Excess (Be) Measure of Metabolic Acid-Base Status: Dr. David LynessDocument1 pageBase Excess (Be) Measure of Metabolic Acid-Base Status: Dr. David LynessDonkeyManNo ratings yet
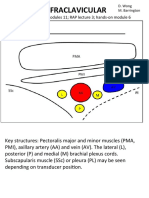
- Infraclavicular: Toolbox: Online Modules 11 RAP Lecture 3 Hands - On Module 6Document4 pagesInfraclavicular: Toolbox: Online Modules 11 RAP Lecture 3 Hands - On Module 6DonkeyManNo ratings yet
- HEARTDocument11 pagesHEART1NC21IS038 POLATHALA MOUNIKANo ratings yet
- The ESC Textbook of Sports CardiologyDocument478 pagesThe ESC Textbook of Sports CardiologyIBFiS100% (1)
- Case Study With ECG Reading OcañaDocument3 pagesCase Study With ECG Reading OcañaNicole Chloe OcanaNo ratings yet
- The Cardiovascular System: Elaine N. MariebDocument46 pagesThe Cardiovascular System: Elaine N. MariebIvann Chan MunarNo ratings yet
- Biventricular Pacing For Atrioventricular Block and Systolic DysfunctionDocument9 pagesBiventricular Pacing For Atrioventricular Block and Systolic DysfunctionRaul OrtegaNo ratings yet
- Nursing Care Plan AnswerDocument6 pagesNursing Care Plan Answercoosa liquorsNo ratings yet
- Experience With A Chest Pain CenterDocument8 pagesExperience With A Chest Pain CenterGabriel Cadavid GilNo ratings yet
- Clinical Application of The EchocardiogtamDocument39 pagesClinical Application of The EchocardiogtamStella CooKeyNo ratings yet
- Basic Life Support Program - Andhra Medical CollegeDocument6 pagesBasic Life Support Program - Andhra Medical CollegeRajasekhar BandiNo ratings yet
- ECG Physician's Guide (Japanese)Document49 pagesECG Physician's Guide (Japanese)Mohammad NasriNo ratings yet
- Congestive Heart FailureDocument25 pagesCongestive Heart FailuredevianiamalinaNo ratings yet
- Nuclear Cardiology: Role in The World of Multimodality Cardiac ImagingDocument5 pagesNuclear Cardiology: Role in The World of Multimodality Cardiac ImagingElena FlorentinaNo ratings yet
- NCLEX Based 1000 MCQs Part-2Document12 pagesNCLEX Based 1000 MCQs Part-2AkashNo ratings yet
- Angiografi Koroner: Indikasi, Kontraindikasi, Dan Proteksi Terhadap RadiasiDocument6 pagesAngiografi Koroner: Indikasi, Kontraindikasi, Dan Proteksi Terhadap Radiasihindri royiah fatmaNo ratings yet
- Pathologt of The HeartDocument40 pagesPathologt of The HeartJudithNo ratings yet
- Systolic MurmursDocument10 pagesSystolic MurmursRizqan Fahlevvi AkbarNo ratings yet
- Amiodarone Vs Sotalol GroupDocument12 pagesAmiodarone Vs Sotalol GroupIrving H Torres LopezNo ratings yet
- Coarctation of Aorta: Seoul National University Hospital Department of Thoracic & Cardiovascular SurgeryDocument39 pagesCoarctation of Aorta: Seoul National University Hospital Department of Thoracic & Cardiovascular Surgeryprencess_jeny5006No ratings yet
- Heart Disease and Stroke Statistics-2023 Update: A Report From The American Heart AssociationDocument529 pagesHeart Disease and Stroke Statistics-2023 Update: A Report From The American Heart Association涂育寬No ratings yet
- 4 - Congenital Heart DefectDocument42 pages4 - Congenital Heart DefectAlfiya HasnaNo ratings yet
- Anesthesiology: Linda S. Aglio Richard D. UrmanDocument457 pagesAnesthesiology: Linda S. Aglio Richard D. UrmanDaia DaiaNo ratings yet
- Heart Lung InteractionDocument39 pagesHeart Lung InteractionziadNo ratings yet
- Biology Investigatory Project: Congenital Heart DiseaseDocument16 pagesBiology Investigatory Project: Congenital Heart DiseaseDraco MalfoyNo ratings yet
- Cardiac Drug FunctionDocument2 pagesCardiac Drug FunctionShanda Rieder KozickiNo ratings yet
- Acute Inferior Myocardial InfarctionDocument1 pageAcute Inferior Myocardial InfarctionLogadarshini VeerasamyNo ratings yet
- Cardiac Cycle by Preetibala Sahu-1Document17 pagesCardiac Cycle by Preetibala Sahu-1aksahu01234No ratings yet
- Short Cases in Clinical Exams of Internal Medicine (PDFDrive)Document185 pagesShort Cases in Clinical Exams of Internal Medicine (PDFDrive)Nadhirah ZulkifliNo ratings yet
- Perimount Theon: Carpentier-Edwards Mitral Pericardial BioprosthesisDocument4 pagesPerimount Theon: Carpentier-Edwards Mitral Pericardial BioprosthesisJose Miguel GonzalezNo ratings yet
- Circulation: Ms. Jonalyn P. SantosDocument18 pagesCirculation: Ms. Jonalyn P. SantosHoward John M. RamiterreNo ratings yet
- NR 161:cardiology Study Guide Cardiology Study GuideDocument6 pagesNR 161:cardiology Study Guide Cardiology Study GuideApril Danielle TeschNo ratings yet