You might also like
- Newman's Billing and Coding Technicians Study GuideFrom EverandNewman's Billing and Coding Technicians Study GuideRating: 4.5 out of 5 stars4.5/5 (2)
- Week 13 Documentation in Psychiatric Mental Health Nursing PracticeDocument69 pagesWeek 13 Documentation in Psychiatric Mental Health Nursing PracticeJeff MalinisNo ratings yet
- NursingDocument57 pagesNursingremzylicious100% (1)
- NCM 103a-W1-Charting-or-Documentation-Module-1Document6 pagesNCM 103a-W1-Charting-or-Documentation-Module-1Nathaniel PulidoNo ratings yet
- Document It RightDocument61 pagesDocument It RightMacrossBala100% (1)
- Neonatal Ventilation, Step by StepDocument99 pagesNeonatal Ventilation, Step by StepMarely Ovando Castillo93% (14)
- Lesson 1-Documentation and ReportingDocument8 pagesLesson 1-Documentation and ReportingCHRISTIAN ROY MAXINO100% (1)
- Ensure Safe Continuity of Psychiatric CareDocument37 pagesEnsure Safe Continuity of Psychiatric CareMARIA STEPHANY DELA CRUZNo ratings yet
- PatientCareDocDocument15 pagesPatientCareDocAra- Cvsu Francisco100% (2)
- Newman's Certified Electronic Health Records Technician Study GuideFrom EverandNewman's Certified Electronic Health Records Technician Study GuideNo ratings yet
- Nursing DocumentationDocument17 pagesNursing Documentationprema100% (4)
- Health Record Documentation in Acute CareDocument8 pagesHealth Record Documentation in Acute Careapi-340699040No ratings yet
- Maintenance of Records and ReportsDocument81 pagesMaintenance of Records and ReportsSanjna Kumari (SNSR Senior Tutor/Lecturer)100% (1)
- Documentation and ReportingDocument32 pagesDocumentation and ReportingBryan Mae H. Degorio100% (1)
- Nursing Process and Documentation GuideDocument52 pagesNursing Process and Documentation Guidegeorgeloto12100% (2)
- Documentation: Basic Nursing: Foundations of Skills & Concepts DocumentationDocument8 pagesDocumentation: Basic Nursing: Foundations of Skills & Concepts DocumentationJona GarzonNo ratings yet
- DCM601A51 - Technical DataDocument405 pagesDCM601A51 - Technical Datathanhthuan100% (1)
- Unit 1 Documentation-and-ReportingDocument39 pagesUnit 1 Documentation-and-ReportingMs.V. Mahesha Asst. Prof.No ratings yet
- Documenting and Reporting: CommunicationDocument5 pagesDocumenting and Reporting: CommunicationDanielle Cachero100% (1)
- C C C M MMMM MM M MMM 3mm MMMMM MM M MMMMMDocument4 pagesC C C M MMMM MM M MMM 3mm MMMMM MM M MMMMMjohkieNo ratings yet
- Documentation & Reporting in Nursing - EFNDocument4 pagesDocumentation & Reporting in Nursing - EFNadellia onyNo ratings yet
- Handouts-IV Therapy Documentation PDFDocument12 pagesHandouts-IV Therapy Documentation PDFTony DemaguilNo ratings yet
- Documentation in Psychiatric Mental Health Nursing Practice: Course Unit 13Document15 pagesDocumentation in Psychiatric Mental Health Nursing Practice: Course Unit 13MARIA STEPHANY DELA CRUZNo ratings yet
- Records and Reports-AnuDocument89 pagesRecords and Reports-AnuNithiya NadesanNo ratings yet
- Nursing ProcessDocument52 pagesNursing ProcessDzon LornaNo ratings yet
- Nicu DoccumentationDocument17 pagesNicu Doccumentationchaarvi100% (1)
- Documenting and Reporting LEARNING OUTCOMES After Completing This ChapterDocument29 pagesDocumenting and Reporting LEARNING OUTCOMES After Completing This Chaptertwy113No ratings yet
- Unidrive Classic User Guide PDFDocument195 pagesUnidrive Classic User Guide PDFkukaNo ratings yet
- Changing Mainline IV BagDocument5 pagesChanging Mainline IV BagLorna PaghunasanNo ratings yet
- Documenting and ReportingDocument17 pagesDocumenting and ReportingalelichengNo ratings yet
- Documentation and ReportingDocument51 pagesDocumentation and ReportingYsabella LlanetaNo ratings yet
- Midterms - HA LabDocument17 pagesMidterms - HA LabMa. Daniela De la CernaNo ratings yet
- Documenting and ReportingDocument5 pagesDocumenting and ReportingElla LobenariaNo ratings yet
- HA-Midterms LabDocument13 pagesHA-Midterms LabMa. Daniela De la CernaNo ratings yet
- NCM-101 - Module-7 - 2Document39 pagesNCM-101 - Module-7 - 2Princess Javier TorcelinoNo ratings yet
- Week 1011 Guidelines Protocols Tools in Documentation Related To Client CareDocument59 pagesWeek 1011 Guidelines Protocols Tools in Documentation Related To Client CareobnimagashelinaNo ratings yet
- Nursing Documentation & ReportingDocument5 pagesNursing Documentation & ReportingMeike ElfkyuminMvp's BanabestfriendmelodyNo ratings yet
- and Report Fy BSC FonDocument43 pagesand Report Fy BSC FonNainesh soyantarNo ratings yet
- Communication in Nursing ReviewerDocument4 pagesCommunication in Nursing ReviewerHana-Lou TaquiquiNo ratings yet
- Week 12 Module FNP LectureDocument15 pagesWeek 12 Module FNP LectureNichole CabadduNo ratings yet
- Documentation in NursingDocument41 pagesDocumentation in NursingGLAIZA PALATINONo ratings yet
- Lecture FinalsDocument121 pagesLecture FinalsFrance LagundayNo ratings yet
- Recording Training: General ObjectiveDocument8 pagesRecording Training: General ObjectiveFarida ZakzoukNo ratings yet
- Specific Skills: Types of Documentation: 1. RecordingDocument5 pagesSpecific Skills: Types of Documentation: 1. Recordingmsah820No ratings yet
- OBM752 HM Unit-IV NotesDocument34 pagesOBM752 HM Unit-IV NotesRajanNo ratings yet
- DOCUMENTATIONDocument2 pagesDOCUMENTATION황춘히No ratings yet
- Relevance of Nursing Documentation and Its Legal ImplicationsDocument8 pagesRelevance of Nursing Documentation and Its Legal ImplicationsGeorge AyiteyNo ratings yet
- Guidelines-in-effective-documentation (1)Document27 pagesGuidelines-in-effective-documentation (1)Gleza MirallesNo ratings yet
- Submitted By: Khyati ROLL. NO:-1819116 BPT 3 YearDocument51 pagesSubmitted By: Khyati ROLL. NO:-1819116 BPT 3 YearShainaNo ratings yet
- Documenting and ReportingDocument33 pagesDocumenting and ReportingShaquilla TrappNo ratings yet
- Documentation and ReportingDocument4 pagesDocumentation and Reportingsnv rishiNo ratings yet
- Chapter 1 The Accident and ImergencyDocument35 pagesChapter 1 The Accident and ImergencyKusumadewi WidiarsaNo ratings yet
- Chapter One: 1.1 Background InformationDocument73 pagesChapter One: 1.1 Background InformationShaheeda janubhaiNo ratings yet
- Cmca Rle L1 DocumentationDocument23 pagesCmca Rle L1 DocumentationJay EstrellaNo ratings yet
- Chapter One: 1.1 Background InformationDocument73 pagesChapter One: 1.1 Background InformationMarkNo ratings yet
- Evaluation and FHSISDocument6 pagesEvaluation and FHSISShara SampangNo ratings yet
- Hatem - Documentation in Nursing SummaryDocument3 pagesHatem - Documentation in Nursing SummaryHatem FaroukNo ratings yet
- Nursing DiagnosisDocument38 pagesNursing DiagnosisJR Rolf NeuqeletNo ratings yet
- Medical Assistant Duties For ResumeDocument7 pagesMedical Assistant Duties For Resumef5dt39tp100% (2)
- Documenting, Reporting, Conferring, and Using InformaticsDocument92 pagesDocumenting, Reporting, Conferring, and Using InformaticsZhiela Esteban AbivaNo ratings yet
- Nursing RecordsDocument20 pagesNursing Recordstessy mathewNo ratings yet
- Legal Protection of Nursing ServiceDocument4 pagesLegal Protection of Nursing ServiceJanna Kristine Ferrer Yosores80% (5)
- WordsDocument11 pagesWordsAref HoseyniNo ratings yet
- Master FormDocument62 pagesMaster FormsamsulNo ratings yet
- Sarah Fahy CV College PDFDocument4 pagesSarah Fahy CV College PDFapi-487352339No ratings yet
- Labrel 104-195Document1,014 pagesLabrel 104-195Maria Seleena HipolitoNo ratings yet
- "Fish" From Gourmet RhapsodyDocument4 pages"Fish" From Gourmet RhapsodySean MattioNo ratings yet
- Working Length Determination in RCTDocument38 pagesWorking Length Determination in RCTDidar Sadiq Kwekha100% (1)
- Generatuer Rayon X 03Document21 pagesGeneratuer Rayon X 03Mehieddine AslounNo ratings yet
- Brooks MT 3018Document16 pagesBrooks MT 3018Martin AndradeNo ratings yet
- Subway 2009Document12 pagesSubway 2009sparklers_mNo ratings yet
- EXERCISE - (JEE Main) Chemical Equilibrium - CombinedDocument24 pagesEXERCISE - (JEE Main) Chemical Equilibrium - CombinedKeerthana Reddy DomaNo ratings yet
- Personal LetterDocument4 pagesPersonal LetterAskme AzmyNo ratings yet
- Ecosystem Components and InteractionsDocument31 pagesEcosystem Components and InteractionsBirraa TajuNo ratings yet
- Midterm Exam Reviewer: Surgical Handwashing QuizDocument9 pagesMidterm Exam Reviewer: Surgical Handwashing QuizOfficially RandomNo ratings yet
- Broiled Salisbury SteaksDocument29 pagesBroiled Salisbury SteaksCei mendozaNo ratings yet
- Warm Vs Cold ShockDocument8 pagesWarm Vs Cold ShockmarleeramirezNo ratings yet
- FORM HSE MATRIX TRAINING (Contoh)Document1 pageFORM HSE MATRIX TRAINING (Contoh)Hifni GhazaliNo ratings yet
- NanocatalysisDocument9 pagesNanocatalysisNouran ElbadawiNo ratings yet
- Concrete Pump Hose TDSDocument2 pagesConcrete Pump Hose TDSAlaa Abu KhurjNo ratings yet
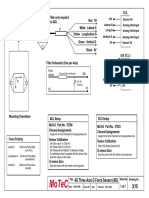
- Filter and wiring schematic for 3-axis ADL G-force sensorDocument1 pageFilter and wiring schematic for 3-axis ADL G-force sensorJuan Ramón Pérez LorenzoNo ratings yet
- Low Noise Pseudomorphic HEMT Technical DataDocument4 pagesLow Noise Pseudomorphic HEMT Technical Datahendpraz88No ratings yet
- Oet Listening 1Document9 pagesOet Listening 1English Around The WorldNo ratings yet
- STD Comparison ChartDocument4 pagesSTD Comparison Chartabu ubaidahNo ratings yet
- Cast Resin Planning Guidelines GEAFOL PDFDocument24 pagesCast Resin Planning Guidelines GEAFOL PDFtenk_man100% (1)
- Edc Power Plant FacilitiesDocument32 pagesEdc Power Plant FacilitiesMichael TayactacNo ratings yet
- Chapter 8Document8 pagesChapter 8Melissa NagyNo ratings yet
- Predicting Natural Hazards PowerPointDocument29 pagesPredicting Natural Hazards PowerPointZarlene SierraNo ratings yet
- Name: Sport: Movement PrepDocument24 pagesName: Sport: Movement PrepS HNo ratings yet