You might also like
- SARS PathophysioDocument2 pagesSARS PathophysioLouise BravoNo ratings yet
- Acute Respiratory Failure Pa Tho PhysiologyDocument4 pagesAcute Respiratory Failure Pa Tho Physiologyroseanne18100% (4)
- Pa ThoDocument3 pagesPa Thotammy_deguzman5223No ratings yet
- Schematic Diagram: Predisposing Factors Precipitating FactorsDocument3 pagesSchematic Diagram: Predisposing Factors Precipitating FactorsDamie FernandezNo ratings yet
- Pathophysiology EmphysemaDocument1 pagePathophysiology Emphysemanursing concept mapsNo ratings yet
- Pharma Finals NotesDocument18 pagesPharma Finals NotesAj MacotoNo ratings yet
- Culture and Sensitivity: InhalationDocument3 pagesCulture and Sensitivity: Inhalationjamie carpioNo ratings yet
- Pcap PathophysiologyDocument3 pagesPcap PathophysiologyZandra Lyn AlundayNo ratings yet
- PathophysiologyDocument1 pagePathophysiologyChua CandiceNo ratings yet
- Patho PneumoniaDocument2 pagesPatho Pneumoniaailyne_galicia100% (2)
- COPD PathophysiologyDocument1 pageCOPD Pathophysiologyaj ajNo ratings yet
- Woc ArdsDocument2 pagesWoc Ardssyarifah salmaNo ratings yet
- Pathophysiology of PcapDocument3 pagesPathophysiology of PcapThomas joshua QuiñonesNo ratings yet
- Respiratory PhysiologyDocument40 pagesRespiratory PhysiologyBookwormNo ratings yet
- Pathophysiology of Chronic Obstructive Pulmonary DisorderDocument2 pagesPathophysiology of Chronic Obstructive Pulmonary DisorderBlessyl Mae EstenzoNo ratings yet
- Community Acquired Pneumonia PathophysiologyDocument2 pagesCommunity Acquired Pneumonia PathophysiologybercoaprilgraceNo ratings yet
- (PULMO) - ABG Interpretation PDFDocument7 pages(PULMO) - ABG Interpretation PDFKeith LajotNo ratings yet
- MK: Ketidakefektifan Bersihanjalanna Pas: - EKG: Sinus Takikardi - X-Ray:pemebesaranparu, DiafragmamendatarDocument2 pagesMK: Ketidakefektifan Bersihanjalanna Pas: - EKG: Sinus Takikardi - X-Ray:pemebesaranparu, DiafragmamendatarpetriNo ratings yet
- Ncma 113Document4 pagesNcma 113Wonie booNo ratings yet
- Respiratory MedicineDocument49 pagesRespiratory MedicinemuhamedNo ratings yet
- L11 Respiratory and Skeletal Systems 2Document41 pagesL11 Respiratory and Skeletal Systems 2rs8kd4kvwhNo ratings yet
- 17 PDFDocument9 pages17 PDFeliasNo ratings yet
- Mod03 GE Pneumonia Class1 Fall2020Document63 pagesMod03 GE Pneumonia Class1 Fall2020RafaelNo ratings yet
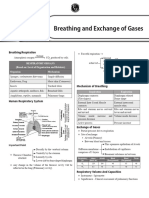
- Breathing and Exchange of GasesDocument6 pagesBreathing and Exchange of Gasesadityaaggarwal821No ratings yet
- Lungs & Gas Exchange Exam Questions: (Total 3 Marks)Document4 pagesLungs & Gas Exchange Exam Questions: (Total 3 Marks)Neelam HanifNo ratings yet
- Student HandoutDocument83 pagesStudent HandoutJoise P, Pharm DNo ratings yet
- Lecture 3 - Breathing Mechanics 2Document36 pagesLecture 3 - Breathing Mechanics 27mb767gqyvNo ratings yet
- Pleural Effusion PatophysiologyDocument2 pagesPleural Effusion PatophysiologyDivine LavaNo ratings yet
- Alumnas Grissel Petra Garcia Paez Materia: Ingles Tecnico HomeworkDocument2 pagesAlumnas Grissel Petra Garcia Paez Materia: Ingles Tecnico HomeworkGrissel PaezNo ratings yet
- Streptococcus Pneumonae: Pathophysiology of CopdDocument1 pageStreptococcus Pneumonae: Pathophysiology of CopdDimpal ChoudharyNo ratings yet
- COPD PathoDocument1 pageCOPD PathoGlenn_Ancheta_2074100% (1)
- Oxygenation - 1Document7 pagesOxygenation - 1Cielo SanchezNo ratings yet
- Draft TB PathophysioDocument2 pagesDraft TB PathophysionikinoonaNo ratings yet
- Pathophysiology Community Aquired Pneumonia and AnemiaDocument3 pagesPathophysiology Community Aquired Pneumonia and Anemiapa3kmedina100% (2)
- 64d0d71d2a4c6c00193d7762 - ## - Breathing and Exchange of Gases Short NotesDocument2 pages64d0d71d2a4c6c00193d7762 - ## - Breathing and Exchange of Gases Short Notesjai maa Durga aadi parashaktiNo ratings yet
- Diffusion of O2 in VesselsDocument1 pageDiffusion of O2 in VesselsAarushi PhilemNo ratings yet
- Assessment Nursing Diagnosis Scientific Rationale Planning Nursing Interventions Rationale EvaluationDocument3 pagesAssessment Nursing Diagnosis Scientific Rationale Planning Nursing Interventions Rationale EvaluationMel Izhra N. MargateNo ratings yet
- Nayli Bio SBP 2019 EseiDocument5 pagesNayli Bio SBP 2019 EseiEqis AlfiesyaNo ratings yet
- Mastering Biology BK1B NotesDocument20 pagesMastering Biology BK1B NotesAlva WongNo ratings yet
- Age - Weather: Aspiration of Secretions Containing MicrobesDocument4 pagesAge - Weather: Aspiration of Secretions Containing Microbeslouie john abilaNo ratings yet
- Assessment Diagnosis Explanation of The Problem Planning Intervention Rationale Evaluation Subjective: Sto: StoDocument5 pagesAssessment Diagnosis Explanation of The Problem Planning Intervention Rationale Evaluation Subjective: Sto: StoMaria Francheska OsiNo ratings yet
- The Pulmonary TableDocument20 pagesThe Pulmonary TableHector100% (1)
- ARDS Patopi FinaleDocument1 pageARDS Patopi FinaleCuttie Anne GalangNo ratings yet
- Texto1 S9 RespiratorioDocument6 pagesTexto1 S9 RespiratorioCAROLINA CHUMACERO BERMEONo ratings yet
- NCP 1 N 2Document5 pagesNCP 1 N 2Cuttie Anne GalangNo ratings yet
- Resp Cheat SheetDocument4 pagesResp Cheat SheetHassaid33No ratings yet
- NCP-Drug Study 2Document4 pagesNCP-Drug Study 2hsiriaNo ratings yet
- Respiratory PhysiologyDocument55 pagesRespiratory PhysiologyANDRES GUARDIA CAYONo ratings yet
- Multiple-Choice QuizDocument7 pagesMultiple-Choice QuizHUAWEI HUAWEINo ratings yet
- Assessment Nursing Diagnosis Scientific Explaination Planning Implementation Rationale EvaluationDocument5 pagesAssessment Nursing Diagnosis Scientific Explaination Planning Implementation Rationale EvaluationDiana MuañaNo ratings yet
- Resp Yamashita Ventilation NotesDocument9 pagesResp Yamashita Ventilation Notes1233211qwerasdNo ratings yet
- Lung Anatomy and Airflow ReportDocument11 pagesLung Anatomy and Airflow Reporttshireletso “TROY” nkunaNo ratings yet
- Respiratory 05 - COPD: Definition: Types For EmphysemaDocument3 pagesRespiratory 05 - COPD: Definition: Types For Emphysemakamil malikNo ratings yet
- 中四至中六 生物科 會員專享試課 - 下載筆記Document15 pages中四至中六 生物科 會員專享試課 - 下載筆記Chang HazelNo ratings yet
- Chapter 43 Physio Respi InsufficiencyDocument3 pagesChapter 43 Physio Respi InsufficiencyAldanna Felicci Garcia CaragNo ratings yet
- Hudson 2012Document10 pagesHudson 2012Rin4lNo ratings yet
- Impaired Gas Exchange RebusquilloDocument2 pagesImpaired Gas Exchange RebusquilloJannen CasasNo ratings yet
- CNS (Primarily) Peripheral Chemoreceptors - Central and Peripheral ChemoreceptorsDocument9 pagesCNS (Primarily) Peripheral Chemoreceptors - Central and Peripheral ChemoreceptorsVin TagenNo ratings yet
- NCP Impaired GasDocument2 pagesNCP Impaired GasRea LynNo ratings yet
- Concrete and Its PropertiesDocument24 pagesConcrete and Its PropertiesAmila LiyanaarachchiNo ratings yet
- Bleeding in A NeonateDocument36 pagesBleeding in A NeonateDrBibek AgarwalNo ratings yet
- Secondary 1 Express English Paper 1 & 2Document15 pagesSecondary 1 Express English Paper 1 & 2Menon HariNo ratings yet
- Consolidation of ClayDocument17 pagesConsolidation of ClayMD Anan MorshedNo ratings yet
- 2-Phase Synchronous-Rectified Buck Controller For Mobile GPU PowerDocument18 pages2-Phase Synchronous-Rectified Buck Controller For Mobile GPU PowerMax Assistência TécnicaNo ratings yet
- Director's Update Our StudentsDocument23 pagesDirector's Update Our StudentsAdrian MojicaNo ratings yet
- November 2013 (v3) QP - Paper 6 CIE Biology IGCSEDocument12 pagesNovember 2013 (v3) QP - Paper 6 CIE Biology IGCSEAfra AhamedNo ratings yet
- Automotive Voltage DropDocument5 pagesAutomotive Voltage Dropashraf.rahim139No ratings yet
- Eye Essentials Cataract Assessment Classification and ManagementDocument245 pagesEye Essentials Cataract Assessment Classification and ManagementKyros1972No ratings yet
- 2.3 & 2.5 Cell DivisionDocument14 pages2.3 & 2.5 Cell DivisionJhonnyNo ratings yet
- Hotel ClassificationDocument10 pagesHotel ClassificationRonelyn Boholst100% (1)
- Reaction Paper On Water PollutionDocument1 pageReaction Paper On Water PollutionAztah KivycNo ratings yet
- Mcdes 1Document7 pagesMcdes 1JerdNo ratings yet
- MPX-200 Service Manual PDFDocument90 pagesMPX-200 Service Manual PDFvivijaNo ratings yet
- Mrunal Handout 12 CSP20Document84 pagesMrunal Handout 12 CSP20SREEKANTHNo ratings yet
- Subhead-5 Pump Motors & Related WorksDocument24 pagesSubhead-5 Pump Motors & Related Worksriyad mahmudNo ratings yet
- MediclaimDocument3 pagesMediclaimPrajwal ShettyNo ratings yet
- Anglo American - Belt Conveyor Design CriteriaDocument19 pagesAnglo American - Belt Conveyor Design CriteriaIgor San Martín Peñaloza0% (1)
- Leon County Sheriff'S Office Daily Booking Report 4-Jan-2022 Page 1 of 3Document3 pagesLeon County Sheriff'S Office Daily Booking Report 4-Jan-2022 Page 1 of 3WCTV Digital TeamNo ratings yet
- Saa6d107e 1CC S N 26540705 Up - Parts Book Do Motor GD655-5Document164 pagesSaa6d107e 1CC S N 26540705 Up - Parts Book Do Motor GD655-5kit101No ratings yet
- Advances in Agronomy v.84Document333 pagesAdvances in Agronomy v.84luisiunesNo ratings yet
- All About Hemp Plant HempInc-eBookDocument17 pagesAll About Hemp Plant HempInc-eBookFelix MartinezNo ratings yet
- Week 4 (Theories)Document15 pagesWeek 4 (Theories)Erica Velasco100% (1)
- Dysfunctional Uterine Bleeding (DUB)Document1 pageDysfunctional Uterine Bleeding (DUB)Bheru LalNo ratings yet
- Mpez-6 Installation Manual - Inline 201007Document8 pagesMpez-6 Installation Manual - Inline 201007api-244989438No ratings yet
- PC110R 1 S N 2265000001 Up PDFDocument330 pagesPC110R 1 S N 2265000001 Up PDFLuis Gustavo Escobar MachadoNo ratings yet
- Design and Fabrication of Floor Cleaning Machine - A ReviewDocument4 pagesDesign and Fabrication of Floor Cleaning Machine - A ReviewIJIERT-International Journal of Innovations in Engineering Research and Technology100% (1)
- Respiratory Examination - Protected 1Document4 pagesRespiratory Examination - Protected 1anirudh811100% (1)
- "Hiv and Aids Awareness of Junior and Senior High School Students" Part I: Profile of RespondentsDocument1 page"Hiv and Aids Awareness of Junior and Senior High School Students" Part I: Profile of RespondentsDahl xxNo ratings yet
- Death Obituary Cause of Death Ookht PDFDocument4 pagesDeath Obituary Cause of Death Ookht PDFMayerRhodes8No ratings yet