You might also like
- Cog 13 - MineralsDocument26 pagesCog 13 - MineralsTahpehs PhiriNo ratings yet
- Disturbances in Mineral MetabolismDocument21 pagesDisturbances in Mineral MetabolismAmit GaurNo ratings yet
- Essential TraceelementsDocument7 pagesEssential TraceelementsSrujana BudheNo ratings yet
- Mineral MetabolismDocument12 pagesMineral MetabolismPavan Kumar RNo ratings yet
- 10.1016@B978 0 323 55512 8.00145 9Document7 pages10.1016@B978 0 323 55512 8.00145 9ahmad aubert pallas bpNo ratings yet
- 6.2 Micronutrients: MineralsDocument3 pages6.2 Micronutrients: Mineralsaayushi tejwaniNo ratings yet
- Minerals: The MicromineralsDocument28 pagesMinerals: The MicromineralsJake Arizapa0% (1)
- CalciumDocument5 pagesCalciumjnssmylpz16No ratings yet
- AAP 2210 Nutrition and Feeding of Non-Ruminants - Last Part 22.11.2019Document33 pagesAAP 2210 Nutrition and Feeding of Non-Ruminants - Last Part 22.11.2019Kevin KahingaNo ratings yet
- Chapter 3 Essential Trace and Nonessential IonDocument8 pagesChapter 3 Essential Trace and Nonessential IonAnthony V. DaquilaNo ratings yet
- Minerals DraftDocument7 pagesMinerals DraftBảo ĐoànNo ratings yet
- The Importance of Minerals in The Health of HumansDocument11 pagesThe Importance of Minerals in The Health of Humanskrich navarroNo ratings yet
- Minerals and Their ClassificationDocument20 pagesMinerals and Their ClassificationShaista AkbarNo ratings yet
- Mineral Metabolism and Abnormalities: Le Duong Hoang Huy M.D Email: Huyldh@pnt - Edu.vnDocument66 pagesMineral Metabolism and Abnormalities: Le Duong Hoang Huy M.D Email: Huyldh@pnt - Edu.vnLam NgoNo ratings yet
- Mineral MetabolismDocument35 pagesMineral MetabolismAditya NayakNo ratings yet
- Small Animal Clinical NutritionDocument42 pagesSmall Animal Clinical NutritionJairo Pereira100% (1)
- Minerial, 2ed Class, BiochemistryDocument29 pagesMinerial, 2ed Class, BiochemistryHussein Al SaediNo ratings yet
- Trace Elements: Sharlyn B. AustriaDocument7 pagesTrace Elements: Sharlyn B. Austriaaida bNo ratings yet
- E013721823 PDFDocument6 pagesE013721823 PDFAbeiasaNo ratings yet
- 458 2020 02 08 MINERALES Diapositivas 2020 Web 1Document15 pages458 2020 02 08 MINERALES Diapositivas 2020 Web 1Juan GonzalezNo ratings yet
- Cations, Anions, and The Human BodyDocument1 pageCations, Anions, and The Human BodyKathryn Dominique PachecoNo ratings yet
- Minerals: Small Ruminant SeriesDocument6 pagesMinerals: Small Ruminant SeriesRaphael yagamiNo ratings yet
- Oleh: Sri Sumarmi: Pelangi GiziDocument55 pagesOleh: Sri Sumarmi: Pelangi GiziRika AmeiliawatiNo ratings yet
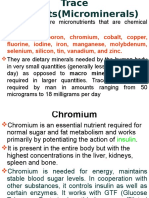
- Trace Elements (Microminerals)Document22 pagesTrace Elements (Microminerals)CLEMENTNo ratings yet
- Minerals: Role of Minerals in The BodyDocument12 pagesMinerals: Role of Minerals in The BodyZA IDNo ratings yet
- MINERALSDocument42 pagesMINERALSVincent Maralit MaterialNo ratings yet
- Mineral Metabolism - P, Fe.Document30 pagesMineral Metabolism - P, Fe.Shivanand MaliNo ratings yet
- C CCCC C: Minerals For LifeDocument35 pagesC CCCC C: Minerals For LifeBench AcostaNo ratings yet
- The Hidden Deficiency Uncovering the Health Impacts of Mineral ShortagesFrom EverandThe Hidden Deficiency Uncovering the Health Impacts of Mineral ShortagesNo ratings yet
- Macro and Micro Minerals-1-1Document36 pagesMacro and Micro Minerals-1-1pinkish7_preciousNo ratings yet
- Presentation On Sodium, Potassium and IronDocument43 pagesPresentation On Sodium, Potassium and IronSangay CheshireNo ratings yet
- Trace Elements in Human BeingsDocument17 pagesTrace Elements in Human BeingsSravan JanardhananNo ratings yet
- MINERALSDocument26 pagesMINERALSSini MinoshNo ratings yet
- Assignment of Food NutritionDocument22 pagesAssignment of Food NutritionHammad EjazNo ratings yet
- Macro and Micro Minerals-1Document38 pagesMacro and Micro Minerals-1Ximay Mato100% (1)
- Essential Trace ElementsDocument21 pagesEssential Trace ElementsPitambar PoudelNo ratings yet
- MACROMINERALSDocument3 pagesMACROMINERALSeaaiedlNo ratings yet
- MineralsDocument9 pagesMineralsAyesha AfzalNo ratings yet
- TRACE MineralsDocument18 pagesTRACE MineralsKipchirchir AbednegoNo ratings yet
- 021220190my Mineral MetabolismDocument29 pages021220190my Mineral Metabolismslmen1269No ratings yet
- Dr. Joel WallachDocument10 pagesDr. Joel WallachfabriciopNo ratings yet
- Dr. Joel WallachDocument10 pagesDr. Joel WallachfabriciopNo ratings yet
- Department of Periodontics and Implantology: Calcium MetabolismDocument63 pagesDepartment of Periodontics and Implantology: Calcium Metabolismrasagna reddy100% (1)
- Mineral MetabolismDocument34 pagesMineral Metabolismalaa haithamNo ratings yet
- 1207 Minerals Elements of Human Nutrition GuideDocument24 pages1207 Minerals Elements of Human Nutrition GuideLETRAP100% (1)
- минералыDocument62 pagesминералыibb ChattawNo ratings yet
- ROLE OF MINERALS IN LIVESTOCK PRODUCTION - Pashudhan PrahareeDocument7 pagesROLE OF MINERALS IN LIVESTOCK PRODUCTION - Pashudhan PrahareeLonely WolfNo ratings yet
- CCN MineralsDocument106 pagesCCN Mineralsariganyira FrancisNo ratings yet
- Role of Iron in Human BodyDocument6 pagesRole of Iron in Human BodyAliza KhanNo ratings yet
- Minerals: Sodium (Salt) Functions in The BodyDocument3 pagesMinerals: Sodium (Salt) Functions in The BodyUca NajjarNo ratings yet
- 1 SMDocument6 pages1 SMAriSuandiNo ratings yet
- Chapter 25 BolandDocument8 pagesChapter 25 BolandEasy ways2017No ratings yet
- Mineral Makro Dan MetabolismeDocument11 pagesMineral Makro Dan MetabolismeNina Yelly100% (1)
- Lecture 8Document34 pagesLecture 8Omar F'KassarNo ratings yet
- PFA NutritionDocument2 pagesPFA NutritionĐẹp Răng KhểnhNo ratings yet
- Electrons Redox Scavenging Free Radicals (1) (2) : CopperDocument9 pagesElectrons Redox Scavenging Free Radicals (1) (2) : CopperTowhid HasanNo ratings yet
- Bioinorganic ChemistryDocument41 pagesBioinorganic ChemistryRamagouda HinglajeNo ratings yet
- Thyroid Gland 1 UMST White BackgroundDocument41 pagesThyroid Gland 1 UMST White Backgroundعوض الكريمNo ratings yet
- 7.MHC and TransplantationDocument34 pages7.MHC and Transplantationعوض الكريمNo ratings yet
- 6.hypersensitivity Reactions 2Document32 pages6.hypersensitivity Reactions 2عوض الكريمNo ratings yet
- Owth and DevelopmentDocument21 pagesOwth and Developmentعوض الكريمNo ratings yet
- 1 ZoonosesDocument13 pages1 Zoonosesعوض الكريمNo ratings yet
- Vitamins: Dr. Babiker Mohamed Ali RahamtallaDocument52 pagesVitamins: Dr. Babiker Mohamed Ali Rahamtallaعوض الكريمNo ratings yet
- Upper Airway Obstruction.1-1Document46 pagesUpper Airway Obstruction.1-1عوض الكريمNo ratings yet
- Benign NephrosclerosisDocument15 pagesBenign Nephrosclerosisعوض الكريمNo ratings yet
- Tubules and Interstitium: Diseases of The KidneyDocument46 pagesTubules and Interstitium: Diseases of The Kidneyعوض الكريمNo ratings yet
- 9.renal TumorsDocument12 pages9.renal Tumorsعوض الكريمNo ratings yet
- TonsillitisDocument30 pagesTonsillitisعوض الكريمNo ratings yet
- ControlDocument12 pagesControlSirVietaNo ratings yet
- ZOO 111 MWF 2:30-3:30 PM: White-Throated Rock Thrush (Monticola Gularis)Document38 pagesZOO 111 MWF 2:30-3:30 PM: White-Throated Rock Thrush (Monticola Gularis)Princess NonNo ratings yet
- Lecture 3 Innate ImmunityDocument26 pagesLecture 3 Innate ImmunitytimcarasNo ratings yet
- 5CRMSDocument2 pages5CRMSpandoraelitesNo ratings yet
- Chapter 1 What Is VisionDocument18 pagesChapter 1 What Is VisionPierre RodulfoNo ratings yet
- Electromyography I PDFDocument13 pagesElectromyography I PDFkeithtrahNo ratings yet
- Drug EduDrug Education and Vice Controlcation and Vice ControlDocument9 pagesDrug EduDrug Education and Vice Controlcation and Vice ControlChristian Dave Tad-awanNo ratings yet
- Aging Changes in The Heart and Blood VesselsDocument4 pagesAging Changes in The Heart and Blood VesselsTotalenesya Reforrent SutiknoNo ratings yet
- Empty Bowl MeditationDocument2 pagesEmpty Bowl MeditationMarifé Cepeda CastroNo ratings yet
- Sorenson Atlas of Human Histology Chapters 1 and 14Document56 pagesSorenson Atlas of Human Histology Chapters 1 and 14Nick john CaminadeNo ratings yet
- Bioreaction Engineering Principles Nielsen Villadsen PDFDocument554 pagesBioreaction Engineering Principles Nielsen Villadsen PDFMuchachos del Rio50% (2)
- Cambios Fisiologicos UlcDocument16 pagesCambios Fisiologicos UlcLuisa Fernanda Laverde ChunzaNo ratings yet
- 1 Sensory MemoryDocument8 pages1 Sensory MemoryViệt Dũng Trần NguyễnNo ratings yet
- Seeley's Chapter 8 Nervous SystemDocument100 pagesSeeley's Chapter 8 Nervous SystemChristine Tapawan88% (8)
- Biological (Met)Document52 pagesBiological (Met)SirLhitz B. UmaliNo ratings yet
- Testicular CancerDocument5 pagesTesticular CancerypintohNo ratings yet
- External Ventricular Drainage PDFDocument2 pagesExternal Ventricular Drainage PDFBarbara100% (1)
- Comparative Phytochemical Profiling of Clerodendrum InfortunatumDocument10 pagesComparative Phytochemical Profiling of Clerodendrum Infortunatumupendra1616No ratings yet
- Pathology+101 Complete)Document147 pagesPathology+101 Complete)Goh Kah Yong100% (2)
- Floating Leaf Disk AssayDocument3 pagesFloating Leaf Disk AssayJohn Osborne0% (1)
- S.5 BIO Reproduction in Animals NOTESDocument18 pagesS.5 BIO Reproduction in Animals NOTESmusokelukia6No ratings yet
- How Cells Harvest Chemical EnergyDocument75 pagesHow Cells Harvest Chemical EnergylinNo ratings yet
- Agriculture& Horticulture Conference BrochureDocument6 pagesAgriculture& Horticulture Conference BrochureAgriculture conferenceNo ratings yet
- Neonatal PneumoniaDocument2 pagesNeonatal PneumoniaJustin EduardoNo ratings yet
- Facial Nerve MCQDocument4 pagesFacial Nerve MCQIqbal Syed100% (1)
- Types of Burns ArticleDocument7 pagesTypes of Burns ArticleSeltri 'ceti' SeptianiNo ratings yet
- Essential Amino Acids Functions: Patricia Anne Nicole C. Mansat Bs Nursing BiochemDocument4 pagesEssential Amino Acids Functions: Patricia Anne Nicole C. Mansat Bs Nursing BiochembiologyNo ratings yet
- Extroverts (Also Spelled Extraverts: ExtroversionDocument8 pagesExtroverts (Also Spelled Extraverts: Extroversionrams4u_001No ratings yet