You might also like
- Paper 1 Calvin and Hobbes Essay - Sarah Al ObaidanDocument3 pagesPaper 1 Calvin and Hobbes Essay - Sarah Al ObaidanSarah Al ObaidanNo ratings yet
- Monologue Pirmojo Poros Kandidato VilniusDocument2 pagesMonologue Pirmojo Poros Kandidato VilniusGintarė ŽindulienėNo ratings yet
- Neuropsychological Rehabilitation of Executive Functions: Challenges and PerspectivesDocument6 pagesNeuropsychological Rehabilitation of Executive Functions: Challenges and PerspectivesEduardo jose LegalNo ratings yet
- Non Pharmacological Cognitive Enhancers 2015Document6 pagesNon Pharmacological Cognitive Enhancers 2015NungkiNo ratings yet
- A Pilot Study To Evaluate Multi-Dimensional Effects of Dance For People With Parkinson's DiseaseDocument6 pagesA Pilot Study To Evaluate Multi-Dimensional Effects of Dance For People With Parkinson's DiseaseRudolfGerNo ratings yet
- LSVT BigDocument13 pagesLSVT BigAgatha SharmaNo ratings yet
- Journal of Yoga & Physical TherapyDocument7 pagesJournal of Yoga & Physical Therapykhadesakshi55No ratings yet
- Physical Activity For Cognitive and Mental Health in Youth: A Systematic Review of MechanismsDocument15 pagesPhysical Activity For Cognitive and Mental Health in Youth: A Systematic Review of MechanismsKiki SyamNo ratings yet
- Jurnal Pendukung 2 - Yoga Therapy For Social Cognition in Schizophrenia - An Experimental Medicine-Based Randomized Controlled TrialDocument8 pagesJurnal Pendukung 2 - Yoga Therapy For Social Cognition in Schizophrenia - An Experimental Medicine-Based Randomized Controlled TrialM SNo ratings yet
- Psychophysiological Effects of Dance MovementDocument11 pagesPsychophysiological Effects of Dance MovementDrHellenNo ratings yet
- Neurobic Excersise Impact On Cognative FunctionDocument8 pagesNeurobic Excersise Impact On Cognative FunctionZalinah Mohd YusofNo ratings yet
- 10 11648 J Ajap 20180701 11 PDFDocument10 pages10 11648 J Ajap 20180701 11 PDFIsaac Saucedo FloresNo ratings yet
- 21 Engh2015Document12 pages21 Engh2015Sergio Machado NeurocientistaNo ratings yet
- Mindfulness Intervention For Mild Cognitive Impairment Led To Attention Related Improvements and Neuroplastic Changes Results From A 9 Month Randomized Control Trial Junhong Yu Full ChapterDocument32 pagesMindfulness Intervention For Mild Cognitive Impairment Led To Attention Related Improvements and Neuroplastic Changes Results From A 9 Month Randomized Control Trial Junhong Yu Full Chapterlydia.dupuy181100% (17)
- 90 10.5923.j.ijpbs.20170704.04Document12 pages90 10.5923.j.ijpbs.20170704.04Sanja Tatalovic VorkapicNo ratings yet
- Mindfulness MeditationDocument8 pagesMindfulness Meditationdyg dygNo ratings yet
- Article Jurnal Risenologi Linteratur Review Antonius NgadiranDocument6 pagesArticle Jurnal Risenologi Linteratur Review Antonius NgadiranFuad AfdhalNo ratings yet
- Jurnallkepjiwa PDFDocument20 pagesJurnallkepjiwa PDFDewi AgustianiNo ratings yet
- Physical Activity, Exercise, and Mental DisordersDocument8 pagesPhysical Activity, Exercise, and Mental DisordersHargo PsyNo ratings yet
- Psychogeriatrics - 2013 - Teixeira - Effects of Square Stepping Exercise On Cognitive Functions of Older PeopleDocument9 pagesPsychogeriatrics - 2013 - Teixeira - Effects of Square Stepping Exercise On Cognitive Functions of Older PeopleAkbar MaulabiNo ratings yet
- Effects of Exercise Programs On Anxiety in Individuals With Disabilities: A Systematic Review With A Meta-AnalysisDocument12 pagesEffects of Exercise Programs On Anxiety in Individuals With Disabilities: A Systematic Review With A Meta-AnalysisAndrade GuiNo ratings yet
- The e Ect of Active Video Games On Cognitive Functioning in Clinical and Non-Clinical Populations A Meta-Analysis of Randomized Controlled TrialsDocument10 pagesThe e Ect of Active Video Games On Cognitive Functioning in Clinical and Non-Clinical Populations A Meta-Analysis of Randomized Controlled TrialsFaiz KunNo ratings yet
- The Effects of Resistance Training On Well-Being and Memory in Elderly VolunteersDocument8 pagesThe Effects of Resistance Training On Well-Being and Memory in Elderly VolunteersAdaLydiaRodriguezNo ratings yet
- Fragi 02 636390Document11 pagesFragi 02 636390msNo ratings yet
- Effects of Cognitive Remediation On Cognitive and SocialDocument14 pagesEffects of Cognitive Remediation On Cognitive and SocialHarumy NakayamaNo ratings yet
- Zoom - Jurnal Psikotik - Nita Fitriani W.Document9 pagesZoom - Jurnal Psikotik - Nita Fitriani W.mayNo ratings yet
- Yoga and CognitionDocument6 pagesYoga and Cognition19satishkumar49No ratings yet
- 6 - Takahashi2012Document6 pages6 - Takahashi2012Sergio Machado NeurocientistaNo ratings yet
- MindfulnessDocument14 pagesMindfulnessAnthony FelderNo ratings yet
- 2022 (A) - The Effect of Change in PA Behaviour On DS Among European Older Adults (Human Movement) PDFDocument7 pages2022 (A) - The Effect of Change in PA Behaviour On DS Among European Older Adults (Human Movement) PDFPriscila PintoNo ratings yet
- Functioning in Schizophrenia: A Delphi Study Covering The Perspective of PhysiotherapistsDocument9 pagesFunctioning in Schizophrenia: A Delphi Study Covering The Perspective of Physiotherapistsyalocim666No ratings yet
- Vancampfort - State Anxiety, Psychological Stress and Positive Well-Being Responses To Yoga and Aerobic Exercise in People With Schizophrenia A Pilot Study.48Document7 pagesVancampfort - State Anxiety, Psychological Stress and Positive Well-Being Responses To Yoga and Aerobic Exercise in People With Schizophrenia A Pilot Study.48Beto RebolledoNo ratings yet
- Long-Term Effects of Cognitive Rehabilitation On Brain, Functional Outcome and Cognition in Parkinson's DiseaseDocument8 pagesLong-Term Effects of Cognitive Rehabilitation On Brain, Functional Outcome and Cognition in Parkinson's DiseasesahandNo ratings yet
- Imbimbo, 2021Document7 pagesImbimbo, 2021Ailla MariaNo ratings yet
- 1 s2.0 S1836955319301341 Main PDFDocument10 pages1 s2.0 S1836955319301341 Main PDFAdilson Skalski ZabielaNo ratings yet
- Landsman Dijkstra2006Document14 pagesLandsman Dijkstra2006Hegymegi-Kiss DalmaNo ratings yet
- Bagian Ilmu Kedokteran Fakultas Kedokteran Ukrida Jakarta: DR Pembimbing: DR Agung SPKJDocument17 pagesBagian Ilmu Kedokteran Fakultas Kedokteran Ukrida Jakarta: DR Pembimbing: DR Agung SPKJlevineloveNo ratings yet
- Jad 88 Jad220243Document16 pagesJad 88 Jad220243MARIA JULIANA GONZALEZNo ratings yet
- Jurnal InternasionalDocument7 pagesJurnal Internasional34. Putu Mariska Abdi CahyaniNo ratings yet
- 2017 Article 457Document10 pages2017 Article 457JoeNo ratings yet
- Review Article Potential Benefits of Physical Activity in MCI and DementiaDocument10 pagesReview Article Potential Benefits of Physical Activity in MCI and DementiaCláudia SilvaNo ratings yet
- Miyajima Et Al. - 2016 - The Effects of Cognitive Remediation Therapy Using - Unlocked PDFDocument27 pagesMiyajima Et Al. - 2016 - The Effects of Cognitive Remediation Therapy Using - Unlocked PDFJeune WillNo ratings yet
- Floriano, 2015Document8 pagesFloriano, 2015Ailla MariaNo ratings yet
- Exercise Physiology Research PaperDocument7 pagesExercise Physiology Research Paperapi-734755901No ratings yet
- UrnalfisioterapiDocument9 pagesUrnalfisioterapiEko MaryaniNo ratings yet
- Brain and Cognition: Rinske A. Gotink, Rozanna Meijboom, Meike W. Vernooij, Marion Smits, M.G. Myriam HuninkDocument10 pagesBrain and Cognition: Rinske A. Gotink, Rozanna Meijboom, Meike W. Vernooij, Marion Smits, M.G. Myriam HuninkcristinaNo ratings yet
- Yoga e CogniçãoDocument6 pagesYoga e CogniçãoMessias FilhoNo ratings yet
- Does Exercise Make You SmarterDocument9 pagesDoes Exercise Make You Smarterfnf102030No ratings yet
- Nandha Kumara PujamDocument6 pagesNandha Kumara PujamnandhaNo ratings yet
- Artigo - Depressão e Treinamento de ForçaDocument11 pagesArtigo - Depressão e Treinamento de ForçaRicardo CortinoveNo ratings yet
- Cognitive Interventions in Mature and Older Adults, Benefits For Psychological Well-Being and Quality of LifeDocument12 pagesCognitive Interventions in Mature and Older Adults, Benefits For Psychological Well-Being and Quality of LifeGabrielle PradoNo ratings yet
- Blomstrand 2020Document13 pagesBlomstrand 2020SAMADHI FERNANDO SALGUERO SILESNo ratings yet
- Consciousness and Cognition: Fadel Zeidan, Susan K. Johnson, Bruce J. Diamond, Zhanna David, Paula GoolkasianDocument9 pagesConsciousness and Cognition: Fadel Zeidan, Susan K. Johnson, Bruce J. Diamond, Zhanna David, Paula GoolkasianVictoria MunteanNo ratings yet
- JURNAL PENGABMAS SENAM OTAK LANSIA (INDRIANA E.Y) .Id - enDocument4 pagesJURNAL PENGABMAS SENAM OTAK LANSIA (INDRIANA E.Y) .Id - enFeldi AsgelNo ratings yet
- Studyprotocol Open AccessDocument13 pagesStudyprotocol Open AccessGabrielDosAnjosNo ratings yet
- Versão Final Depressão ExecutivasDocument15 pagesVersão Final Depressão ExecutivasGeorgiana PrisoschiNo ratings yet
- Goodwin Et Al-2008-Movement DisordersDocument10 pagesGoodwin Et Al-2008-Movement DisordersyuliatinnisaNo ratings yet
- Ni Hms 902678Document17 pagesNi Hms 902678suanton5885No ratings yet
- The Brain and Movement - How Physical Activity Affects The BrainDocument6 pagesThe Brain and Movement - How Physical Activity Affects The BrainSơn Đoàn TrungNo ratings yet
- Research. 244, 394-402Document6 pagesResearch. 244, 394-402annespeaks017No ratings yet
- Development and Analysis of Group Intervention in Occupational Therapy For Elderly With Mild Neurocognitive DisorderDocument20 pagesDevelopment and Analysis of Group Intervention in Occupational Therapy For Elderly With Mild Neurocognitive DisorderFrancisca Cid BelmarNo ratings yet
- Psychophysiological assessment of human cognition and its enhancement by a non-invasive methodFrom EverandPsychophysiological assessment of human cognition and its enhancement by a non-invasive methodNo ratings yet
- Overview of Cardiac Valvular Disorders - Cardiovascular Disorders - MSD Manual Professional EditionDocument4 pagesOverview of Cardiac Valvular Disorders - Cardiovascular Disorders - MSD Manual Professional EditionNura Eky VNo ratings yet
- 3 Mode Exc OADocument7 pages3 Mode Exc OANura Eky VNo ratings yet
- S0003999321002963Document10 pagesS0003999321002963Nura Eky VNo ratings yet
- Bloom's Taxonomy - WikipediaDocument11 pagesBloom's Taxonomy - WikipediaNura Eky VNo ratings yet
- OTAGO On FrailtyDocument5 pagesOTAGO On FrailtyNura Eky VNo ratings yet
- 1 s2.0 S0531556520305611 MainDocument8 pages1 s2.0 S0531556520305611 MainNura Eky VNo ratings yet
- 1 s2.0 S1877065719301794 MainDocument8 pages1 s2.0 S1877065719301794 MainNura Eky VNo ratings yet
- Hof Condition For Dynamic StabilityDocument8 pagesHof Condition For Dynamic StabilityNura Eky VNo ratings yet
- Anterior Cruciate Ligament Injury-Who Succeeds WitDocument9 pagesAnterior Cruciate Ligament Injury-Who Succeeds WitNura Eky VNo ratings yet
- CP Spastic, Diskinetik, AtaxicDocument4 pagesCP Spastic, Diskinetik, AtaxicNura Eky VNo ratings yet
- Leonard, 2002Document18 pagesLeonard, 2002Nura Eky VNo ratings yet
- 1 s2.0 S0003999321001404Document10 pages1 s2.0 S0003999321001404Nura Eky VNo ratings yet
- Design CPMDocument5 pagesDesign CPMNura Eky VNo ratings yet
- CASP RCT Checklist PDF Fillable FormDocument4 pagesCASP RCT Checklist PDF Fillable FormNura Eky VNo ratings yet
- Polifarmasi and Fall in ElderlyDocument5 pagesPolifarmasi and Fall in ElderlyNura Eky VNo ratings yet
- Obesity Review MelaninDocument12 pagesObesity Review MelaninNura Eky VNo ratings yet
- Impact of Covid Patient RecoveryDocument15 pagesImpact of Covid Patient RecoveryNura Eky VNo ratings yet
- Pai Patton97PostPrintDocument7 pagesPai Patton97PostPrintNura Eky VNo ratings yet
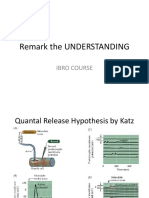
- Remark The UNDERSTANDING: Ibro CourseDocument4 pagesRemark The UNDERSTANDING: Ibro CourseNura Eky VNo ratings yet
- Spleen: - Site of Lymphocyte Proliferation - Immune Surveillance and Response - Cleanses The BloodDocument13 pagesSpleen: - Site of Lymphocyte Proliferation - Immune Surveillance and Response - Cleanses The BloodNura Eky VNo ratings yet
- Midea Modularni Cilleri MGB-service ManualDocument119 pagesMidea Modularni Cilleri MGB-service ManualGermánCastiglioniNo ratings yet
- MBEH'S - Final - Work (1) 27Document72 pagesMBEH'S - Final - Work (1) 27Fon Palverd Brent BridenNo ratings yet
- CH 5 RCC SlabDocument76 pagesCH 5 RCC SlabAmanGargNo ratings yet
- BS 6724 1997Document42 pagesBS 6724 1997Simon Law100% (1)
- Naruto - Harem of The Strong CYOA v1.0 (By Arandommark)Document56 pagesNaruto - Harem of The Strong CYOA v1.0 (By Arandommark)Diogo GalvaoNo ratings yet
- Pre - Historic ArchitectureDocument4 pagesPre - Historic ArchitecturemoodyNo ratings yet
- Handover Analysis of 3G NetworkDocument43 pagesHandover Analysis of 3G NetworkMohammed NazimNo ratings yet
- English Language: 8700/1 Paper 1 Explorations in Creative Reading and Writing Mark SchemeDocument21 pagesEnglish Language: 8700/1 Paper 1 Explorations in Creative Reading and Writing Mark SchemeT SolomonNo ratings yet
- Case Study - XYZ CompanyDocument2 pagesCase Study - XYZ Companysnjingco8505valNo ratings yet
- Ai Lect3 Search2Document135 pagesAi Lect3 Search2Menna SaedNo ratings yet
- 100-149 Bac 2010-2019Document169 pages100-149 Bac 2010-2019Maria RusschihNo ratings yet
- Operator DescriptionDocument6 pagesOperator DescriptionSmart CrazyNo ratings yet
- Group 2 - Article Review (Ads 607)Document12 pagesGroup 2 - Article Review (Ads 607)NUR AHLAM FAIQAH MOHD ROSDINo ratings yet
- Ic Talks Rubric PDFDocument1 pageIc Talks Rubric PDFfrank100% (1)
- Transformers The Basics On The Decepticon Justice Division - YoutubeDocument1 pageTransformers The Basics On The Decepticon Justice Division - YoutubeCarlos BaroniNo ratings yet
- The Science of Emotional Intelligence Book 2021Document226 pagesThe Science of Emotional Intelligence Book 2021raneem.elrahimNo ratings yet
- 12em ComputerDocument17 pages12em ComputerAshish100% (2)
- The Kushite World: Beiträge Zur Sudanforschung. Beiheft 9Document16 pagesThe Kushite World: Beiträge Zur Sudanforschung. Beiheft 9Tarek Mohamed Tarek FouadNo ratings yet
- Surface Vehicle Recommended Practice: (R) Biaxial Wheel Fatigue TestDocument23 pagesSurface Vehicle Recommended Practice: (R) Biaxial Wheel Fatigue TestAdriana SukmanaputraNo ratings yet
- SHE List DocumentDocument1 pageSHE List DocumentMunajamNo ratings yet
- Assignment 1Document2 pagesAssignment 1Nitish KumarNo ratings yet
- Chapter3GettingToKnowYourself Report PE Final ReportDocument16 pagesChapter3GettingToKnowYourself Report PE Final ReportLlabado Sarmiento EleorephNo ratings yet
- Heterogeneous Catalysis: Rica Rose L. SantosDocument10 pagesHeterogeneous Catalysis: Rica Rose L. SantosBenedick Jayson Marti100% (1)
- Rowbottom Cardinals and Jonsson Cardinals Are Almost The Same - E. M. KleinbergDocument6 pagesRowbottom Cardinals and Jonsson Cardinals Are Almost The Same - E. M. KleinbergGabriel medinaNo ratings yet
- Design and Construction LandscapingDocument162 pagesDesign and Construction LandscapingShah Tulsi100% (3)
- DLL - Mathematics 6 - Q3 - W7Document12 pagesDLL - Mathematics 6 - Q3 - W7Gerome JutajeroNo ratings yet
- Rulebook Newton PDFDocument16 pagesRulebook Newton PDFvaggos1988No ratings yet
- PR2 Questionnaire FinalDocument4 pagesPR2 Questionnaire FinalGevin DuetchNo ratings yet