You might also like
- Engineering Journal The Effects of Individualized Physical Rehabilitation ProgramDocument7 pagesEngineering Journal The Effects of Individualized Physical Rehabilitation ProgramEngineering JournalNo ratings yet
- Ejercicio IntervalosDocument7 pagesEjercicio IntervalosOmar DVNo ratings yet
- Pending 1666841661 DownloadDocument8 pagesPending 1666841661 Downloadmilena martinsNo ratings yet
- Comparison Between Single-Diode Low-Level Laser Therapy LLLT and LED Multi-Diode CLUSTER Therapy LEDT Applications Before High-Intensity Exercise PDFDocument9 pagesComparison Between Single-Diode Low-Level Laser Therapy LLLT and LED Multi-Diode CLUSTER Therapy LEDT Applications Before High-Intensity Exercise PDFJanaina PanizzaNo ratings yet
- Dosagem Otima Musculo PDFDocument10 pagesDosagem Otima Musculo PDFJanaina PanizzaNo ratings yet
- Koh2010 PDFDocument12 pagesKoh2010 PDFNovara Qus'nul LuvfiantiNo ratings yet
- 1. CPETDocument16 pages1. CPETFaizal AblansahNo ratings yet
- 10 1111@sms 13853Document17 pages10 1111@sms 13853Cintia BeatrizNo ratings yet
- Intra Dial y TicDocument8 pagesIntra Dial y Ticratna220693No ratings yet
- JURNAL 18 GordonDocument17 pagesJURNAL 18 GordonResky Ika Sah PutriNo ratings yet
- The Effects of Pilates Exercise On Cardiopulmonary Function in The Chronic Stroke Patients A Randomized Controlled Trials PDFDocument5 pagesThe Effects of Pilates Exercise On Cardiopulmonary Function in The Chronic Stroke Patients A Randomized Controlled Trials PDFImam santosoNo ratings yet
- Presentation 1Document31 pagesPresentation 1hababneh790No ratings yet
- A Post Hoc Analysis On Rhythm and High Intensity Interval Training in Cardiac Resynchronization TherapyDocument10 pagesA Post Hoc Analysis On Rhythm and High Intensity Interval Training in Cardiac Resynchronization TherapyNinaRomorNo ratings yet
- Heart Rate As A Measure of Exercise Testing Early After Acquired Brain InjuryDocument5 pagesHeart Rate As A Measure of Exercise Testing Early After Acquired Brain InjuryJaviera Soto AndradeNo ratings yet
- Nightingale 2018Document10 pagesNightingale 2018Ayu SuprabawatiNo ratings yet
- 1 s2.0 S2405587515300263 MainDocument8 pages1 s2.0 S2405587515300263 MainmaracioNo ratings yet
- Jurnal 2 PDFDocument4 pagesJurnal 2 PDFfister19 rifaudinNo ratings yet
- Comparison of Single-Session Dose Response Effects of Whole Body Vibration on Spasticity and Walking Speed in Persons with Spinal Cord InjuryDocument13 pagesComparison of Single-Session Dose Response Effects of Whole Body Vibration on Spasticity and Walking Speed in Persons with Spinal Cord InjurylabsoneducationNo ratings yet
- Accepted Manuscript: 10.1016/j.apmr.2016.08.481Document14 pagesAccepted Manuscript: 10.1016/j.apmr.2016.08.481Vivin YulvinaNo ratings yet
- The Impact of Whole Body Vibration Therapy on Spasticity and Disability of the Patients with Poststroke HemiplegiaDocument6 pagesThe Impact of Whole Body Vibration Therapy on Spasticity and Disability of the Patients with Poststroke HemiplegialabsoneducationNo ratings yet
- Jurnal NataDocument9 pagesJurnal Natadr. siti alfiana RS PELNINo ratings yet
- Thematic Poster Bioenergetics and Training: (No Relationships Reported)Document2 pagesThematic Poster Bioenergetics and Training: (No Relationships Reported)pantufoNo ratings yet
- Letter To The Editor Hydrotherapy in Heart Failure: A Case: BackgroundDocument4 pagesLetter To The Editor Hydrotherapy in Heart Failure: A Case: BackgroundElizabete MonteiroNo ratings yet
- 1 s2.0 S2405587515300263 MainDocument8 pages1 s2.0 S2405587515300263 Maindianaerlita97No ratings yet
- Abstract BookDocument222 pagesAbstract BookArkesh PatnaikNo ratings yet
- The Effect of Physical Training in Chronic Heart FailureDocument5 pagesThe Effect of Physical Training in Chronic Heart FailureDitaris GINo ratings yet
- (European Heart Journal 2004) Beneficial Effects of Chronic Low-FrequencyDocument8 pages(European Heart Journal 2004) Beneficial Effects of Chronic Low-FrequencyRodolfo MatosNo ratings yet
- ARTICLE-Effects of A Wheelchair Ergometer Training Programme On SpinalDocument6 pagesARTICLE-Effects of A Wheelchair Ergometer Training Programme On SpinalavalosheNo ratings yet
- Ventrículo Esquerdo Mecânica, Cardíaca Autonômica e MetabólicaDocument31 pagesVentrículo Esquerdo Mecânica, Cardíaca Autonômica e MetabólicaThiago SartiNo ratings yet
- HRV Powerlift JSSC 2011Document7 pagesHRV Powerlift JSSC 2011Claudio FerranteNo ratings yet
- WJC 3 248Document8 pagesWJC 3 248RIAN NUGRAHANo ratings yet
- CRP2020 1236968Document9 pagesCRP2020 1236968Lal NandaniNo ratings yet
- Cardiac Rehab Improves Physical Capacity and Anxiety After AF AblationDocument10 pagesCardiac Rehab Improves Physical Capacity and Anxiety After AF AblationdrewantaNo ratings yet
- Alterations in Gait Velocity and Grip Strength of Stroke Survivors Following A 12-Week Structured Therapeutic Exercise ProgrammeDocument5 pagesAlterations in Gait Velocity and Grip Strength of Stroke Survivors Following A 12-Week Structured Therapeutic Exercise ProgrammeCristina MuyargasNo ratings yet
- Effects of Respiratory Resistance Training With A Concurrent Flow Device On Wheelchair AthletesDocument8 pagesEffects of Respiratory Resistance Training With A Concurrent Flow Device On Wheelchair AthletesN onlyNo ratings yet
- Prospective Echocardiographic Assessment of Androgenic-Anabolic Steroids Effects On Cardiac Structure and Function in Strength Athletes.Document8 pagesProspective Echocardiographic Assessment of Androgenic-Anabolic Steroids Effects On Cardiac Structure and Function in Strength Athletes.Waleed El-HawarryNo ratings yet
- s-0042-104197Document8 pagess-0042-104197Leticia N. S. NevesNo ratings yet
- Fonseca Et Al - 2017Document23 pagesFonseca Et Al - 2017TAINAH DE PAULANo ratings yet
- Physiotherapy 3 1 2Document4 pagesPhysiotherapy 3 1 2AjiNo ratings yet
- Effects of aerobic exercise using cycle ergometry on balance and functional capacity in post stroke patients a systematic review and meta analysisDocument8 pagesEffects of aerobic exercise using cycle ergometry on balance and functional capacity in post stroke patients a systematic review and meta analysisluigi.adacampoNo ratings yet
- Ijerph 16 03509Document11 pagesIjerph 16 03509Chloe BujuoirNo ratings yet
- Aluko2013 2Document11 pagesAluko2013 2Dr Ahmed NabilNo ratings yet
- Simple Bodyweight Training Improves Cardiorespiratory Fitness With Minimal Time Commitment: A Contemporary Application of The 5BX ApproachDocument8 pagesSimple Bodyweight Training Improves Cardiorespiratory Fitness With Minimal Time Commitment: A Contemporary Application of The 5BX ApproachROBERTANo ratings yet
- Task Oriented Improves Strength - Stroke PatientsDocument7 pagesTask Oriented Improves Strength - Stroke PatientsPedro FonsecaNo ratings yet
- Ergometer Cycling Improves The Ambulatory Function and Cardiovascular Fitness of Stroke Patients-A Randomized Controlled TrialDocument6 pagesErgometer Cycling Improves The Ambulatory Function and Cardiovascular Fitness of Stroke Patients-A Randomized Controlled Trialayu lestariNo ratings yet
- CortezDocument8 pagesCorteztalleresccorporal5No ratings yet
- Core Muscle StrengtheningDocument56 pagesCore Muscle StrengtheningVijayalaxmi KathareNo ratings yet
- 04 - Cardiometabolic Effects of High-Intensity Hybrid Functional Electrical Stimulation Exercise after Spinal Cord InjuryDocument20 pages04 - Cardiometabolic Effects of High-Intensity Hybrid Functional Electrical Stimulation Exercise after Spinal Cord Injurywellington contieroNo ratings yet
- Effect of Whole-Body Vibration On Sagittal Plane in ACLRDocument8 pagesEffect of Whole-Body Vibration On Sagittal Plane in ACLRhasma azisNo ratings yet
- Concurrent Training For Sports Performance - The 2 Sides of The MedalDocument8 pagesConcurrent Training For Sports Performance - The 2 Sides of The MedalDouglas MarinNo ratings yet
- DONEDocument7 pagesDONEpashaNo ratings yet
- Relationship Between The Lower Quarter Y-Balance Test Scores and Isokinetic Strength Testing in Patients Status Post Acl ReconstructionDocument8 pagesRelationship Between The Lower Quarter Y-Balance Test Scores and Isokinetic Strength Testing in Patients Status Post Acl ReconstructionNovfran Adi ArtaNo ratings yet
- 218-1670416528Document7 pages218-1670416528Esteban AmayaNo ratings yet
- Diferent Exercise TrainingDocument9 pagesDiferent Exercise TrainingRenan Carraro RosaNo ratings yet
- Identifying Athlete Body Fluid Changes During A Competitive Season With Bioelectrical Impedance Vector AnalysisDocument7 pagesIdentifying Athlete Body Fluid Changes During A Competitive Season With Bioelectrical Impedance Vector AnalysisLevyNo ratings yet
- Effects of The Bad Ragaz Ring Method On Muscle Activation of The Lower Limbs and Balance Ability in Chronic Stroke: A Randomised Controlled TrialDocument7 pagesEffects of The Bad Ragaz Ring Method On Muscle Activation of The Lower Limbs and Balance Ability in Chronic Stroke: A Randomised Controlled TrialDianaNo ratings yet
- Pilates RandomizadoDocument13 pagesPilates RandomizadorodrigueuresNo ratings yet
- Impact of Aerobic Exercise On Physical Fitness and Fatigue in Children With Acute Lymphoblastic Leukemia PDFDocument8 pagesImpact of Aerobic Exercise On Physical Fitness and Fatigue in Children With Acute Lymphoblastic Leukemia PDFALvin DeeNo ratings yet
- Use of Cold-Water Immersion To Reduce Muscle Damage and Delayed-Onset Muscle Soreness and Preserve Muscle Power in Jiu-Jitsu AthletesDocument10 pagesUse of Cold-Water Immersion To Reduce Muscle Damage and Delayed-Onset Muscle Soreness and Preserve Muscle Power in Jiu-Jitsu Athletes11BULAN FEBRI PUTRI ARISTIAWATINo ratings yet
- Muscle and Exercise PhysiologyFrom EverandMuscle and Exercise PhysiologyJerzy A. ZoladzRating: 3.5 out of 5 stars3.5/5 (3)
- Overview of Cardiac Valvular Disorders - Cardiovascular Disorders - MSD Manual Professional EditionDocument4 pagesOverview of Cardiac Valvular Disorders - Cardiovascular Disorders - MSD Manual Professional EditionNura Eky VNo ratings yet
- Orthography Development: Frank SeifartDocument26 pagesOrthography Development: Frank SeifartAnwar WafiNo ratings yet
- Bloom's Taxonomy - WikipediaDocument11 pagesBloom's Taxonomy - WikipediaNura Eky VNo ratings yet
- 1 s2.0 S0531556520305611 MainDocument8 pages1 s2.0 S0531556520305611 MainNura Eky VNo ratings yet
- 3 Mode Exc OADocument7 pages3 Mode Exc OANura Eky VNo ratings yet
- 1 s2.0 S0003999321001404Document10 pages1 s2.0 S0003999321001404Nura Eky VNo ratings yet
- ESWT in Chronic LBPDocument6 pagesESWT in Chronic LBPNura Eky VNo ratings yet
- ISMST GuidelinesDocument112 pagesISMST GuidelinesDhrubo TaraNo ratings yet
- PRM 5 20200018Document9 pagesPRM 5 20200018Nura Eky VNo ratings yet
- OTAGO On FrailtyDocument5 pagesOTAGO On FrailtyNura Eky VNo ratings yet
- CP Spastic, Diskinetik, AtaxicDocument4 pagesCP Spastic, Diskinetik, AtaxicNura Eky VNo ratings yet
- Cryptogenic Stroke After Percutaneous Closure of ADocument6 pagesCryptogenic Stroke After Percutaneous Closure of ANura Eky VNo ratings yet
- Relationship Between Frontal Knee Position and TheDocument12 pagesRelationship Between Frontal Knee Position and TheNura Eky VNo ratings yet
- Effect of Different Types of Exercises On Psychological and Cognitive Features in People With Parkinson's Disease: A Randomized Controlled TrialDocument10 pagesEffect of Different Types of Exercises On Psychological and Cognitive Features in People With Parkinson's Disease: A Randomized Controlled TrialNura Eky VNo ratings yet
- Spa Therapy and Exercise for Knee OsteoarthritisDocument8 pagesSpa Therapy and Exercise for Knee OsteoarthritisNura Eky VNo ratings yet
- Maintaining Dynamic BalanceDocument8 pagesMaintaining Dynamic BalanceNura Eky VNo ratings yet
- Anterior Cruciate Ligament Injury-Who Succeeds WitDocument9 pagesAnterior Cruciate Ligament Injury-Who Succeeds WitNura Eky VNo ratings yet
- Short Physical Performance Battery Protocol and Score Sheet: 1. Balance TestsDocument8 pagesShort Physical Performance Battery Protocol and Score Sheet: 1. Balance Testsruth lopezNo ratings yet
- CASP RCT Checklist PDF Fillable FormDocument4 pagesCASP RCT Checklist PDF Fillable FormNura Eky VNo ratings yet
- Polifarmasi and Fall in ElderlyDocument5 pagesPolifarmasi and Fall in ElderlyNura Eky VNo ratings yet
- Leonard, 2002Document18 pagesLeonard, 2002Nura Eky VNo ratings yet
- Methods For Assessing Leg Length DiscrepancyDocument13 pagesMethods For Assessing Leg Length DiscrepancyKanika SinhaNo ratings yet
- Pai Patton97PostPrintDocument7 pagesPai Patton97PostPrintNura Eky VNo ratings yet
- Design CPMDocument5 pagesDesign CPMNura Eky VNo ratings yet
- Impact of Covid Patient RecoveryDocument15 pagesImpact of Covid Patient RecoveryNura Eky VNo ratings yet
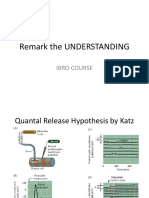
- Remark The UNDERSTANDING: Ibro CourseDocument4 pagesRemark The UNDERSTANDING: Ibro CourseNura Eky VNo ratings yet
- Spleen: - Site of Lymphocyte Proliferation - Immune Surveillance and Response - Cleanses The BloodDocument13 pagesSpleen: - Site of Lymphocyte Proliferation - Immune Surveillance and Response - Cleanses The BloodNura Eky VNo ratings yet
- Keseimbangan Asam BasaDocument2 pagesKeseimbangan Asam BasaNura Eky VNo ratings yet
- Obesity Review MelaninDocument12 pagesObesity Review MelaninNura Eky VNo ratings yet
- Acute Diseases and Life-Threatening Conditions: Assistant Professor Kenan KaravdićDocument33 pagesAcute Diseases and Life-Threatening Conditions: Assistant Professor Kenan KaravdićGoran MaliNo ratings yet
- Supliment-2022 RJC PDFDocument320 pagesSupliment-2022 RJC PDFSimona IonitaNo ratings yet
- 1.8.2 HandoutDocument4 pages1.8.2 Handoutkhushisarfraz123No ratings yet
- Types of Myocardial InfarctionDocument4 pagesTypes of Myocardial InfarctionntnquynhproNo ratings yet
- Assessing Operability of Congenital Heart Defects With Elevated Pulmonary Vascular ResistanceDocument6 pagesAssessing Operability of Congenital Heart Defects With Elevated Pulmonary Vascular ResistancedeepaNo ratings yet
- Human Heart ScienceDocument7 pagesHuman Heart ScienceJewel Kathryn MorenoNo ratings yet
- Cardiopulmonary Resuscitation: Dr. Abdul Rashad Senior Lecturer United College of Physical TherapyDocument27 pagesCardiopulmonary Resuscitation: Dr. Abdul Rashad Senior Lecturer United College of Physical TherapypashaNo ratings yet
- Tissues and Intro To Circulation 2014 2Document51 pagesTissues and Intro To Circulation 2014 2Chantae JulienNo ratings yet
- Algo Pals BLS Pediatric Cardiac ArrestDocument1 pageAlgo Pals BLS Pediatric Cardiac ArrestSiti NabilaNo ratings yet
- USMLE World Step 3 High Yield Notes 90 PagesDocument90 pagesUSMLE World Step 3 High Yield Notes 90 PagesVS95% (55)
- Circuit Weight Training in Cardiac PatientsDocument5 pagesCircuit Weight Training in Cardiac PatientsVivin YulvinaNo ratings yet
- CVS-System Wise 1700 document team contribution guideDocument158 pagesCVS-System Wise 1700 document team contribution guideBio DataNo ratings yet
- Incidence of Venous Air Embolism During Craniectomy For Craniosynostosis RepairDocument4 pagesIncidence of Venous Air Embolism During Craniectomy For Craniosynostosis RepairFika Khulma SofiaNo ratings yet
- EmbolizacionDocument8 pagesEmbolizacionnatalia.gallinoNo ratings yet
- Assessment of Cardiovascular Function Hinkle PPT CH 25Document26 pagesAssessment of Cardiovascular Function Hinkle PPT CH 25DelindaEvans100% (1)
- Perioperative Management of Patients With End-Stage Renal DiseaseDocument17 pagesPerioperative Management of Patients With End-Stage Renal DiseaseAn JNo ratings yet
- ECG InterpretationDocument5 pagesECG InterpretationRichelle Dianne Ramos-Giang100% (3)
- The Distribution of Hypertension in The Philippine General Hospital After 4 Decades (A Comparative Study)Document4 pagesThe Distribution of Hypertension in The Philippine General Hospital After 4 Decades (A Comparative Study)dennisNo ratings yet
- Phys9 06 1Document6 pagesPhys9 06 1alifia azzahraNo ratings yet
- Suz 183Document29 pagesSuz 183Benny Chris TantoNo ratings yet
- Physioex Lab Report: Pre-Lab Quiz ResultsDocument3 pagesPhysioex Lab Report: Pre-Lab Quiz ResultsPavel MilenkovskiNo ratings yet
- Basic Concepts in Exercise PhysiologyDocument40 pagesBasic Concepts in Exercise PhysiologyHammad AqibNo ratings yet
- Impact of High Sensitivity Troponins For 6nov Cardiac ForumDocument39 pagesImpact of High Sensitivity Troponins For 6nov Cardiac Forummouna6685No ratings yet
- ALTERATION/ ABNORMAL FINDINGS IN PULSEDocument7 pagesALTERATION/ ABNORMAL FINDINGS IN PULSEShalabh JoharyNo ratings yet
- Myocardial Bridging Presenting As An Acute CoronarDocument8 pagesMyocardial Bridging Presenting As An Acute Coronarfita triastuti /ananda syifa ahmad syamilNo ratings yet
- Left Sided Heart FailureDocument25 pagesLeft Sided Heart FailurePaulNo ratings yet
- Chest Pain FinalDocument17 pagesChest Pain FinalVarun R'MenonNo ratings yet
- Basic ECGDocument152 pagesBasic ECGTuấn Thanh VõNo ratings yet
- Checking Vital Signs ReportDocument3 pagesChecking Vital Signs ReportLuthi PratiwiNo ratings yet
- Lab 4 Handout Cardiac Physiology II (ECG BP HR)Document6 pagesLab 4 Handout Cardiac Physiology II (ECG BP HR)Wilson CheungNo ratings yet