You might also like
- Exercise Physiology for the Pediatric and Congenital CardiologistFrom EverandExercise Physiology for the Pediatric and Congenital CardiologistNo ratings yet
- De Paula 2017Document21 pagesDe Paula 2017TAINAH DE PAULANo ratings yet
- s-0042-104197Document8 pagess-0042-104197Leticia N. S. NevesNo ratings yet
- Inter HugoDocument10 pagesInter HugorizkaNo ratings yet
- Am J Hypertens 2015 Sharman 147 58Document12 pagesAm J Hypertens 2015 Sharman 147 58yusnadiNo ratings yet
- Accepted Manuscript: Journal of The American Society of HypertensionDocument17 pagesAccepted Manuscript: Journal of The American Society of HypertensionLeticia N. S. NevesNo ratings yet
- Physical Activity and Fitness For The Prevention of HypertensionDocument8 pagesPhysical Activity and Fitness For The Prevention of HypertensionFerdy LainsamputtyNo ratings yet
- Acute Resistance Exercise With Blood Flow Restriction in Elderly Hypertensive Women: Haemodynamic, Rating of Perceived Exertion and Blood LactateDocument8 pagesAcute Resistance Exercise With Blood Flow Restriction in Elderly Hypertensive Women: Haemodynamic, Rating of Perceived Exertion and Blood LactateJuanfran Montesinos GarciaNo ratings yet
- Artigo Completo Pei Fisio 1Document13 pagesArtigo Completo Pei Fisio 1harlley sanNo ratings yet
- 2022 Strength Training For Arterial Hypertension Treatment A Systematic Review and Meta-Analysis of Randomize Clinical TrialsDocument15 pages2022 Strength Training For Arterial Hypertension Treatment A Systematic Review and Meta-Analysis of Randomize Clinical TrialsAntofa V EndeNo ratings yet
- A Single Session of Aerobic Exercise Reduces Systolic Blood Pressure at Rest and in Response To Stress in Women With Rheumatoid Arthritis and HypertensionDocument9 pagesA Single Session of Aerobic Exercise Reduces Systolic Blood Pressure at Rest and in Response To Stress in Women With Rheumatoid Arthritis and HypertensionRobles Murillo Carlos Eduardo Augusto 1FNo ratings yet
- Brazilian Journal of Physical TherapyDocument12 pagesBrazilian Journal of Physical TherapyKen ABNo ratings yet
- Experimental Gerontology: ArticleinfoDocument7 pagesExperimental Gerontology: ArticleinfoLaily Mita AndriaNo ratings yet
- Rev Bras Hum: CineantropomDocument11 pagesRev Bras Hum: CineantropomGabriel ArcenioNo ratings yet
- Exercício Físico e Autofagia Seletiva Benefício e Risco Na Saúde CardiovascularDocument18 pagesExercício Físico e Autofagia Seletiva Benefício e Risco Na Saúde CardiovascularHenrique WilliamNo ratings yet
- Diferent Exercise TrainingDocument9 pagesDiferent Exercise TrainingRenan Carraro RosaNo ratings yet
- Review Article: Acute Effects of Exercise On Blood Pressure: A Meta-Analytic InvestigationDocument12 pagesReview Article: Acute Effects of Exercise On Blood Pressure: A Meta-Analytic InvestigationFisio KineticNo ratings yet
- J Strength Cond Res - 2011 - A Comparison of The Immediate Effects of Resistance, Aerobic, and Concurrent Exercise On Postexercise HypotensionDocument8 pagesJ Strength Cond Res - 2011 - A Comparison of The Immediate Effects of Resistance, Aerobic, and Concurrent Exercise On Postexercise HypotensionTAINAH DE PAULANo ratings yet
- Exercise Training For Blood Pressure: A Systematic Review and Meta-AnalysisDocument9 pagesExercise Training For Blood Pressure: A Systematic Review and Meta-AnalysisAnonymous 7dsX2F8nNo ratings yet
- A Comparison of The Immediate Effects of Resistance, Aerobic, and Concurrent Exercise On Postexercise HypotensionDocument8 pagesA Comparison of The Immediate Effects of Resistance, Aerobic, and Concurrent Exercise On Postexercise HypotensionTAINAH DE PAULANo ratings yet
- Physiological Mechanisms of the Athlete's Heart and the Volume of Exercise Needed for Cardiac AdaptationsDocument6 pagesPhysiological Mechanisms of the Athlete's Heart and the Volume of Exercise Needed for Cardiac AdaptationsJasmina Pluncevic GligoroskaNo ratings yet
- (Human Movement) Blood Pressure Responses After A Session of Functional Training in Young Adults and The Elderly A Pilot StudyDocument7 pages(Human Movement) Blood Pressure Responses After A Session of Functional Training in Young Adults and The Elderly A Pilot StudyEvaNo ratings yet
- Tensión Arterial y Ejercicio de FuerzaDocument8 pagesTensión Arterial y Ejercicio de Fuerzaabraham landaetaNo ratings yet
- HRV Powerlift JSSC 2011Document7 pagesHRV Powerlift JSSC 2011Claudio FerranteNo ratings yet
- Hypertension and ExerciseDocument8 pagesHypertension and ExercisemeyqiNo ratings yet
- Final Project Exp590-3Document19 pagesFinal Project Exp590-3api-315973465No ratings yet
- Letter To The Editor Hydrotherapy in Heart Failure: A Case: BackgroundDocument4 pagesLetter To The Editor Hydrotherapy in Heart Failure: A Case: BackgroundElizabete MonteiroNo ratings yet
- 1985-Cardiac Adaptations To Chronic ExerciseDocument28 pages1985-Cardiac Adaptations To Chronic ExerciseJavier Mora BaizNo ratings yet
- FileDocument8 pagesFilealexdinoy249No ratings yet
- Cardiologia: Post-Exercise Hypotension in Response To High-Intensity Interval Exercise: Potential MechanismsDocument3 pagesCardiologia: Post-Exercise Hypotension in Response To High-Intensity Interval Exercise: Potential MechanismsLeticia N. S. NevesNo ratings yet
- PHY2 8 E14455Document14 pagesPHY2 8 E14455Alexis Arce AlvarezNo ratings yet
- Ejercicio IntervalosDocument7 pagesEjercicio IntervalosOmar DVNo ratings yet
- Krustrup et al_2009_Recreational soccer is an effective health-promoting activity for untrained menDocument7 pagesKrustrup et al_2009_Recreational soccer is an effective health-promoting activity for untrained menIainNo ratings yet
- Terapi HT PDFDocument9 pagesTerapi HT PDFHamdaniNo ratings yet
- Dose-Response Relationship of The Cardiovascular Adaptation To Endurance Training in Healthy Adults: How Much Training For What Benefit?Document9 pagesDose-Response Relationship of The Cardiovascular Adaptation To Endurance Training in Healthy Adults: How Much Training For What Benefit?Choiri Khumaidah FikriyahNo ratings yet
- Marchese 2019 Controlled Study of Central Hemodynamic ChangesDocument8 pagesMarchese 2019 Controlled Study of Central Hemodynamic Changestaaaatan.04No ratings yet
- Thematic Poster Bioenergetics and Training: (No Relationships Reported)Document2 pagesThematic Poster Bioenergetics and Training: (No Relationships Reported)pantufoNo ratings yet
- WJC 3 248Document8 pagesWJC 3 248RIAN NUGRAHANo ratings yet
- Ijerph 17 07233Document12 pagesIjerph 17 07233Mumtaz MaulanaNo ratings yet
- 22Document17 pages22sani widya firnandaNo ratings yet
- S0003999321002963Document10 pagesS0003999321002963Nura Eky VNo ratings yet
- Breathing Training For Older Patients WithDocument28 pagesBreathing Training For Older Patients WithRieke Desti LegianaNo ratings yet
- Intra Dial y TicDocument8 pagesIntra Dial y Ticratna220693No ratings yet
- Peripheral Heart Action (PHA) Training As A Valid Substitute To High Intensity Interval Training To Improve Resting Cardiovascular Changes and Autonomic Adaptation Piras201Document11 pagesPeripheral Heart Action (PHA) Training As A Valid Substitute To High Intensity Interval Training To Improve Resting Cardiovascular Changes and Autonomic Adaptation Piras201jojoNo ratings yet
- AHA Heart Article 2 Week 13Document12 pagesAHA Heart Article 2 Week 13beniak_preNo ratings yet
- Inter-And Intra-Individual Analysis of Post-Exercise Hypotension Following A Single Bout of High-Intensity Interval Exercise and Continuous Exercise: A Pilot StudyDocument6 pagesInter-And Intra-Individual Analysis of Post-Exercise Hypotension Following A Single Bout of High-Intensity Interval Exercise and Continuous Exercise: A Pilot Studynuttela ismeNo ratings yet
- JHH 2013 121Document5 pagesJHH 2013 121adri20121989No ratings yet
- JEP Journal of Exercise PhysiologyDocument7 pagesJEP Journal of Exercise PhysiologykambuaNo ratings yet
- Aerobic Versus Isometric Handgrip Exercise in Hypertension: A Randomized Controlled TrialDocument8 pagesAerobic Versus Isometric Handgrip Exercise in Hypertension: A Randomized Controlled TrialROSANo ratings yet
- Associations Between Borgs' Rating of Perceived Exertion and Physiological Measures of Exercise Intensity # ControlDocument9 pagesAssociations Between Borgs' Rating of Perceived Exertion and Physiological Measures of Exercise Intensity # ControlVinicius Fallux QueirozNo ratings yet
- The Effect of Pursed - Lip Breathing Exercise Vs Diaphragmatic Breathing in Stabilizing The Vitals After 6-MWT Among Overweight Individuals-IJRASETDocument12 pagesThe Effect of Pursed - Lip Breathing Exercise Vs Diaphragmatic Breathing in Stabilizing The Vitals After 6-MWT Among Overweight Individuals-IJRASETIJRASETPublicationsNo ratings yet
- Postexercise Hypotension in An Endurance-Trained Population of Men and Women Following High-Intensity Interval and Steady-State CyclingDocument10 pagesPostexercise Hypotension in An Endurance-Trained Population of Men and Women Following High-Intensity Interval and Steady-State Cyclingnuttela ismeNo ratings yet
- Cardiac Physiology in Acute and Chronic Endurance ExcerciseDocument27 pagesCardiac Physiology in Acute and Chronic Endurance ExcerciseKevin MulyaNo ratings yet
- Effects of Exercise On Quality of Life in Stroke Survivors: A Meta-AnalysisDocument12 pagesEffects of Exercise On Quality of Life in Stroke Survivors: A Meta-AnalysisNoor KameliaNo ratings yet
- Zouhal Et Al-2021-The Effects of Exercise Training On Plasma Volume Variations A Systematic ReviewDocument34 pagesZouhal Et Al-2021-The Effects of Exercise Training On Plasma Volume Variations A Systematic ReviewMumtaz MaulanaNo ratings yet
- Isometric TrainingDocument7 pagesIsometric Trainingsilvio da costa guerreiroNo ratings yet
- 13-09-2021-1631535170-6-Impact - Ijrhal-3. Prescribing Exercise Intensity For Healthy Using Perceived Exertion DR Adesola - 1Document14 pages13-09-2021-1631535170-6-Impact - Ijrhal-3. Prescribing Exercise Intensity For Healthy Using Perceived Exertion DR Adesola - 1Impact JournalsNo ratings yet
- Feasibility and Estimated Efficacy of Blood Flow Restricted Training in Female Patients With Rheumatoid Arthritis A Randomized Controlled Pilot StudyDocument10 pagesFeasibility and Estimated Efficacy of Blood Flow Restricted Training in Female Patients With Rheumatoid Arthritis A Randomized Controlled Pilot StudyDaniel Andrés Bulla GarcíaNo ratings yet
- A Post Hoc Analysis On Rhythm and High Intensity Interval Training in Cardiac Resynchronization TherapyDocument10 pagesA Post Hoc Analysis On Rhythm and High Intensity Interval Training in Cardiac Resynchronization TherapyNinaRomorNo ratings yet
- Bangsbo Et Al. - 2015 - Recreational Football For Disease Prevention and Treatment in Untrained Men A Narrative Review Examining CardiovDocument10 pagesBangsbo Et Al. - 2015 - Recreational Football For Disease Prevention and Treatment in Untrained Men A Narrative Review Examining CardiovABDALMAJED ALMOTERYNo ratings yet
- Farinatti 2021Document12 pagesFarinatti 2021TAINAH DE PAULANo ratings yet
- Fidalgo Et Al - 2019Document15 pagesFidalgo Et Al - 2019TAINAH DE PAULANo ratings yet
- De Paula 2021Document8 pagesDe Paula 2021TAINAH DE PAULANo ratings yet
- J Strength Cond Res - 2011 - A Comparison of The Immediate Effects of Resistance, Aerobic, and Concurrent Exercise On Postexercise HypotensionDocument8 pagesJ Strength Cond Res - 2011 - A Comparison of The Immediate Effects of Resistance, Aerobic, and Concurrent Exercise On Postexercise HypotensionTAINAH DE PAULANo ratings yet
- The Aftereffects of Dynamic Exercise On Ambulatory Blood PressureDocument7 pagesThe Aftereffects of Dynamic Exercise On Ambulatory Blood PressureTAINAH DE PAULANo ratings yet
- Post-Concurrent Exercise Hemodynamics and Cardiac Autonomic ModulationDocument10 pagesPost-Concurrent Exercise Hemodynamics and Cardiac Autonomic ModulationTAINAH DE PAULANo ratings yet
- Barros Et Al - 2021Document14 pagesBarros Et Al - 2021TAINAH DE PAULANo ratings yet
- Munir Et Al 2007 Exercise Reduces Arterial Pressure Augmentation Through Vasodilation of Muscular Arteries in HumansDocument6 pagesMunir Et Al 2007 Exercise Reduces Arterial Pressure Augmentation Through Vasodilation of Muscular Arteries in HumansTAINAH DE PAULANo ratings yet
- A Comparison of The Immediate Effects of Resistance, Aerobic, and Concurrent Exercise On Postexercise HypotensionDocument8 pagesA Comparison of The Immediate Effects of Resistance, Aerobic, and Concurrent Exercise On Postexercise HypotensionTAINAH DE PAULANo ratings yet
- Yoon Et Al 2010effects of Acute Resistance Exercise On Arterial Stiffness in Young MenDocument7 pagesYoon Et Al 2010effects of Acute Resistance Exercise On Arterial Stiffness in Young MenTAINAH DE PAULANo ratings yet
- Exercise Reduces Arterial Pressure Augmentation Through Vasodilation of Muscular Arteries in HumansDocument6 pagesExercise Reduces Arterial Pressure Augmentation Through Vasodilation of Muscular Arteries in HumansTAINAH DE PAULANo ratings yet
- Clinical Significance of Cardiac Damage and Changes in Function After Exercise.Document8 pagesClinical Significance of Cardiac Damage and Changes in Function After Exercise.TAINAH DE PAULANo ratings yet
- Clinical Significance of Cardiac Damage and Changes in Function After Exercise.Document8 pagesClinical Significance of Cardiac Damage and Changes in Function After Exercise.TAINAH DE PAULANo ratings yet
- Yoon Et Al 2010effects of Acute Resistance Exercise On Arterial Stiffness in Young MenDocument7 pagesYoon Et Al 2010effects of Acute Resistance Exercise On Arterial Stiffness in Young MenTAINAH DE PAULANo ratings yet
- Differential Response of Central Blood Pressure To Isometric and Isotonic ExerciseDocument5 pagesDifferential Response of Central Blood Pressure To Isometric and Isotonic ExerciseTAINAH DE PAULANo ratings yet
- SportMedicine2009 Cuantificacion EntrenamientoDocument18 pagesSportMedicine2009 Cuantificacion EntrenamientoParra VictorNo ratings yet
- Test A: Reading - Passage 1Document29 pagesTest A: Reading - Passage 1barishyayNo ratings yet
- ป 6Document43 pagesป 6MoLo Kanyarat ChenpitaksombatNo ratings yet
- April 12th Test PDFDocument32 pagesApril 12th Test PDFهخه •No ratings yet
- Septic Abortion PDFDocument4 pagesSeptic Abortion PDFmariachrismayaniNo ratings yet
- Pearly Co Cleared Funds ForecastDocument8 pagesPearly Co Cleared Funds ForecastPutin Phy0% (1)
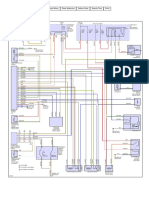
- Aire Acondicionado Mazda 3 2006Document2 pagesAire Acondicionado Mazda 3 2006Jhon ConnorNo ratings yet
- GMP TD Ar FPL 11033Document1 pageGMP TD Ar FPL 11033Sammy NguyenNo ratings yet
- Mbenson hw410 1602c - Unit-9-AssignmentDocument46 pagesMbenson hw410 1602c - Unit-9-Assignmentapi-355858071No ratings yet
- Population Ecology: Aecc-I +3 1 YearDocument32 pagesPopulation Ecology: Aecc-I +3 1 YearAnita kumari SahuNo ratings yet
- Bibliometric Handbook For Karolinska InstitutetDocument41 pagesBibliometric Handbook For Karolinska InstitutetCamila Araya G100% (1)
- Trisyl Silica Gel: For Oils/Fats and Biofuel RefiningDocument4 pagesTrisyl Silica Gel: For Oils/Fats and Biofuel RefiningJosé Mauricio Bonilla TobónNo ratings yet
- Quiz Integumentary SystemDocument23 pagesQuiz Integumentary SystemLemuel CunananNo ratings yet
- Amul India Case Study: Product Portfolio and SWOT AnalysisDocument10 pagesAmul India Case Study: Product Portfolio and SWOT AnalysisShruti NagmoteNo ratings yet
- Sound Level MeterDocument11 pagesSound Level MeterFityatal HasanahNo ratings yet
- Government Schemes Current Affairs PDF E Book PDFDocument106 pagesGovernment Schemes Current Affairs PDF E Book PDFRohini VjNo ratings yet
- Kristeva On Melanie Klein's "Oresteia"Document6 pagesKristeva On Melanie Klein's "Oresteia"danthetoasterNo ratings yet
- Healthy Lifestyle HabitsDocument2 pagesHealthy Lifestyle HabitsJesus BaldeonNo ratings yet
- Rocket Motor Head-end Structural AnalysisDocument83 pagesRocket Motor Head-end Structural AnalysisRudra Sai SandeepNo ratings yet
- Gaggia Cadorna Milk Full Instruction ManualDocument76 pagesGaggia Cadorna Milk Full Instruction ManualKanen Coffee, LLC.No ratings yet
- Sprocket Asa 180Document1 pageSprocket Asa 180jhampolrosalesNo ratings yet
- Music and Therapy Bun2Document17 pagesMusic and Therapy Bun2PanteaAlisaNo ratings yet
- FarkolDocument7 pagesFarkolHasiadin LaodeNo ratings yet
- Torc 4 Abscohort1 - CompressDocument13 pagesTorc 4 Abscohort1 - CompressFaye MartinezNo ratings yet
- Starbucks BSC Project Analyzes Store PerformanceDocument8 pagesStarbucks BSC Project Analyzes Store Performanceandrea100% (1)
- 2020 End Year 6 PenulisanDocument8 pages2020 End Year 6 PenulisanZulhillmi ZainuddinNo ratings yet
- Celecoxib Identification MethodsDocument5 pagesCelecoxib Identification Methodsabc1679No ratings yet
- Alpine Valley Liability ReleaseDocument1 pageAlpine Valley Liability ReleaseChristina Nakazaki0% (1)
- Queuing System Optimization for Mercury Drug StoreDocument17 pagesQueuing System Optimization for Mercury Drug StoreAllen Agno llNo ratings yet
- Positive Thinking GuideDocument23 pagesPositive Thinking GuideSimon Brassard100% (1)
- BW Mc2 XWHM y Na ManualDocument23 pagesBW Mc2 XWHM y Na ManualSatyasrinivas PulavarthiNo ratings yet
- Functional Training and Beyond: Building the Ultimate Superfunctional Body and MindFrom EverandFunctional Training and Beyond: Building the Ultimate Superfunctional Body and MindRating: 4.5 out of 5 stars4.5/5 (1)
- Aging Backwards: Reverse the Aging Process and Look 10 Years Younger in 30 Minutes a DayFrom EverandAging Backwards: Reverse the Aging Process and Look 10 Years Younger in 30 Minutes a DayNo ratings yet
- Chair Yoga: Sit, Stretch, and Strengthen Your Way to a Happier, Healthier YouFrom EverandChair Yoga: Sit, Stretch, and Strengthen Your Way to a Happier, Healthier YouRating: 3.5 out of 5 stars3.5/5 (5)
- Whole Body Barefoot: Transitioning Well to Minimal FootwearFrom EverandWhole Body Barefoot: Transitioning Well to Minimal FootwearRating: 4 out of 5 stars4/5 (16)
- Strong Is the New Beautiful: Embrace Your Natural Beauty, Eat Clean, and Harness Your PowerFrom EverandStrong Is the New Beautiful: Embrace Your Natural Beauty, Eat Clean, and Harness Your PowerRating: 4 out of 5 stars4/5 (5)
- Body by Science: A Research Based Program for Strength Training, Body building, and Complete Fitness in 12 Minutes a WeekFrom EverandBody by Science: A Research Based Program for Strength Training, Body building, and Complete Fitness in 12 Minutes a WeekRating: 4.5 out of 5 stars4.5/5 (84)
- Music For Healing: With Nature Sounds For Natural Healing Powers: Sounds Of Nature, Deep Sleep Music, Meditation, Relaxation, Healing MusicFrom EverandMusic For Healing: With Nature Sounds For Natural Healing Powers: Sounds Of Nature, Deep Sleep Music, Meditation, Relaxation, Healing MusicRating: 5 out of 5 stars5/5 (1)
- Power of 10: The Once-A-Week Slow Motion Fitness RevolutionFrom EverandPower of 10: The Once-A-Week Slow Motion Fitness RevolutionRating: 3.5 out of 5 stars3.5/5 (11)
- Peak: The New Science of Athletic Performance That is Revolutionizing SportsFrom EverandPeak: The New Science of Athletic Performance That is Revolutionizing SportsRating: 5 out of 5 stars5/5 (95)
- Boundless: Upgrade Your Brain, Optimize Your Body & Defy AgingFrom EverandBoundless: Upgrade Your Brain, Optimize Your Body & Defy AgingRating: 4.5 out of 5 stars4.5/5 (66)
- Endure: Mind, Body, and the Curiously Elastic Limits of Human PerformanceFrom EverandEndure: Mind, Body, and the Curiously Elastic Limits of Human PerformanceRating: 4.5 out of 5 stars4.5/5 (237)
- The Seven Spiritual Laws of Yoga: A Practical Guide to Healing Body, Mind, and SpiritFrom EverandThe Seven Spiritual Laws of Yoga: A Practical Guide to Healing Body, Mind, and SpiritRating: 4.5 out of 5 stars4.5/5 (73)
- Weight Lifting Is a Waste of Time: So Is Cardio, and There’s a Better Way to Have the Body You WantFrom EverandWeight Lifting Is a Waste of Time: So Is Cardio, and There’s a Better Way to Have the Body You WantRating: 4.5 out of 5 stars4.5/5 (38)
- Relentless: From Good to Great to UnstoppableFrom EverandRelentless: From Good to Great to UnstoppableRating: 5 out of 5 stars5/5 (782)
- Muscle for Life: Get Lean, Strong, and Healthy at Any Age!From EverandMuscle for Life: Get Lean, Strong, and Healthy at Any Age!Rating: 4.5 out of 5 stars4.5/5 (22)
- Not a Diet Book: Take Control. Gain Confidence. Change Your Life.From EverandNot a Diet Book: Take Control. Gain Confidence. Change Your Life.Rating: 4.5 out of 5 stars4.5/5 (124)
- Yamas & Niyamas: Exploring Yoga's Ethical PracticeFrom EverandYamas & Niyamas: Exploring Yoga's Ethical PracticeRating: 4.5 out of 5 stars4.5/5 (110)
- Roxane Gay & Everand Originals: Built for This: The Quiet Strength of PowerliftingFrom EverandRoxane Gay & Everand Originals: Built for This: The Quiet Strength of PowerliftingRating: 4.5 out of 5 stars4.5/5 (132)
- You: Breathing Easy: Meditation and Breathing Techniques to Relax, Refresh and RevitalizeFrom EverandYou: Breathing Easy: Meditation and Breathing Techniques to Relax, Refresh and RevitalizeRating: 3 out of 5 stars3/5 (5)
- SAS Training Manual: How to get fit enough to pass a special forces selection courseFrom EverandSAS Training Manual: How to get fit enough to pass a special forces selection courseRating: 4 out of 5 stars4/5 (3)
- The Yogi Code: Seven Universal Laws of Infinite SuccessFrom EverandThe Yogi Code: Seven Universal Laws of Infinite SuccessRating: 4.5 out of 5 stars4.5/5 (104)
- Body by Science: A Research Based Program to Get the Results You Want in 12 Minutes a WeekFrom EverandBody by Science: A Research Based Program to Get the Results You Want in 12 Minutes a WeekRating: 4 out of 5 stars4/5 (38)
- Buteyko Breathing Course Manual: For use with the Advanced Buteyko CourseFrom EverandButeyko Breathing Course Manual: For use with the Advanced Buteyko CourseRating: 5 out of 5 stars5/5 (1)
- Wall Pilates: Quick-and-Simple to Lose Weight and Stay Healthy. A 30-Day Journey with + 100 ExercisesFrom EverandWall Pilates: Quick-and-Simple to Lose Weight and Stay Healthy. A 30-Day Journey with + 100 ExercisesNo ratings yet
- The Yamas & Niyamas: Exploring Yoga's Ethical PracticeFrom EverandThe Yamas & Niyamas: Exploring Yoga's Ethical PracticeRating: 4.5 out of 5 stars4.5/5 (19)
- The Calisthenics Codex: Fifty Exercises for Functional FitnessFrom EverandThe Calisthenics Codex: Fifty Exercises for Functional FitnessRating: 4 out of 5 stars4/5 (9)
- 7 Weeks to 10 Pounds of Muscle: The Complete Day-by-Day Program to Pack on Lean, Healthy Muscle MassFrom Everand7 Weeks to 10 Pounds of Muscle: The Complete Day-by-Day Program to Pack on Lean, Healthy Muscle MassRating: 4 out of 5 stars4/5 (2)