You might also like
- Fluid and Electrolytes for Nursing StudentsFrom EverandFluid and Electrolytes for Nursing StudentsRating: 5 out of 5 stars5/5 (12)
- Lung Expansion RevisionDocument89 pagesLung Expansion RevisionPatrick RoqueNo ratings yet
- Respiratory Emergencies: Eileen Humphreys PA-C, EMT-IDocument71 pagesRespiratory Emergencies: Eileen Humphreys PA-C, EMT-IChristian JaraNo ratings yet
- CPAP SlidesDocument52 pagesCPAP SlidesAnusha Verghese100% (1)
- When The Ventilator Alarm Sounds SANTANILLADocument58 pagesWhen The Ventilator Alarm Sounds SANTANILLAAshish PandeyNo ratings yet
- Respiratory Assessment OHT Branding EditsDocument25 pagesRespiratory Assessment OHT Branding EditsDeepika LingamNo ratings yet
- How To Approach Dyspnea in ED - Pramono SigitDocument29 pagesHow To Approach Dyspnea in ED - Pramono SigitLeonita DwiNo ratings yet
- 2021 Lecture COPD & Asthma Full Size NotesDocument73 pages2021 Lecture COPD & Asthma Full Size NotesChelsea JiangNo ratings yet
- Bronchial HygieneDocument37 pagesBronchial HygieneRayan MohhamadNo ratings yet
- Bantuan Hidup Dasar (BHD) : Dr. Zulkimaulub R Span Bagian Anestesiology Dan Reanimasi Rsud M Yunus BengkuluDocument77 pagesBantuan Hidup Dasar (BHD) : Dr. Zulkimaulub R Span Bagian Anestesiology Dan Reanimasi Rsud M Yunus Bengkulupkm cgdmNo ratings yet
- Assessment of Critically Ill Patient Lec-1Document9 pagesAssessment of Critically Ill Patient Lec-1lshj318No ratings yet
- Advanced Cardiac Life SupportDocument42 pagesAdvanced Cardiac Life SupportDennis MiritiNo ratings yet
- WCS 011 - Low BP or Fast Pulse and No BP No Pulse - by Prof M Irwin (Updated)Document64 pagesWCS 011 - Low BP or Fast Pulse and No BP No Pulse - by Prof M Irwin (Updated)RachelMokNo ratings yet
- Understanding Mechanical Ventilation: Jennifer Zanni, PT, DSCPT Johns Hopkins HospitalDocument52 pagesUnderstanding Mechanical Ventilation: Jennifer Zanni, PT, DSCPT Johns Hopkins HospitalDeepa BhattacharjeeNo ratings yet
- Advance Trauma Life SupportDocument67 pagesAdvance Trauma Life SupportraffellaNo ratings yet
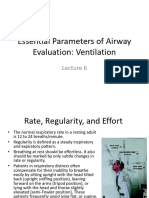
- Essential Parameters of Airway Evaluation Lecture 6Document27 pagesEssential Parameters of Airway Evaluation Lecture 69yqgmkvyzdNo ratings yet
- Dept. of Anesthesiology & Reanimation Airlangga University School of Medicine SurabayaDocument32 pagesDept. of Anesthesiology & Reanimation Airlangga University School of Medicine SurabayamerrynoviNo ratings yet
- Shortness of BreathDocument49 pagesShortness of BreathMetkaNo ratings yet
- Asthma Nur220 Student PowerpointDocument26 pagesAsthma Nur220 Student PowerpointPaula BissetteNo ratings yet
- 2-Shortness of Breath by DR - HananDocument49 pages2-Shortness of Breath by DR - HananSoon SheedNo ratings yet
- Vital Signs: Jeffrey Evangelista, RN, MANDocument52 pagesVital Signs: Jeffrey Evangelista, RN, MANHikari 光 ShidouNo ratings yet
- Lung Expansion 1Document31 pagesLung Expansion 11trindogg100% (2)
- CPPT in The IcuDocument39 pagesCPPT in The Icueyob kaseyeNo ratings yet
- Chapter 07 Taking Vital SignsDocument22 pagesChapter 07 Taking Vital SignsNephNo ratings yet
- Human Factors and Pilot Performance: Section 1 Human Physiology and The Affects of AltitudeDocument19 pagesHuman Factors and Pilot Performance: Section 1 Human Physiology and The Affects of Altitudealex962No ratings yet
- Vitals ObservationsDocument52 pagesVitals ObservationsletticianabunyaNo ratings yet
- 1.1 Obtaining Vital SignsDocument66 pages1.1 Obtaining Vital SignsJomaleah OficiarNo ratings yet
- Nursing Skills (Vital Signs) PDFDocument48 pagesNursing Skills (Vital Signs) PDFkhizer hayatNo ratings yet
- Assessment of The Acutely Ill PatientDocument10 pagesAssessment of The Acutely Ill PatientZacmilo Dela TorreNo ratings yet
- Assessment Cardiovascular Sy - 1Document32 pagesAssessment Cardiovascular Sy - 1TASNEEM LAKKADSHANo ratings yet
- Physical Examination Techniques and ManueversDocument160 pagesPhysical Examination Techniques and ManueversMa-anJaneDiamosNo ratings yet
- Performed Structural DesignDocument93 pagesPerformed Structural DesignSaiful IslamNo ratings yet
- Breathing & CirculationDocument40 pagesBreathing & CirculationRia UtamiNo ratings yet
- Bantuan Hidup DasarDocument77 pagesBantuan Hidup DasarKLINIK KIRANA MEDIKANo ratings yet
- Ventilator Waveforms: DR Barry Dixon ST - Vincent's Hospital Melbourne AustraliaDocument44 pagesVentilator Waveforms: DR Barry Dixon ST - Vincent's Hospital Melbourne AustraliaBenvenuto AxelNo ratings yet
- Module 2 Full SlidesDocument69 pagesModule 2 Full SlidesMaria Du-PastoralNo ratings yet
- Neonatal ResuscitationDocument46 pagesNeonatal ResuscitationAsaliwe BorahNo ratings yet
- Vishtasb DiagnosticDocument24 pagesVishtasb DiagnosticVishtasb KhaliliNo ratings yet
- SOAPIE Room 302 TelarmaDocument1 pageSOAPIE Room 302 TelarmaasdasdNo ratings yet
- Publication 2 21768 958Document41 pagesPublication 2 21768 958Safi MohammedNo ratings yet
- Life Support DocumentDocument9 pagesLife Support DocumentThe Print shopNo ratings yet
- ACLS NotesDocument9 pagesACLS Notestasha0% (1)
- Aha Acls GuideDocument11 pagesAha Acls GuideIrene PimentelNo ratings yet
- Case Presentation ETD (COPD)Document45 pagesCase Presentation ETD (COPD)Dzachary13No ratings yet
- Cpap - A Gentle VentilationDocument24 pagesCpap - A Gentle VentilationrobystwnNo ratings yet
- Basic Life SupportDocument101 pagesBasic Life SupportMasyfuk Zuhdi JamhurNo ratings yet
- Physiotherapy Assessment and Treatment On PICUDocument54 pagesPhysiotherapy Assessment and Treatment On PICUBatool Rehman100% (2)
- C.O.P.D: (Chronic Obstructive Pulmonary Disorder)Document47 pagesC.O.P.D: (Chronic Obstructive Pulmonary Disorder)KrystelNo ratings yet
- ModuleIV RespiratoryEmergencies CHF COPD AsthmaDocument96 pagesModuleIV RespiratoryEmergencies CHF COPD AsthmaSaiKiranNo ratings yet
- Osce Notes - Rac - Safina AdatiaDocument35 pagesOsce Notes - Rac - Safina AdatiaTraventure 2000No ratings yet
- Workshop #4 Internal Medicine IDocument78 pagesWorkshop #4 Internal Medicine IhevinpatelNo ratings yet
- Workshop #4 Internal Medicine IDocument78 pagesWorkshop #4 Internal Medicine Ihevinpatel100% (1)
- Oxygenation Part 1Document86 pagesOxygenation Part 1Shaira Mae Fangon De GuzmanNo ratings yet
- Anestesi - 02 Review UKMPPDDocument87 pagesAnestesi - 02 Review UKMPPDNia UswantiNo ratings yet
- Vital Signs: Sheila Arelli Garcia-Safra, PRTP, MhpedDocument26 pagesVital Signs: Sheila Arelli Garcia-Safra, PRTP, MhpedSheila SafraNo ratings yet
- Lecture 5 - Assessing Respiratory Function & Respiratory Care Modalities 2020-2021MTDocument47 pagesLecture 5 - Assessing Respiratory Function & Respiratory Care Modalities 2020-2021MTعمار عاشورNo ratings yet
- Respiratory DisordersDocument8 pagesRespiratory DisordersCezanne CruzNo ratings yet
- Anesthesia Emergencies AccidentsDocument9 pagesAnesthesia Emergencies Accidentsshubhangi godboleNo ratings yet
- Resp Lecture FinalDocument37 pagesResp Lecture Finalapi-195799092No ratings yet
- Periop For TIDocument31 pagesPeriop For TIBen ScottNo ratings yet
- Arrhythmic PatientsDocument15 pagesArrhythmic PatientsBen ScottNo ratings yet
- MDT PanelDocument33 pagesMDT PanelBen ScottNo ratings yet
- Charts and Hearts PDFDocument51 pagesCharts and Hearts PDFBen ScottNo ratings yet
- Controlled Drugs 2013Document1 pageControlled Drugs 2013Ben ScottNo ratings yet
- Latin Abbreviations Used in Prescription Writing 11Document1 pageLatin Abbreviations Used in Prescription Writing 11Ben ScottNo ratings yet
- Takeaway Special Menu July 2022Document1 pageTakeaway Special Menu July 2022Ben ScottNo ratings yet
- Legal Requirements For A Prescription.: Medicines Regulations 1984 R.41 Form of PrescriptionDocument2 pagesLegal Requirements For A Prescription.: Medicines Regulations 1984 R.41 Form of PrescriptionBen ScottNo ratings yet
- 2018 05 09 Primary Care Prescribing Guidelines For Drugs Used at The End of Life 1528456872Document5 pages2018 05 09 Primary Care Prescribing Guidelines For Drugs Used at The End of Life 1528456872Ben ScottNo ratings yet
- Takeaway Special Menu July 2022Document1 pageTakeaway Special Menu July 2022Ben ScottNo ratings yet
- ACFrOgDACnKE0rUjf42HXaSb36Wbju Urd7BPPqmTBRXMMFtZ91-fOr1fErSfh6BzXghJFKNYiKG5H-y3ET76l8IkKipRRxFa4B6gSp0OP6njH7C 5ulv8f C1cL DaDocument209 pagesACFrOgDACnKE0rUjf42HXaSb36Wbju Urd7BPPqmTBRXMMFtZ91-fOr1fErSfh6BzXghJFKNYiKG5H-y3ET76l8IkKipRRxFa4B6gSp0OP6njH7C 5ulv8f C1cL Dajelena_stankovic_34No ratings yet
- Respiratory FailureDocument46 pagesRespiratory FailureSintya RistriyaniNo ratings yet
- Acute Respiratory FailureDocument29 pagesAcute Respiratory FailurePurnima ChoudhuryNo ratings yet
- Respiratory Failure PresentationDocument13 pagesRespiratory Failure PresentationHusnain Irshad AlviNo ratings yet
- Niv BK 9051941 EnusDocument84 pagesNiv BK 9051941 EnusmatijahNo ratings yet
- Insuf Respiratória Aguda - RevisãoDocument19 pagesInsuf Respiratória Aguda - RevisãoksdposaNo ratings yet
- Nejm 2204556Document11 pagesNejm 2204556tommy taylor084No ratings yet
- Aicu Worksheet 1.Document4 pagesAicu Worksheet 1.Cyril SolimanNo ratings yet
- Optiflow Flow Matters Newsletter Edition 11 PM 621178Document3 pagesOptiflow Flow Matters Newsletter Edition 11 PM 621178Moas GabrounNo ratings yet
- Gagal NafasDocument33 pagesGagal NafastitoNo ratings yet
- Acute Respiratory Failure For StudentDocument41 pagesAcute Respiratory Failure For Studentapi-379952350% (4)
- Respiratory FailureDocument29 pagesRespiratory Failureageng rusbaya0% (1)
- Case Study For Acute Respiratory FailureDocument10 pagesCase Study For Acute Respiratory FailureGabbii CincoNo ratings yet
- Acute Respiratory FailureDocument7 pagesAcute Respiratory FailureNurol-Ainah Hafizah U. PimpingNo ratings yet
- E000170 Full PDFDocument20 pagesE000170 Full PDFdimas antaraNo ratings yet
- Lo Tropmed 1Document49 pagesLo Tropmed 1belleNo ratings yet
- Impaired Gas Exchange NCPDocument3 pagesImpaired Gas Exchange NCPMae Denn LabordoNo ratings yet
- Diagnosis: ARDS OverviewDocument5 pagesDiagnosis: ARDS OverviewLuvita RonteltapNo ratings yet
- Physioloical Integrity Acute Biologic CrisisDocument42 pagesPhysioloical Integrity Acute Biologic CrisisJohn Paul M. TagapanNo ratings yet
- Basic Principles of Oxygen TherapyDocument20 pagesBasic Principles of Oxygen TherapyAdikurniawan100% (1)
- Acute Respiratory FailureDocument28 pagesAcute Respiratory FailureMohamed Na3eemNo ratings yet
- I Am Sharing 'Case Study NCM 118' With YouDocument6 pagesI Am Sharing 'Case Study NCM 118' With YouQusai BassamNo ratings yet
- CHPT 70 Respiratory Part 2Document56 pagesCHPT 70 Respiratory Part 2helen brockNo ratings yet
- Respiratory FailureDocument52 pagesRespiratory FailureMohammad_Islam87100% (8)
- Quick Review of Some Medical TopicsDocument40 pagesQuick Review of Some Medical TopicsdoctormussieaberraNo ratings yet
- Oxygen InsufficiencyDocument70 pagesOxygen InsufficiencydaisyNo ratings yet
- Tatalaksana Hipoksemia Akut CovidDocument31 pagesTatalaksana Hipoksemia Akut CovidLilis Sumiyati100% (1)
- MOHFW Critical Care GuidelinesDocument123 pagesMOHFW Critical Care GuidelinesMOHAMMED IQBALNo ratings yet
- Caring For Mechanical Ventilated PatientDocument10 pagesCaring For Mechanical Ventilated Patientems100% (1)
- Basic Principles of Intensive Care NursingDocument24 pagesBasic Principles of Intensive Care NursingInstalasi PelayananJantungTerpaduNo ratings yet