You might also like
- Atlas of 3D Transesophageal Echocardiography in Structural Heart Disease Interventions: Cases and VideosFrom EverandAtlas of 3D Transesophageal Echocardiography in Structural Heart Disease Interventions: Cases and VideosNo ratings yet
- Cardiac Cath Lab PlanningDocument56 pagesCardiac Cath Lab PlanningPriyanka Satalkar60% (5)
- Textbook of Urgent Care Management: Chapter 35, Urgent Care Imaging and InterpretationFrom EverandTextbook of Urgent Care Management: Chapter 35, Urgent Care Imaging and InterpretationNo ratings yet
- Cardiac Cath Lab ReportDocument12 pagesCardiac Cath Lab ReportRumela Chakraborty100% (2)
- Cardiology Department: Iccu and WardsDocument12 pagesCardiology Department: Iccu and WardsPoojaNo ratings yet
- Magnetic Resonance Imaging: Recording, Reconstruction and AssessmentFrom EverandMagnetic Resonance Imaging: Recording, Reconstruction and AssessmentRating: 5 out of 5 stars5/5 (1)
- Impact of Artificial Intelligence On Interventional CardiologyDocument27 pagesImpact of Artificial Intelligence On Interventional CardiologyASIK1144No ratings yet
- Computer Applications in Health CareDocument20 pagesComputer Applications in Health CareUsman Suleman AhmadNo ratings yet
- Orientation To The Cath Lab NewDocument33 pagesOrientation To The Cath Lab NewMoch Irvan Badri100% (4)
- Information Technology Applicable in The Nursing Practice: A. Hospital and Critical Care ApplicationsDocument8 pagesInformation Technology Applicable in The Nursing Practice: A. Hospital and Critical Care ApplicationsRein ArgosinoNo ratings yet
- Improvement in Coronary Anastomosis WitDocument6 pagesImprovement in Coronary Anastomosis WitTerymar SthefannyNo ratings yet
- Hospital Spaces - Surgical SuiteDocument12 pagesHospital Spaces - Surgical SuiteJonalyn GarciaNo ratings yet
- JJ Clinical Engineering OverviewDocument16 pagesJJ Clinical Engineering OverviewFreddy VargasNo ratings yet
- Tracking healthcare providers in the ERDocument8 pagesTracking healthcare providers in the ERLorenzo GarciaNo ratings yet
- Healthcare and Technology: A Growing RelationshipDocument15 pagesHealthcare and Technology: A Growing RelationshipMartina GuaschNo ratings yet
- Cath Lab PlanningDocument20 pagesCath Lab PlanningJune Karki100% (1)
- Planning and Design of Radiology & Imaging SciencesDocument39 pagesPlanning and Design of Radiology & Imaging SciencesMariaNo ratings yet
- Remote Healthcare Monitoring SystemDocument5 pagesRemote Healthcare Monitoring Systemnallamal1006No ratings yet
- Information Technology System Applicable in Nursing PracticeDocument9 pagesInformation Technology System Applicable in Nursing PracticeZyrene Rivera100% (3)
- The Advanced Multimodality Image - Guided Operating (AMIGO) SuiteDocument30 pagesThe Advanced Multimodality Image - Guided Operating (AMIGO) Suitedan1kacherNo ratings yet
- DHA Part B Cardiac InvestigationsDocument37 pagesDHA Part B Cardiac InvestigationsFaisal OmarNo ratings yet
- Lec 4. Radiology WorkflowDocument24 pagesLec 4. Radiology Workflowallexa jimlaniNo ratings yet
- Cardiac Catheterization LaboratoryDocument5 pagesCardiac Catheterization LaboratoryDrAsra KhaleelNo ratings yet
- Trend 33 SmartorsDocument2 pagesTrend 33 SmartorsBingDelaCruzNo ratings yet
- Keperawatan Poli RajalDocument3 pagesKeperawatan Poli Rajalachmad subahtiarNo ratings yet
- Information Technology System Applicable in Nursing (Unit 3)Document6 pagesInformation Technology System Applicable in Nursing (Unit 3)jimuelmacamaNo ratings yet
- Skip To Main ContentDocument11 pagesSkip To Main ContentBudi YunantoNo ratings yet
- Cath Lab PlanningDocument2 pagesCath Lab PlanningHenry SuarezNo ratings yet
- Hemodialysis (Ipapaprint)Document2 pagesHemodialysis (Ipapaprint)John Paul Delos SantosNo ratings yet
- Cath Lab Operations MGMT PaperDocument14 pagesCath Lab Operations MGMT Paperah_zdn100% (1)
- Clinical Management System Project DocumDocument29 pagesClinical Management System Project DocumMelese SoratoNo ratings yet
- Computers in Health BY Group MDocument25 pagesComputers in Health BY Group MUsman Suleman Ahmad100% (1)
- Virtual Bio-Instrumentation: Jon B. Olansen, PH.DDocument42 pagesVirtual Bio-Instrumentation: Jon B. Olansen, PH.Dcata86_mailNo ratings yet
- Ni RevDocument12 pagesNi RevJaslir MendozaNo ratings yet
- Pharmacy Internship ReportDocument13 pagesPharmacy Internship ReportAmmar Ali73% (11)
- HOSPITAL DATABASE MANAGEMENT SYSTEMDocument11 pagesHOSPITAL DATABASE MANAGEMENT SYSTEMANKIT KUMARNo ratings yet
- Computer Science Advances HealthcareDocument13 pagesComputer Science Advances HealthcareUsman Suleman AhmadNo ratings yet
- Using Tracking Tools To Improve Patient Flow in Hospitals: Executive SummaryDocument21 pagesUsing Tracking Tools To Improve Patient Flow in Hospitals: Executive SummaryHughNo ratings yet
- Case StudyDocument10 pagesCase StudyMabalatan Renz CruzNo ratings yet
- Nursing InformaticsDocument32 pagesNursing InformaticsApril Maecy F. Dignomo100% (1)
- Operation Theatre ManagementDocument55 pagesOperation Theatre ManagementSushmitaBhaumik100% (73)
- Comparison of C4.5 Algorithm and Naïve Bayes For Last Information On ICU PatientsDocument7 pagesComparison of C4.5 Algorithm and Naïve Bayes For Last Information On ICU PatientsSumpena SuhandiNo ratings yet
- Hospital Database Management System SQL PDFDocument5 pagesHospital Database Management System SQL PDFRaoof Smko100% (1)
- RESEARCHDocument34 pagesRESEARCHBeiya MaeNo ratings yet
- Checklists For Central Sterile Supply Departments: CIS Self-Study Lesson PlanDocument5 pagesChecklists For Central Sterile Supply Departments: CIS Self-Study Lesson Planjerimiah_manzonNo ratings yet
- Veri ChipDocument33 pagesVeri ChipPraseetha RaoNo ratings yet
- Hospital Management SystemDocument39 pagesHospital Management SystemMeenahNo ratings yet
- Xcelera Brochure Updated (English)Document24 pagesXcelera Brochure Updated (English)Pablo Rosas100% (1)
- A Mobile-Based Patient-Centric Passive System For Guiding Patients Through The Hospital Workflow Desing and DevelopmentDocument19 pagesA Mobile-Based Patient-Centric Passive System For Guiding Patients Through The Hospital Workflow Desing and DevelopmentJuanse KrdenazNo ratings yet
- USG Gap AnalysisDocument37 pagesUSG Gap Analysispraveen maniNo ratings yet
- Radiomics Enabler An Etl ExtraDocument6 pagesRadiomics Enabler An Etl ExtraAshish Presanna ChandranNo ratings yet
- Operating RoomDocument8 pagesOperating Roomjonathan_tinsayNo ratings yet
- Journal of Biomedical Informatics: Jens Meier, Andreas Dietz, Andreas Boehm, Thomas NeumuthDocument12 pagesJournal of Biomedical Informatics: Jens Meier, Andreas Dietz, Andreas Boehm, Thomas NeumuthTanvin AyatNo ratings yet
- Final NI PaperDocument4 pagesFinal NI PaperMahmoud AliNo ratings yet
- Artificial Intelligence: in The ICUDocument5 pagesArtificial Intelligence: in The ICUGriyaNo ratings yet
- K J Somaiya Hospital & Research Centre: Job DescriptionDocument2 pagesK J Somaiya Hospital & Research Centre: Job DescriptionArpita MishraNo ratings yet
- Administration of A Radiological FacilityDocument92 pagesAdministration of A Radiological Facilitykyuleen05No ratings yet
- Invasive Cardiology LectureDocument49 pagesInvasive Cardiology LectureJibran Jones GarciaNo ratings yet
- Hospital Records Management SystemDocument7 pagesHospital Records Management SystemPrajwol GhemosuNo ratings yet
- Library DetailsDocument1 pageLibrary DetailsNasim AhmadNo ratings yet
- Front View: Material-Part-6&13 Caste Iron (Grade-Fg 260) Confirming To Is 210-1978Document1 pageFront View: Material-Part-6&13 Caste Iron (Grade-Fg 260) Confirming To Is 210-1978Nasim AhmadNo ratings yet
- Front View: Material-Part-6&13 Caste Iron (Grade-Fg 260) Confirming To Is 210-1978Document1 pageFront View: Material-Part-6&13 Caste Iron (Grade-Fg 260) Confirming To Is 210-1978Nasim AhmadNo ratings yet
- How Project Is UniqueDocument3 pagesHow Project Is UniqueNasim AhmadNo ratings yet
- Economic Considerations For Tall Multi-Use BuildingsDocument5 pagesEconomic Considerations For Tall Multi-Use BuildingsNasim AhmadNo ratings yet
- Building Services Design Requirements for All UsersDocument15 pagesBuilding Services Design Requirements for All UsersNasim AhmadNo ratings yet
- COST EFFECTIVE HIGH RISE BUILDING DESIGNDocument33 pagesCOST EFFECTIVE HIGH RISE BUILDING DESIGNNasim AhmadNo ratings yet
- Why Cnlu Is Coloured in Blue and Yellow: Class RommDocument2 pagesWhy Cnlu Is Coloured in Blue and Yellow: Class RommNasim AhmadNo ratings yet
- Photoshop 7 User Manual - 11pág.Document11 pagesPhotoshop 7 User Manual - 11pág.futurista666No ratings yet
- Burj Khalifa - The World's Most Expensive Buildings - TravelDocument13 pagesBurj Khalifa - The World's Most Expensive Buildings - TravelNasim AhmadNo ratings yet
- Annexure: I Norms and RequirementsDocument10 pagesAnnexure: I Norms and Requirementssivakumark1290No ratings yet
- Presentation 3Document2 pagesPresentation 3Nasim AhmadNo ratings yet
- Shopping Mall Literature StudyDocument27 pagesShopping Mall Literature StudyNasim AhmadNo ratings yet
- Gandhinagar Capital of GujaratDocument6 pagesGandhinagar Capital of GujaratNasim AhmadNo ratings yet
- Nid PresentationDocument8 pagesNid PresentationNasim AhmadNo ratings yet
- Shopping MallsDocument28 pagesShopping MallsNasim AhmadNo ratings yet
- Pacific Mall Case StudyDocument24 pagesPacific Mall Case StudyAyushi Rishi Rai89% (9)
- ClimateDocument3 pagesClimateNasim AhmadNo ratings yet
- Floor Plans@ KHERIA-ModelDocument1 pageFloor Plans@ KHERIA-ModelNasim AhmadNo ratings yet
- For Case Study Sheet FormateDocument2 pagesFor Case Study Sheet FormateNasim AhmadNo ratings yet
- Space Planning Critical Design Features in Healthcare ProjectsDocument38 pagesSpace Planning Critical Design Features in Healthcare ProjectsVinoth KumarNo ratings yet
- Grid Plan 7.3.18 For Tabin-Model - PDF BurDocument1 pageGrid Plan 7.3.18 For Tabin-Model - PDF BurNasim AhmadNo ratings yet
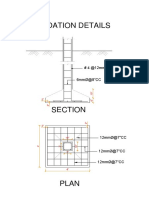
- Foundation Details PDFDocument1 pageFoundation Details PDFNasim AhmadNo ratings yet
- For Case Study Sheet FormateDocument2 pagesFor Case Study Sheet FormateNasim AhmadNo ratings yet
- Urban Design PrinciplesDocument53 pagesUrban Design PrinciplesNasim AhmadNo ratings yet
- Railway Station Design (B.arch Thesis)Document9 pagesRailway Station Design (B.arch Thesis)Nasim Ahmad43% (7)
- Microsoft Word - Building Bye Laws English Final 29.11.2013Document1 pageMicrosoft Word - Building Bye Laws English Final 29.11.2013Nasim AhmadNo ratings yet
- Viraat Ramayan Mandir, Near Kesaria, BiharDocument3 pagesViraat Ramayan Mandir, Near Kesaria, BiharNasim AhmadNo ratings yet
- Opeman MIDTERM 2Document2 pagesOpeman MIDTERM 2Michelle Ann WongNo ratings yet
- HyperthyroidismDocument6 pagesHyperthyroidismNader Smadi100% (2)
- Nasterea in Prezentatie PelvinaDocument14 pagesNasterea in Prezentatie PelvinaIrina AdrianaNo ratings yet
- Manu Chopra MD, DNB, Mnams PulmonologistDocument95 pagesManu Chopra MD, DNB, Mnams PulmonologistJaya Semara PutraNo ratings yet
- Discover Our Gastroenterology Senior Residency ProgrammeDocument3 pagesDiscover Our Gastroenterology Senior Residency Programmegus_lionsNo ratings yet
- The Unofficial Clinical Clerkship Survival Guide: LouisvilleDocument65 pagesThe Unofficial Clinical Clerkship Survival Guide: LouisvilleAffan HaqNo ratings yet
- Work Immersion Experience at Mindanao Doctors Hospital and Cancer Center LaboratoryDocument12 pagesWork Immersion Experience at Mindanao Doctors Hospital and Cancer Center LaboratoryAngel RamosNo ratings yet
- Heparin Induced ThrombocytopeniaDocument29 pagesHeparin Induced Thrombocytopeniahari krishna100% (6)
- Ampicillin/sulbactamDocument0 pagesAmpicillin/sulbactamputri_agustina_1No ratings yet
- Clinical Trial Published in The International Journal of Oral Maxillofacial Implants Demonstrates Less Pain and Higher Quality Bone With Snoasis Medical's BioXclude®Document3 pagesClinical Trial Published in The International Journal of Oral Maxillofacial Implants Demonstrates Less Pain and Higher Quality Bone With Snoasis Medical's BioXclude®PR.comNo ratings yet
- SAP HaluDocument6 pagesSAP HaluFarhan HerjantoNo ratings yet
- Peripheral Arterial Disease of The Lower ExtremitiesDocument25 pagesPeripheral Arterial Disease of The Lower Extremitiesapi-3697326100% (1)
- 8 Dimensions Picker InstitusiDocument2 pages8 Dimensions Picker Institusiinggar ratnakusumaNo ratings yet
- Intravenous Lidocaine in The Treatment of Refractory Headache A Retrospective Case Series.Document6 pagesIntravenous Lidocaine in The Treatment of Refractory Headache A Retrospective Case Series.Jordan WardNo ratings yet
- Hospital Thesis Preparatory GAURAVDocument22 pagesHospital Thesis Preparatory GAURAVGaurav Jain100% (3)
- Audit Discharge SummaryDocument15 pagesAudit Discharge SummaryDrKarnav PanchalNo ratings yet
- CACVS2016 AbstractBookDocument100 pagesCACVS2016 AbstractBookChuk IfeanyiNo ratings yet
- Transplantation ImmunologyDocument69 pagesTransplantation Immunologytummalapalli venkateswara rao100% (1)
- Inservice PresentationDocument13 pagesInservice Presentationapi-467829418No ratings yet
- Guide BLS + SkenarioDocument4 pagesGuide BLS + Skenariofatimah putriNo ratings yet
- Rowena R. Marasigan BSN, RNDocument3 pagesRowena R. Marasigan BSN, RNAMINAH JULIANNA MARASIGANNo ratings yet
- U1 Matter - The Baby and The Bottle - Making A Case Project Details and RubricDocument4 pagesU1 Matter - The Baby and The Bottle - Making A Case Project Details and RubricKAELYN CARNAKONo ratings yet
- FLASHCARD CardiovascularDocument40 pagesFLASHCARD CardiovascularsnehaNo ratings yet
- MRI Scanning and OrthodonticsDocument7 pagesMRI Scanning and OrthodonticsAmit SagarNo ratings yet
- Anaesthesia For Trauma PatientsDocument5 pagesAnaesthesia For Trauma Patientscahya candraNo ratings yet
- History of Herbal TritmentDocument10 pagesHistory of Herbal TritmentTorentSpyNo ratings yet
- Effects of Implementation of Focus-Pdca Model OnDocument14 pagesEffects of Implementation of Focus-Pdca Model OnSofiyullohNo ratings yet
- Orthodontics I/Ii/Iii: Goals: This Series of Seminars Should Enable The Resident ToDocument9 pagesOrthodontics I/Ii/Iii: Goals: This Series of Seminars Should Enable The Resident Todruzair007No ratings yet
- Application of Alfred Adler Individual PsychologyDocument6 pagesApplication of Alfred Adler Individual PsychologyArian FerrerNo ratings yet
- Dental Plans and Rates: Bay AreaDocument6 pagesDental Plans and Rates: Bay AreaJDanaNo ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (17)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (403)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- 12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosFrom Everand12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosRating: 4.5 out of 5 stars4.5/5 (207)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Algorithms to Live By: The Computer Science of Human DecisionsFrom EverandAlgorithms to Live By: The Computer Science of Human DecisionsRating: 4.5 out of 5 stars4.5/5 (722)
- Summary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (11)
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)