You might also like
- Operating Manual: Tubing TongDocument290 pagesOperating Manual: Tubing Tongwuillian barretoNo ratings yet
- Chain Block InspectionDocument1 pageChain Block InspectionMochammad AriefNo ratings yet
- Deviation Approval FORMDocument4 pagesDeviation Approval FORMFatimahAhmatNo ratings yet
- Liquid Penetrant Examination Report: PO No.&Document2 pagesLiquid Penetrant Examination Report: PO No.&Samir Chaudhary100% (2)
- Form-I-010 Welding Machine Inspection Form: Carry-In CertificateDocument1 pageForm-I-010 Welding Machine Inspection Form: Carry-In CertificateAdhy DarmawanNo ratings yet
- Service Manual Trucks: Circuit and Wiring Numbers VN, VHDDocument34 pagesService Manual Trucks: Circuit and Wiring Numbers VN, VHDАндрейNo ratings yet
- Crane Inspection FormDocument2 pagesCrane Inspection FormWisnu Suryo Andriyanto AndriyantoNo ratings yet
- Crane InspectionDocument2 pagesCrane InspectionAdhy DarmawanNo ratings yet
- Branch Circuit ComputationDocument9 pagesBranch Circuit ComputationLester Musca100% (1)
- Doha Expressway Pipe Laying InspectionDocument1 pageDoha Expressway Pipe Laying InspectionraghebomNo ratings yet
- ACMV Inspeciton Check ListDocument22 pagesACMV Inspeciton Check ListNaing Win TunNo ratings yet
- INCR New Format 2021Document1 pageINCR New Format 2021Khan ZamanNo ratings yet
- Project Name:-: Inspection Test Plan (ITP)Document6 pagesProject Name:-: Inspection Test Plan (ITP)TchoboNo ratings yet
- Project Eagle: Quality Management Inspection ReportDocument2 pagesProject Eagle: Quality Management Inspection ReportrcpretoriusNo ratings yet
- A Contractor's Guide to the FIDIC Conditions of ContractFrom EverandA Contractor's Guide to the FIDIC Conditions of ContractNo ratings yet
- Computerized Lensmeter: Instruction ManualDocument29 pagesComputerized Lensmeter: Instruction ManualRitesh Gupta100% (1)
- Crane InspectionDocument2 pagesCrane InspectionAdhy DarmawanNo ratings yet
- Smart BoomDocument10 pagesSmart BoomKevine Khaled100% (1)
- Check List For Installation of Cooling TowersDocument2 pagesCheck List For Installation of Cooling TowersGirithar M Sundaram67% (3)
- Qa QC Inspection ReportDocument1 pageQa QC Inspection ReportUbaidullah KhanNo ratings yet
- Subcontractor Document Review Risk AssessmentDocument24 pagesSubcontractor Document Review Risk Assessmentrodman823No ratings yet
- Im-Co-Fo-88 Summary Inspection Report of The Rig PTX 15 - Mar - 1Document33 pagesIm-Co-Fo-88 Summary Inspection Report of The Rig PTX 15 - Mar - 1JUAN JOSE VESGA RUEDA100% (1)
- By Akhilesh CHECKLIST - For AllDocument15 pagesBy Akhilesh CHECKLIST - For AllankurNo ratings yet
- DRP001-OUF-GAL-PRO-Q-000-067 Rev-S1Document61 pagesDRP001-OUF-GAL-PRO-Q-000-067 Rev-S1Rafat KhanNo ratings yet
- Material Traceability Inspection ReportDocument32 pagesMaterial Traceability Inspection ReportBalmiki SinghNo ratings yet
- BMJV-QUA-F18.01 Excavation Checklist R00Document1 pageBMJV-QUA-F18.01 Excavation Checklist R00Taiwo OshinNo ratings yet
- S-000-1679-0001V Itp For Insulation PDFDocument5 pagesS-000-1679-0001V Itp For Insulation PDFPhuoc PhuNo ratings yet
- Synthetics Rubber Indonesia Pile InspectionDocument2 pagesSynthetics Rubber Indonesia Pile InspectionDenny SyafwalufiNo ratings yet
- Form 02 Crane Inspection FormDocument2 pagesForm 02 Crane Inspection FormDenny SyafwalufiNo ratings yet
- Form 16 Light VehicleDocument2 pagesForm 16 Light VehicleDenny SyafwalufiNo ratings yet
- Form 01 Crane Carry in InspectionDocument3 pagesForm 01 Crane Carry in InspectionDenny Syafwalufi0% (1)
- Soil Handling Equipment InspectionDocument2 pagesSoil Handling Equipment InspectionAdhy DarmawanNo ratings yet
- Pile Driving Machine InspectionDocument2 pagesPile Driving Machine InspectionAdhy Darmawan100% (1)
- Form Inspection Premob - Quarterly (1) - 2Document26 pagesForm Inspection Premob - Quarterly (1) - 2Ryan RhamdhaniNo ratings yet
- PDFDocument3 pagesPDFnate anantathatNo ratings yet
- Task Risk Assessment for Emergency RepairsDocument16 pagesTask Risk Assessment for Emergency Repairsrodman823No ratings yet
- Installation of Irrigation System ITPDocument2 pagesInstallation of Irrigation System ITPBleep NewsNo ratings yet
- Diesel Tanker Inspection ChecklistDocument2 pagesDiesel Tanker Inspection ChecklistNisar DeenNo ratings yet
- Slawinski Datasheet enDocument10 pagesSlawinski Datasheet enahmed mohamedNo ratings yet
- 7 PDF - 1 - 2781 NCR TEP JHS 001 - 05sep18Document1 page7 PDF - 1 - 2781 NCR TEP JHS 001 - 05sep18Victor ManaoNo ratings yet
- Pt. Sispum Sarana GrahaDocument2 pagesPt. Sispum Sarana GrahaMochammad AriefNo ratings yet
- D6255-SIR FormatDocument4 pagesD6255-SIR Formatnisha_khanNo ratings yet
- 1340 Hse FRM - 16 Crane Safety ChecklistDocument1 page1340 Hse FRM - 16 Crane Safety Checklistvenkateshr.193No ratings yet
- RFI-Form Updated 3.07.2018.......Document6 pagesRFI-Form Updated 3.07.2018.......nate anantathatNo ratings yet
- Ohs-Pr-09-19-F14 (A) Mancage Register & InspectionDocument3 pagesOhs-Pr-09-19-F14 (A) Mancage Register & InspectionShafie ZubierNo ratings yet
- INCR-Pouring Without Inspection - Girls SchoolDocument1 pageINCR-Pouring Without Inspection - Girls SchoolusmanNo ratings yet
- Lorry Boom PlacerDocument2 pagesLorry Boom PlacerBakri Bin SapilahNo ratings yet
- SA048-WSP-GEN-MTS-MNCR-2 Non-Conformance Report - Tested Stockpile BarricationDocument2 pagesSA048-WSP-GEN-MTS-MNCR-2 Non-Conformance Report - Tested Stockpile BarricationmustafaansmeNo ratings yet
- Itr-Msa (Air Cooler)Document13 pagesItr-Msa (Air Cooler)mahmoudNo ratings yet
- Breaker Driving Machine InspectionDocument2 pagesBreaker Driving Machine InspectionMochammad AriefNo ratings yet
- Drill Machine ChecklistDocument2 pagesDrill Machine ChecklistTejas SarodeNo ratings yet
- Subcontractor TRA for Night Shift WorkDocument26 pagesSubcontractor TRA for Night Shift Workrodman823No ratings yet
- Supplier Inspection Report for Aramco Metering Systems UpgradeDocument4 pagesSupplier Inspection Report for Aramco Metering Systems Upgradenisha_khanNo ratings yet
- الأسرة وتربية الطفل ، الدكتورة هدى محمود الناشفDocument1 pageالأسرة وتربية الطفل ، الدكتورة هدى محمود الناشفanon_545606833No ratings yet
- P-0008-01 installation of Above Ground Water Supply PipingDocument1 pageP-0008-01 installation of Above Ground Water Supply PipinghassanabunafeesahNo ratings yet
- Contract Review FormDocument2 pagesContract Review Formsunday babalolaNo ratings yet
- QS049-P04-ASH-GEN-GEN-IR-28624 R0-SignedDocument6 pagesQS049-P04-ASH-GEN-GEN-IR-28624 R0-SignedMa NadeemNo ratings yet
- M-0043-01-CL - Installation of Above GroundDocument1 pageM-0043-01-CL - Installation of Above GroundhassanabunafeesahNo ratings yet
- Pt. Rekayasa Industri: Engineering & ConstructionDocument5 pagesPt. Rekayasa Industri: Engineering & ConstructionandhyirawanNo ratings yet
- Non-Conformity Report: Date NCR No.: Sheet: 1/1 Client: Project: Job No: ItemDocument2 pagesNon-Conformity Report: Date NCR No.: Sheet: 1/1 Client: Project: Job No: ItemKhaled GamalNo ratings yet
- Materials Inspection RequestDocument1 pageMaterials Inspection RequestMaina MathengeNo ratings yet
- Inspection Report: Report of Final Inspection Intermediate / Progress Inspection Report Number QETO/VFL/JSPL/SUD/00194Document2 pagesInspection Report: Report of Final Inspection Intermediate / Progress Inspection Report Number QETO/VFL/JSPL/SUD/00194sudipta dasNo ratings yet
- MS For Leak Test in ManholesDocument7 pagesMS For Leak Test in ManholesMadhavMitruNo ratings yet
- Parts List for Motorcycle ComponentsDocument45 pagesParts List for Motorcycle ComponentsR SuMmOnNo ratings yet
- Mitsubishi Electric PUHZ-SHW80-140 Service Manual EngDocument136 pagesMitsubishi Electric PUHZ-SHW80-140 Service Manual EngSERVI-TODO JR Ricardo herreraNo ratings yet
- 1 Get Prod Catalogue Full June2009Document178 pages1 Get Prod Catalogue Full June2009adirajjNo ratings yet
- Electric Pump and Bracket AccessoriesDocument14 pagesElectric Pump and Bracket AccessoriesEdison GonsalvesNo ratings yet
- TL105 Test Lamp Manual For Optical Flame DetectorsDocument1 pageTL105 Test Lamp Manual For Optical Flame DetectorsArnulfo SanchezNo ratings yet
- LFK95 LeafletDocument4 pagesLFK95 LeafletKhalid MahmoodNo ratings yet
- Hyd System - Part 1 Single Lift Pump ( - A - Batt. Comp.) (25,1.0,35,1.6, RR) (02.0-14.0-005)Document6 pagesHyd System - Part 1 Single Lift Pump ( - A - Batt. Comp.) (25,1.0,35,1.6, RR) (02.0-14.0-005)rorroscNo ratings yet
- Electera NEE 43 44Document62 pagesElectera NEE 43 44MTK2016No ratings yet
- HYGOOD SAPPHIRE With Z 10 and Lithium IonDocument14 pagesHYGOOD SAPPHIRE With Z 10 and Lithium IonMarcio BritoNo ratings yet
- Gfps Us Catalog Contain It Secondary Containment enDocument23 pagesGfps Us Catalog Contain It Secondary Containment enFrancesco GarieriNo ratings yet
- DRL Master: SEO-Optimized Title for Daytime Running Lamp DocumentDocument7 pagesDRL Master: SEO-Optimized Title for Daytime Running Lamp DocumentIván Colomino ValverdeNo ratings yet
- Floor Standing Enclosures Multicompact - MT: AccessoriesDocument1 pageFloor Standing Enclosures Multicompact - MT: AccessoriesAdel AdelNo ratings yet
- Aprilaire Stat 3041 - InstallDocument28 pagesAprilaire Stat 3041 - InstallRetro SeasonsNo ratings yet
- 7720120191pl IntralogicDocument206 pages7720120191pl IntralogicSayeed AnwarNo ratings yet
- TM9 2920 242 35Document110 pagesTM9 2920 242 35Rulax MtzNo ratings yet
- KWK Data Sheet 2021 02Document7 pagesKWK Data Sheet 2021 02Anas RaisNo ratings yet
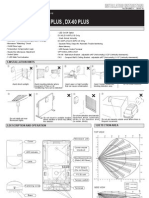
- DX-40, DX-60, DX-40 PLUS, DX-60 PLUS: FeaturesDocument4 pagesDX-40, DX-60, DX-40 PLUS, DX-60 PLUS: FeaturesIulia GvrNo ratings yet
- DC Current Transducer CTG: Features / ApplicationsDocument1 pageDC Current Transducer CTG: Features / ApplicationsLê Nhi ThảoNo ratings yet
- Work permit safety checklistDocument2 pagesWork permit safety checklistNilamSanjeev Kumar SinghNo ratings yet
- Line Boring ToolsDocument8 pagesLine Boring ToolsMalik Uddin ZahirNo ratings yet
- COMBI 350 Sawing Machine Operating ManualDocument9 pagesCOMBI 350 Sawing Machine Operating ManualDein MasterNo ratings yet
- Discipline Build GuideDocument11 pagesDiscipline Build Guidealmanet666No ratings yet
- eTORK Digital Wrench InstructionsDocument8 pageseTORK Digital Wrench InstructionsJHON FREDY PEREZ ZAMUDIONo ratings yet
- Spare Parts Guide for INVERTEC 135S, 150S & 170S MachinesDocument7 pagesSpare Parts Guide for INVERTEC 135S, 150S & 170S MachinesDiegoNo ratings yet
- LG Therma V AWHP R32 Monobloc PDB (Jan 2019)Document49 pagesLG Therma V AWHP R32 Monobloc PDB (Jan 2019)kirooNo ratings yet