You might also like
- MR Loveday Little Outing Day AnalysisDocument4 pagesMR Loveday Little Outing Day AnalysisLorenaGeninSantaCruz40% (10)
- Lung - PathologyDocument34 pagesLung - Pathologyjmosser100% (3)
- Checklist For Local Anesthetic Toxicity Treatment 1-18-12Document2 pagesChecklist For Local Anesthetic Toxicity Treatment 1-18-12Akilesh RamasamyNo ratings yet
- Cardiovascular Pathology - 025) Valvular Heart Diseases Overview (Notes)Document18 pagesCardiovascular Pathology - 025) Valvular Heart Diseases Overview (Notes)Geraldine HernandezNo ratings yet
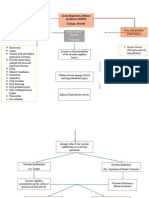
- Non-Modifiable Risk Factor Modifiable Risk Factors: Acute Respiratory Distress Syndrome (ARDS) (Lungs Alveoli)Document3 pagesNon-Modifiable Risk Factor Modifiable Risk Factors: Acute Respiratory Distress Syndrome (ARDS) (Lungs Alveoli)joyrena ochondraNo ratings yet
- Ards PDFDocument20 pagesArds PDFRuki HartawanNo ratings yet
- Acute/Adulth Respiratory Distress Syndrome (ARDS) : RohmanDocument54 pagesAcute/Adulth Respiratory Distress Syndrome (ARDS) : RohmanMuhammad Rizki Junaidi SaputraNo ratings yet
- 1.04 GEN PATH LAB REALLS-Fluid and Hemodynamics UEDocument5 pages1.04 GEN PATH LAB REALLS-Fluid and Hemodynamics UEAllysa Marie CotandaNo ratings yet
- Pollution - Solved-Examples Solved-ExampleDocument6 pagesPollution - Solved-Examples Solved-ExampleBharati GulajkarNo ratings yet
- Covid and Ebola MsDocument7 pagesCovid and Ebola MsAimee Rochelle MaesaNo ratings yet
- 2 Respiratory Medicine: Streptococcus Pneumoniae Klebsiella Pneumoniae Legionella Pneumophila Mycoplasma PneumoniaeDocument24 pages2 Respiratory Medicine: Streptococcus Pneumoniae Klebsiella Pneumoniae Legionella Pneumophila Mycoplasma Pneumoniaesultan khabeeb100% (1)
- Respiratory-Renal Block, Practical IDocument37 pagesRespiratory-Renal Block, Practical Imina mounirNo ratings yet
- A Tricompartmental Model of Lung Oxygenation Disruption To Explain Pulmonary and Systemic Pathology in Severe COVID-19Document8 pagesA Tricompartmental Model of Lung Oxygenation Disruption To Explain Pulmonary and Systemic Pathology in Severe COVID-19alvaro millanNo ratings yet
- Path Lung McqsDocument24 pagesPath Lung McqsShafaque IrfanNo ratings yet
- Doxycycline: From Ocular Rosacea To COVID-19 Anosmia. New Insight Into The Coronavirus OutbreakDocument4 pagesDoxycycline: From Ocular Rosacea To COVID-19 Anosmia. New Insight Into The Coronavirus OutbreakAndhi Riawan Eko WiikramatunggadewaNo ratings yet
- Chronic Obstructive Pulmonary Disease: Iman Galal, MDDocument60 pagesChronic Obstructive Pulmonary Disease: Iman Galal, MDYan Sheng HoNo ratings yet
- Covid Fisiopato InglesDocument8 pagesCovid Fisiopato InglesaarongondraNo ratings yet
- Answer: CHAPTER 1 Stimuli and ResponsesDocument8 pagesAnswer: CHAPTER 1 Stimuli and Responses林柄洲No ratings yet
- Endothelial Dysfunction in COVID-19 Potential Mechanisms and Possible Therapeutic OptionsDocument24 pagesEndothelial Dysfunction in COVID-19 Potential Mechanisms and Possible Therapeutic OptionssamuelNo ratings yet
- Lobar Pneumonia: Deevon M. Cariaga FEU-NRMF Institute of MedicineDocument12 pagesLobar Pneumonia: Deevon M. Cariaga FEU-NRMF Institute of MedicinedeevoncNo ratings yet
- Pathophysiology of COVID19: Deekshya Devkota 8025Document2 pagesPathophysiology of COVID19: Deekshya Devkota 8025Deekshya DevkotaNo ratings yet
- Coomon Diseases & DescriptionsDocument1 pageCoomon Diseases & Descriptionsdheeraj kumarNo ratings yet
- Test 7 XI - Unit5Document9 pagesTest 7 XI - Unit5Tamal NayakNo ratings yet
- Neet Class 11 Morning Batch 1705736322Document15 pagesNeet Class 11 Morning Batch 1705736322thetom1245No ratings yet
- UntitledDocument34 pagesUntitledDr.younes95 RekaaneyNo ratings yet
- Hnizdo 2003Document8 pagesHnizdo 2003Dang QuanNo ratings yet
- Pneumonia Parient BasedDocument2 pagesPneumonia Parient BasedKismet SummonsNo ratings yet
- Articulo Fisiopatologia de La Enfermedad 2Document5 pagesArticulo Fisiopatologia de La Enfermedad 2ivanNo ratings yet
- ICU Department ICU DepartmentDocument48 pagesICU Department ICU DepartmentEmad ElhusseinNo ratings yet
- Diseases MSDocument6 pagesDiseases MSKajolNo ratings yet
- Emergency Radiologic Approach To Sinus Disease: Matthew R. Mccann Alexander T. Kessler Alok A. BhattDocument8 pagesEmergency Radiologic Approach To Sinus Disease: Matthew R. Mccann Alexander T. Kessler Alok A. BhattVidya PasaribuNo ratings yet
- Pulmonary Immuno-Thrombosis in COVID-19 ARDS PathogenesisDocument4 pagesPulmonary Immuno-Thrombosis in COVID-19 ARDS PathogenesisXavier AbrilNo ratings yet
- Subcutaneous Emphysema Complicated by COVID-19 Infection Case Report and Literature ReviewDocument3 pagesSubcutaneous Emphysema Complicated by COVID-19 Infection Case Report and Literature ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Supplemental Chapter 2 Intersitial Lung Disease: A Picture BookDocument13 pagesSupplemental Chapter 2 Intersitial Lung Disease: A Picture Bookpablo carednasNo ratings yet
- 5 THDocument6 pages5 THArnav GuptaNo ratings yet
- Interstitial Lung DiseaseDocument66 pagesInterstitial Lung DiseaseGrant Wynn ArnucoNo ratings yet
- FC Rad Diag (SA) Part II Past Papers - 2021 1st Semester 30 11 2022Document4 pagesFC Rad Diag (SA) Part II Past Papers - 2021 1st Semester 30 11 2022asdsaNo ratings yet
- Acute Respiratory Distress Syndrome by Mr. Ashish RoyDocument45 pagesAcute Respiratory Distress Syndrome by Mr. Ashish RoySyedzulqurnainhussainshah ZulqurnainNo ratings yet
- Assignmnet 2 Soltn - ESC 202Document4 pagesAssignmnet 2 Soltn - ESC 202Nidhi MalikNo ratings yet
- Y11 Biology Mock Exam Questions and MS-RRRDocument75 pagesY11 Biology Mock Exam Questions and MS-RRRsaeedshahidNo ratings yet
- Atrial Fibrillation AtfDocument11 pagesAtrial Fibrillation AtfChristine MagnoNo ratings yet
- Norma, PathoDocument3 pagesNorma, PathoHazelyn CayleNo ratings yet
- Atelectasis: Contraction Atelectasis (Or Cicatrization Atelectasis)Document10 pagesAtelectasis: Contraction Atelectasis (Or Cicatrization Atelectasis)Gan BangNo ratings yet
- 0052 - Kadek Diana Susilawati - LP Luka BakarDocument11 pages0052 - Kadek Diana Susilawati - LP Luka BakarDiana IdNo ratings yet
- Cell Injury Electronic or Printed Copies of These Slides!!: Pathology I ImagesDocument20 pagesCell Injury Electronic or Printed Copies of These Slides!!: Pathology I ImagesMiile EstrellitaaNo ratings yet
- Necropsy of The Pig - EoDocument6 pagesNecropsy of The Pig - EoMaverick LastimosaNo ratings yet
- Chapter13 and 14 HeiDocument90 pagesChapter13 and 14 HeiAyieMz Iverson SolisNo ratings yet
- The Pathology of Lung Diseases: I. Restrictive Lung Diseas ESDocument65 pagesThe Pathology of Lung Diseases: I. Restrictive Lung Diseas ESLiana Ika SuwandyNo ratings yet
- Amy and Kisham: Worksheets AnswersDocument8 pagesAmy and Kisham: Worksheets AnswersAnas Ahmed MamdouhNo ratings yet
- XII - Biology - Module - 5 - Environmental Issues - SolutionsDocument17 pagesXII - Biology - Module - 5 - Environmental Issues - SolutionsShreyashNo ratings yet
- COVID-19: Hemoglobin, Iron, and Hypoxia Beyond Inflammation. A Narrative ReviewDocument7 pagesCOVID-19: Hemoglobin, Iron, and Hypoxia Beyond Inflammation. A Narrative ReviewAlejandroNo ratings yet
- Module 4Document34 pagesModule 4xtnreyesNo ratings yet
- Jurnal ARDSDocument17 pagesJurnal ARDSwahyuNo ratings yet
- Pulmonary EmbolismDocument12 pagesPulmonary EmbolismJohn Paul MatienzoNo ratings yet
- Cardiovascular Pathology - 020) Aortic Valve Stenosis and Regurgitation (Notes)Document13 pagesCardiovascular Pathology - 020) Aortic Valve Stenosis and Regurgitation (Notes)arga setyo adjiNo ratings yet
- 1082 Medical Surgical Nursing Eye & Ent & Integumentary System DDocument16 pages1082 Medical Surgical Nursing Eye & Ent & Integumentary System DdhavalsagthiaaNo ratings yet
- CCR Landoni120 June v6-2Document3 pagesCCR Landoni120 June v6-2Rara AuliaNo ratings yet
- Pangpangdeo Shanne Delle B. - Worksheet 5 ArdsDocument7 pagesPangpangdeo Shanne Delle B. - Worksheet 5 ArdsPANGPANGDEO Shanne Delle B.No ratings yet
- 07-Pollution of Air & WaterDocument3 pages07-Pollution of Air & WatervarshavishuNo ratings yet
- Assignmnet 2 Ques - ESC 202Document4 pagesAssignmnet 2 Ques - ESC 202Nidhi MalikNo ratings yet
- 粉尘与尘肺Document59 pages粉尘与尘肺api-3735745No ratings yet
- 246 - Respiratory Pathology Pneumonia - Treatment and PreventionDocument4 pages246 - Respiratory Pathology Pneumonia - Treatment and PreventionPranav PunjabiNo ratings yet
- 243 - Respiratory Pathology COPD - Treatment and PreventionDocument3 pages243 - Respiratory Pathology COPD - Treatment and PreventionPranav PunjabiNo ratings yet
- Renal Pathology Acute Kidney Injury AKIDocument14 pagesRenal Pathology Acute Kidney Injury AKIPranav PunjabiNo ratings yet
- 242 - Respiratory Pathology COPD - Clinical FeaturesDocument3 pages242 - Respiratory Pathology COPD - Clinical FeaturesPranav PunjabiNo ratings yet
- Barth BulimiaDocument13 pagesBarth BulimiaFernando Mišel PessoaNo ratings yet
- Langley-Evans-2015-Journal of Human Nutrition and Dietetics PDFDocument14 pagesLangley-Evans-2015-Journal of Human Nutrition and Dietetics PDFPriscila Lemasson DuranteNo ratings yet
- Role Play PDFDocument18 pagesRole Play PDFTin TinNo ratings yet
- Cdmp2015 HandbookDocument90 pagesCdmp2015 HandbookTony NgNo ratings yet
- Insignis PCM3 Dengue, Blood Donation, HIV, Mental Health, NBS, LeprosyDocument133 pagesInsignis PCM3 Dengue, Blood Donation, HIV, Mental Health, NBS, LeprosyNibshian Dela RosaNo ratings yet
- Contraindications To Air TravelDocument15 pagesContraindications To Air TravelsDamnNo ratings yet
- Hypertension JDHHDDDocument5 pagesHypertension JDHHDDabcxyz15021999No ratings yet
- Drug Study Lab, NCP - Bronchial AsthmaDocument6 pagesDrug Study Lab, NCP - Bronchial AsthmaRichelle Sandriel C. de CastroNo ratings yet
- Denagard Amoxicillin MICs For Respiratory PathogensDocument2 pagesDenagard Amoxicillin MICs For Respiratory Pathogensnick224No ratings yet
- Nurture and ConnectionDocument4 pagesNurture and Connectionparents021100% (1)
- Mobic 15 MG Tablets - Summary of Product Characteristics (SPC)Document11 pagesMobic 15 MG Tablets - Summary of Product Characteristics (SPC)zxvcazcf0% (1)
- Diagnostic Value of Non Invasive Liver Function Tests in Liver Fibrosis and Changes in These Parameters Post Metabolic SurgeryDocument7 pagesDiagnostic Value of Non Invasive Liver Function Tests in Liver Fibrosis and Changes in These Parameters Post Metabolic SurgeryTan BulNo ratings yet
- Bells PalsyDocument66 pagesBells PalsyanshikaNo ratings yet
- Early Onset SchizophreniaDocument3 pagesEarly Onset SchizophreniaDoc Prince CaballeroNo ratings yet
- Nursing Care PlanDocument1 pageNursing Care Planapi-248135371No ratings yet
- Parathyroid Glands: Serum PTH Levels Are Inappropriately Elevated For The LevelDocument4 pagesParathyroid Glands: Serum PTH Levels Are Inappropriately Elevated For The LevelNada MuchNo ratings yet
- Forgein Bodies PPDDocument22 pagesForgein Bodies PPDVishuNo ratings yet
- Case Study 5 Year Boy With CoughDocument3 pagesCase Study 5 Year Boy With CoughAryl Eduarte100% (1)
- Title: HypoglycemiaDocument13 pagesTitle: Hypoglycemia025 MUHAMAD HAZIQ BIN AHMAD AZMANNo ratings yet
- Recurrent Pregnancy LossDocument18 pagesRecurrent Pregnancy LossNap91No ratings yet
- Mr. Jones Case StudyDocument4 pagesMr. Jones Case StudyDiane JaravataNo ratings yet
- A Critique PaperDocument1 pageA Critique PaperAyessa Nedine SalazarNo ratings yet
- 1-Normality and Mental HealthDocument7 pages1-Normality and Mental HealthRoland GealonNo ratings yet
- Getweightloss in Intragastric BalloonDocument2 pagesGetweightloss in Intragastric Balloongetweightloss2023No ratings yet
- AR para ManosDocument22 pagesAR para ManosAndres CasteloNo ratings yet
- Diarrhea: On This PageDocument6 pagesDiarrhea: On This PageKristine AlejandroNo ratings yet
- Cards RQs For INDEBDocument38 pagesCards RQs For INDEBJanderson LeiteNo ratings yet
- Algorithm For Anemia in Children Based On MCV - UpToDateDocument2 pagesAlgorithm For Anemia in Children Based On MCV - UpToDatefabsscribdworksNo ratings yet