You might also like
- Chapter 33.3 WorksheetDocument4 pagesChapter 33.3 WorksheetMING ZHU0% (1)
- Lung - PathologyDocument34 pagesLung - Pathologyjmosser100% (3)
- Atelectasis: Contraction Atelectasis (Or Cicatrization Atelectasis)Document10 pagesAtelectasis: Contraction Atelectasis (Or Cicatrization Atelectasis)Gan BangNo ratings yet
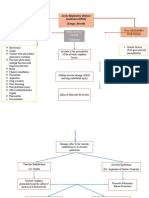
- Non-Modifiable Risk Factor Modifiable Risk Factors: Acute Respiratory Distress Syndrome (ARDS) (Lungs Alveoli)Document3 pagesNon-Modifiable Risk Factor Modifiable Risk Factors: Acute Respiratory Distress Syndrome (ARDS) (Lungs Alveoli)joyrena ochondraNo ratings yet
- Acute Respiratory Distress SyndromeDocument9 pagesAcute Respiratory Distress SyndromeAgnes Jeane EnriquezNo ratings yet
- Ncma113 Finals-ReviewerDocument84 pagesNcma113 Finals-ReviewerYu AnNo ratings yet
- Legionella Pneumophilia PaperDocument13 pagesLegionella Pneumophilia PaperCliff TorrenceNo ratings yet
- Ncma113 Finals-ReviewerDocument53 pagesNcma113 Finals-ReviewerAB AlmazoraNo ratings yet
- Respiratory MS NOTESDocument15 pagesRespiratory MS NOTESMARY ANN CAGATANNo ratings yet
- 118 Ards NotesDocument3 pages118 Ards Notescabelin randy amenNo ratings yet
- Conference Proceedings: Physiology of Airway Mucus Secretion and Pathophysiology of HypersecretionDocument16 pagesConference Proceedings: Physiology of Airway Mucus Secretion and Pathophysiology of HypersecretionFadhiil Asyarullah MurtadhoNo ratings yet
- Dafpus Baru 5Document11 pagesDafpus Baru 5stanleyNo ratings yet
- Lesson 2 Acute Respiratory Distress Syndrome (ARDS)Document3 pagesLesson 2 Acute Respiratory Distress Syndrome (ARDS)Rocelyn CristobalNo ratings yet
- Isabela State University: Republic of The Philippines San Fabian, Echague, Isabela Activity 2 Medical-Surgical NursingDocument9 pagesIsabela State University: Republic of The Philippines San Fabian, Echague, Isabela Activity 2 Medical-Surgical Nursingpinoy HubNo ratings yet
- Epithelial Barriers in Allergy and AsthmaDocument11 pagesEpithelial Barriers in Allergy and AsthmaFrancisco Baca DejoNo ratings yet
- The Pathology of Lung Diseases: I. Restrictive Lung Diseas ESDocument65 pagesThe Pathology of Lung Diseases: I. Restrictive Lung Diseas ESLiana Ika SuwandyNo ratings yet
- Acute Epiglottitis: DR Eric El HittiDocument5 pagesAcute Epiglottitis: DR Eric El HittinoviNo ratings yet
- Aljean Altheo L. Artillo BSN-3B 1. What Are The Pathophysiologies of Chronic Obstructive Pulmonary Disease (COPD) ?Document2 pagesAljean Altheo L. Artillo BSN-3B 1. What Are The Pathophysiologies of Chronic Obstructive Pulmonary Disease (COPD) ?Al TheóNo ratings yet
- Pathology Lecture 1 MSADocument6 pagesPathology Lecture 1 MSAcejix87209No ratings yet
- Balingbing Histo LungsDocument5 pagesBalingbing Histo LungsJonas Zacarias BalingbingNo ratings yet
- Covid and Ebola MsDocument7 pagesCovid and Ebola MsAimee Rochelle MaesaNo ratings yet
- Asphyxia NeonatorumDocument28 pagesAsphyxia NeonatorumAsha jilu100% (1)
- Abc Lec NotesDocument5 pagesAbc Lec NoteshanhananicasNo ratings yet
- Biok 6.4 Gas ExchangeDocument16 pagesBiok 6.4 Gas ExchangeMishaal IrfanNo ratings yet
- Chronic Obstructive Pulmonary Disease: Iman Galal, MDDocument60 pagesChronic Obstructive Pulmonary Disease: Iman Galal, MDYan Sheng HoNo ratings yet
- Principles of Mechanical Ventilation For Non-Critical Care NursesDocument6 pagesPrinciples of Mechanical Ventilation For Non-Critical Care NursesSarah Jane PetalioNo ratings yet
- Jacobs 2015Document6 pagesJacobs 2015rani tiaraNo ratings yet
- Textbook Discussion On Acute Community-Acquired Pneumonia (BSN 3A-Group 6)Document9 pagesTextbook Discussion On Acute Community-Acquired Pneumonia (BSN 3A-Group 6)Jica Marie Bandiola GicaroNo ratings yet
- 3 RestrictiveLungDiseasesDocument14 pages3 RestrictiveLungDiseasesSaiaDaphiNo ratings yet
- COPD: Pathogenesis Environmental Insult To Lungs Genetic SusceptibilityDocument1 pageCOPD: Pathogenesis Environmental Insult To Lungs Genetic SusceptibilityMaria Vhanesa AbuyanNo ratings yet
- Mucociliary ClearanceDocument9 pagesMucociliary Clearancerbatjun576No ratings yet
- Acute/Adulth Respiratory Distress Syndrome (ARDS) : RohmanDocument54 pagesAcute/Adulth Respiratory Distress Syndrome (ARDS) : RohmanMuhammad Rizki Junaidi SaputraNo ratings yet
- The Histological Effects of Covid-19 On The Lower Respiratory SystemDocument9 pagesThe Histological Effects of Covid-19 On The Lower Respiratory SystemIJAR JOURNALNo ratings yet
- Respiratory PhysiologyDocument40 pagesRespiratory PhysiologyBookwormNo ratings yet
- Ards PDFDocument20 pagesArds PDFRuki HartawanNo ratings yet
- Pats 201003-027rn PDFDocument5 pagesPats 201003-027rn PDFKarina Aguirre AlvarezNo ratings yet
- Activity 2 - Types of Sutures and Complications of Surgical Post-OperationDocument3 pagesActivity 2 - Types of Sutures and Complications of Surgical Post-OperationCezanne CruzNo ratings yet
- Taponamiento MucososDocument6 pagesTaponamiento Mucososkarla Carolina Morón TorresNo ratings yet
- Pathophysiology of Tissue Fluid Accumulation in InflammationDocument9 pagesPathophysiology of Tissue Fluid Accumulation in InflammationGLEE ANN UYCOCONo ratings yet
- Atelectasis NFDocument57 pagesAtelectasis NFNurul FathiyaNo ratings yet
- A Review of Complications of Odontogenic InfectionsDocument8 pagesA Review of Complications of Odontogenic InfectionsAndrés Faúndez TeránNo ratings yet
- BOURBON 2009 - BPD An Emphysema-In Search of Commom Therapeutic TargetsDocument11 pagesBOURBON 2009 - BPD An Emphysema-In Search of Commom Therapeutic TargetsRafael JustinoNo ratings yet
- Ncma 113Document4 pagesNcma 113Wonie booNo ratings yet
- Respiratory Module Pathology Lecture 1, Upper Respiratory Tract, Atelectasis, ARDSDocument29 pagesRespiratory Module Pathology Lecture 1, Upper Respiratory Tract, Atelectasis, ARDSalielabadi10No ratings yet
- COVID-19 Is, in The End, An Endothelial Disease: Peter Libby and Thomas Lu ScherDocument7 pagesCOVID-19 Is, in The End, An Endothelial Disease: Peter Libby and Thomas Lu ScherJose Antonio RamosNo ratings yet
- Alveolar Cells Under Mechanical Stressed Niche: Critical Contributors To Pulmonary FibrosisDocument11 pagesAlveolar Cells Under Mechanical Stressed Niche: Critical Contributors To Pulmonary Fibrosisrbatjun576No ratings yet
- The Cough Re Ex: The Janus of Respiratory Medicine: Frontiers in Physiology June 2021Document9 pagesThe Cough Re Ex: The Janus of Respiratory Medicine: Frontiers in Physiology June 2021stellacharlesNo ratings yet
- Biology Model AnswersDocument6 pagesBiology Model AnswersAbdiNo ratings yet
- DiptheriaDocument20 pagesDiptheriaDorothy Pearl Loyola PalabricaNo ratings yet
- Biology 10 00095Document37 pagesBiology 10 00095Dayana CheriyanNo ratings yet
- Head and Neck Space Infections: Parotid AbscessDocument7 pagesHead and Neck Space Infections: Parotid AbscessFara Nindya MaharaniNo ratings yet
- ImpactsDocument4 pagesImpactsnghĩa trầnNo ratings yet
- Jurnal BG AndiDocument36 pagesJurnal BG AndiKristian Sudana HartantoNo ratings yet
- 1 s2.0 S003139551730072XDocument21 pages1 s2.0 S003139551730072XvgmanjunathNo ratings yet
- Disease: Community Acquired PneumoniaDocument4 pagesDisease: Community Acquired PneumoniaJo Traven AzueloNo ratings yet
- 1 s2.0 S0140673622010522 MainDocument18 pages1 s2.0 S0140673622010522 MainMirella Rugel SocolaNo ratings yet
- Mers Cov/H1N1/Corona Virus: By: Gilbert B. Gelig IIDocument25 pagesMers Cov/H1N1/Corona Virus: By: Gilbert B. Gelig IIDaciel GleeNo ratings yet
- Modeling, Simulation and Analysis of Lung Mechanics Using LabviewDocument8 pagesModeling, Simulation and Analysis of Lung Mechanics Using LabviewVinod VargheseNo ratings yet
- Indoor Air Quality and Health: Impact On Respiratory and Cardiovascular SystemDocument4 pagesIndoor Air Quality and Health: Impact On Respiratory and Cardiovascular SystemerpublicationNo ratings yet
- Monochrome Photo 2022 CalendarDocument12 pagesMonochrome Photo 2022 CalendarPANGPANGDEO Shanne Delle B.No ratings yet
- College of Nursing: Benguet State UniversityDocument4 pagesCollege of Nursing: Benguet State UniversityPANGPANGDEO Shanne Delle B.No ratings yet
- In Patient Face Sheet: Caesarean Section 082.1Document8 pagesIn Patient Face Sheet: Caesarean Section 082.1PANGPANGDEO Shanne Delle B.No ratings yet
- III. The Procedure (Oxygen Therapy)Document4 pagesIII. The Procedure (Oxygen Therapy)PANGPANGDEO Shanne Delle B.No ratings yet
- Cardiovascular WorksheetDocument9 pagesCardiovascular WorksheetPANGPANGDEO Shanne Delle B.No ratings yet
- Pangpangdeo Shanne Delle B. - Worksheet 4Document4 pagesPangpangdeo Shanne Delle B. - Worksheet 4PANGPANGDEO Shanne Delle B.No ratings yet
- B9 Barangay AmbuklaoDocument15 pagesB9 Barangay AmbuklaoPANGPANGDEO Shanne Delle B.No ratings yet
- A Detailed Lesson Plan in Living ThingsDocument23 pagesA Detailed Lesson Plan in Living ThingsclarisseNo ratings yet
- How To Read Chest X RayDocument3 pagesHow To Read Chest X RayGeetha PuvanNo ratings yet
- Riwayat Pendidikan: Curiculum VitaeDocument44 pagesRiwayat Pendidikan: Curiculum VitaePrabJot SinGhNo ratings yet
- Frog Dissection PDFDocument19 pagesFrog Dissection PDFTintin GasparNo ratings yet
- Present Your Findings..Document30 pagesPresent Your Findings..Feyer MartinsNo ratings yet
- Perioperative Nursing Hand Out - Postop-1Document22 pagesPerioperative Nursing Hand Out - Postop-1Jamie NarcisoNo ratings yet
- PE NotesDocument20 pagesPE NotesAlma C WalshNo ratings yet
- 病理國考複習 PDFDocument61 pages病理國考複習 PDFAnonymous ZUQcbcNo ratings yet
- PRELIM NCM 112 RleDocument20 pagesPRELIM NCM 112 RleKylle AlimosaNo ratings yet
- Frog ALL SYSTEMS-1Document85 pagesFrog ALL SYSTEMS-1Ranjeet PandeyNo ratings yet
- Chest PhysiotherapyDocument8 pagesChest PhysiotherapyPoova RagavanNo ratings yet
- By Prof - DR.: Ahmed AllamDocument84 pagesBy Prof - DR.: Ahmed Allamdrqazi777No ratings yet
- NCM 114 Midterm Module ContentDocument54 pagesNCM 114 Midterm Module ContentJohn Van Dave TaturoNo ratings yet
- Anatomy and Physiology-A ReviewDocument38 pagesAnatomy and Physiology-A Reviewjava_biscocho1229100% (4)
- Science-9-Q1 M2 - Efren Agdinaoay JRDocument29 pagesScience-9-Q1 M2 - Efren Agdinaoay JRLiezl ValienteNo ratings yet
- Slow Deep Pursed-Lips Breathing Exercise On Vital Lung Capacity in Post-Extubation Patients in The Intensive Care UnitDocument10 pagesSlow Deep Pursed-Lips Breathing Exercise On Vital Lung Capacity in Post-Extubation Patients in The Intensive Care Unitanggi rahmawatiNo ratings yet
- Grade 9 Science 1ST QuarterDocument2 pagesGrade 9 Science 1ST QuarterRechelie Alferez ParanNo ratings yet
- Hsslive Xii Zoology Lab Notes by Navas 2024Document100 pagesHsslive Xii Zoology Lab Notes by Navas 2024spookyvibee666No ratings yet
- Nursing Care Related To Psychological and Physiological Changes of PregnancyDocument180 pagesNursing Care Related To Psychological and Physiological Changes of PregnancyJohanine VillasantiagoNo ratings yet
- Year 9 Biology QuestionsDocument58 pagesYear 9 Biology QuestionsDuong Kha NhiNo ratings yet
- 2022-23 F3 Biology Exam Mock Paper 1 1Document20 pages2022-23 F3 Biology Exam Mock Paper 1 1azuryicerobloxNo ratings yet
- Pathology EssayDocument19 pagesPathology EssayARUNSKNo ratings yet
- 4HB1 02 Que 20220114Document24 pages4HB1 02 Que 20220114DinangaNo ratings yet
- Review Notes On The Anatomy of The LungDocument5 pagesReview Notes On The Anatomy of The LungNabil Abd El-tawabNo ratings yet
- Reading SkillsDocument179 pagesReading SkillsDylan VanslochterenNo ratings yet
- Artificial LungDocument25 pagesArtificial Lungaloove66No ratings yet
- Anatomy: ST ND TH TH Th. RD TH TH THDocument11 pagesAnatomy: ST ND TH TH Th. RD TH TH THskNo ratings yet
- 1001219 急診基礎超音波簡介Document101 pages1001219 急診基礎超音波簡介juice119No ratings yet
- 15a. First Aid ManualDocument73 pages15a. First Aid ManualchimaraiykeNo ratings yet