You might also like
- Microsoft PowerPoint 2016Document63 pagesMicrosoft PowerPoint 2016Timothy Lemuel GulapaNo ratings yet
- Tms Messageusageguide 7.0 Key DownloadingDocument198 pagesTms Messageusageguide 7.0 Key DownloadingHenry S. AdkinNo ratings yet
- PastillasDocument6 pagesPastillasJessa Caringal100% (3)
- Fire and Gas in Safety SystemsDocument5 pagesFire and Gas in Safety Systemsmostafa_1000100% (1)
- Audit Training ManualDocument15 pagesAudit Training ManualNilesh GhamNo ratings yet
- Petroleum Engineering Handbook For The Practicing EngineerDocument6 pagesPetroleum Engineering Handbook For The Practicing EngineerMustafa Alasady67% (3)
- Iso 22476 2 2005 en PDFDocument11 pagesIso 22476 2 2005 en PDFMustafa ÇakırNo ratings yet
- Memory Unit - 5 Coa PDFDocument18 pagesMemory Unit - 5 Coa PDFArun KrishNo ratings yet
- Crocels Community Media Group NMH RatesDocument1 pageCrocels Community Media Group NMH RatesCrocels BriefsNo ratings yet
- Fee Structure (Inclusive of GST) (Applicable From 01st April, 2019)Document1 pageFee Structure (Inclusive of GST) (Applicable From 01st April, 2019)subhashNo ratings yet
- SN Product Description Unit Price Qty Total Price: Date:-8th July 2019 Ref: - RSGS/RH-1101 /july/2019Document1 pageSN Product Description Unit Price Qty Total Price: Date:-8th July 2019 Ref: - RSGS/RH-1101 /july/2019Rakesh HarekarNo ratings yet
- Practicalskillschecklist 13Document15 pagesPracticalskillschecklist 13api-396515657No ratings yet
- QT 22129Document1 pageQT 22129Speciality GeochemNo ratings yet
- Individual Enterprise (Referred Individual) : I. Basic InformationDocument4 pagesIndividual Enterprise (Referred Individual) : I. Basic InformationKevin SiegbahnNo ratings yet
- West Bengal DarpanDocument4 pagesWest Bengal Darpanfunda metricsNo ratings yet
- 2022 Programme Intake Dates & FeesDocument1 page2022 Programme Intake Dates & FeesLee LeeNo ratings yet
- Sinclair User 1 Apr 1982Document68 pagesSinclair User 1 Apr 1982JasonWhite99No ratings yet
- Multidisciplinary Framework For Skills and CostingDocument8 pagesMultidisciplinary Framework For Skills and CostingLelanie van NiekerkNo ratings yet
- Osn Quantastor 2015 Price GuideDocument5 pagesOsn Quantastor 2015 Price GuideImran MohdNo ratings yet
- CLDHEI-Aganon, Von Ymor 2Document1 pageCLDHEI-Aganon, Von Ymor 2Von Ymor AganonNo ratings yet
- To The With: OateaDocument3 pagesTo The With: OateaAbinash acharyaNo ratings yet
- QuotationDocument1 pageQuotationbarbadosrajNo ratings yet
- CHC 447 MedicineDocument20 pagesCHC 447 MedicinePravin ChaudhariNo ratings yet
- SETSCO Services Pte LTD: Non-Destructive Testing Course Programme (Year 2018)Document13 pagesSETSCO Services Pte LTD: Non-Destructive Testing Course Programme (Year 2018)Mai Sỹ HảiNo ratings yet
- TumiDocument14 pagesTumiMiracle /TDNo ratings yet
- Particulars T U V Y: © The Institute of Chartered Accountants of IndiaDocument15 pagesParticulars T U V Y: © The Institute of Chartered Accountants of Indiareniya mathewNo ratings yet
- Production and Operations Department Comp PlanDocument3 pagesProduction and Operations Department Comp PlanPaul Benedick VictorinoNo ratings yet
- Course Total Fee: FEE STRUCTURE (Including GST) - JAIPUR (English Medium) (Applicable From September 1, 2021)Document2 pagesCourse Total Fee: FEE STRUCTURE (Including GST) - JAIPUR (English Medium) (Applicable From September 1, 2021)vijay choudharyNo ratings yet
- Everyday Extras: Get The Same Amount Back Each Time You VisitDocument2 pagesEveryday Extras: Get The Same Amount Back Each Time You Visitfrank.wangNo ratings yet
- Faculty BudgetDocument2 pagesFaculty BudgetIvy Jane EstrellaNo ratings yet
- 2021 22 Technology Tuition IntlDocument2 pages2021 22 Technology Tuition IntlccpiNo ratings yet
- BCIT 2021-22 Full-time/Cohort Technology Fee Schedule Effective Date of This Tuition Schedule: August 1, 2021Document2 pagesBCIT 2021-22 Full-time/Cohort Technology Fee Schedule Effective Date of This Tuition Schedule: August 1, 2021Ricardoe RodriguezNo ratings yet
- 2015-16 and Before Registrations 2018-19 Academic Year Fee TableDocument1 page2015-16 and Before Registrations 2018-19 Academic Year Fee TableCan MutluNo ratings yet
- Esplanade Recital Studio Rental RatesDocument1 pageEsplanade Recital Studio Rental RatesSolasido Music and ArtNo ratings yet
- SBFP 2022-2023 WFPDocument2 pagesSBFP 2022-2023 WFPNicole MontesNo ratings yet
- CS SheetDocument1 pageCS SheetVishnu TamrakarNo ratings yet
- Price BidDocument2 pagesPrice Bidsandy kulkarniNo ratings yet
- IBA CustomizationDocument7 pagesIBA CustomizationRajpal JangraNo ratings yet
- Department of Posts: Ministry of Communications, Government of IndiaDocument5 pagesDepartment of Posts: Ministry of Communications, Government of IndiaBaskar ANgadeNo ratings yet
- PTP - Professional ChefDocument1 pagePTP - Professional ChefjohnNo ratings yet
- Free Structure 2020 21Document8 pagesFree Structure 2020 21I'm AJNo ratings yet
- Ab12a3 Group 3 Delivious Comapny Financial PlanDocument77 pagesAb12a3 Group 3 Delivious Comapny Financial PlanSepalon RheynierNo ratings yet
- Coco Cost of Production1Document3 pagesCoco Cost of Production1Cristobal Macapala Jr.No ratings yet
- Adoress FarmDocument1 pageAdoress FarmJanu MaglenteNo ratings yet
- IAM and KJA Global Presentation - PPSXDocument39 pagesIAM and KJA Global Presentation - PPSXJuan TamadNo ratings yet
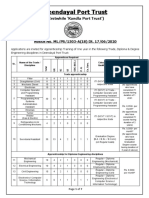
- Advt. Apprenticeship 2020Document7 pagesAdvt. Apprenticeship 2020Vishakha TakodaraNo ratings yet
- Daftar HargaDocument2 pagesDaftar HargaUhi Latief100% (1)
- AlmurilDocument1 pageAlmurilAron paul San MiguelNo ratings yet
- Carswell Checklist 10Document15 pagesCarswell Checklist 10api-400442112No ratings yet
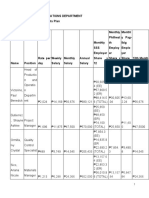
- Future Generali India Life Insurance Co. LTD.: Personaldetails Yo U R Plan D EtailsDocument3 pagesFuture Generali India Life Insurance Co. LTD.: Personaldetails Yo U R Plan D EtailsApoorva kNo ratings yet
- Future Generali India Life Insurance Co. LTD.: Personaldetails Yo U R Plan D EtailsDocument3 pagesFuture Generali India Life Insurance Co. LTD.: Personaldetails Yo U R Plan D EtailsApoorva kNo ratings yet
- Management ConsultancyDocument3 pagesManagement ConsultancyPatrickNo ratings yet
- Production Control Approved RequestDocument1 pageProduction Control Approved RequestAlfon BayuNo ratings yet
- Sale 331 05-06-2023Document2 pagesSale 331 05-06-2023bhaleraokrushna433No ratings yet
- Amanda Wilkes - Week 10Document12 pagesAmanda Wilkes - Week 10api-396549652No ratings yet
- Stock Opname - Check List WomaDocument6 pagesStock Opname - Check List WomaAdmin VendorNo ratings yet
- Training - Seminar: Rizal YahyaDocument23 pagesTraining - Seminar: Rizal YahyaDwikiNo ratings yet
- StockAxis Ajanta Pharma LTD Research Report - BCDocument7 pagesStockAxis Ajanta Pharma LTD Research Report - BCabhinavnarayanNo ratings yet
- Compare - TVs - Sony SingaporeDocument8 pagesCompare - TVs - Sony SingaporeBrishketu PrakashNo ratings yet
- QTN-044-17-NFT Channel Bucket - 10000 AnujDocument10 pagesQTN-044-17-NFT Channel Bucket - 10000 AnujAnuj MittalNo ratings yet
- Reno 7 8GB 256Gb Invoice Flipkart BillDocument2 pagesReno 7 8GB 256Gb Invoice Flipkart BillPriyanka ThakurNo ratings yet
- ABB 4 Pole Contactor, 230V, 40ADocument1 pageABB 4 Pole Contactor, 230V, 40ASEERALANNo ratings yet
- Expenses:: Q: Yearly Budget????Document6 pagesExpenses:: Q: Yearly Budget????Anonymous fyPLVENo ratings yet
- Riya Autolink: Price List Wef 22/02/2023Document1 pageRiya Autolink: Price List Wef 22/02/2023segiw15263No ratings yet
- AsthmaDocument2 pagesAsthmaMarya Fanta C LupuNo ratings yet
- Nicole Brunne-Practical Skills - Week 10Document15 pagesNicole Brunne-Practical Skills - Week 10api-396515657No ratings yet
- CBSE WebinarDocument4 pagesCBSE Webinarshailendra patilNo ratings yet
- The 16 Key Skills Needed To Be A PharmacistDocument28 pagesThe 16 Key Skills Needed To Be A Pharmacistshailendra patilNo ratings yet
- Soft Skills For Pharmacist 2Document5 pagesSoft Skills For Pharmacist 2shailendra patilNo ratings yet
- Soft Skills For Pharmacist 1Document7 pagesSoft Skills For Pharmacist 1shailendra patilNo ratings yet
- Lec3 Prodrug Poly IntroDocument20 pagesLec3 Prodrug Poly Introshailendra patilNo ratings yet
- Soft Skills in The Pharmacy Curriculum: Lilian M. AzzopardiDocument14 pagesSoft Skills in The Pharmacy Curriculum: Lilian M. Azzopardishailendra patilNo ratings yet
- Soft Skills Needed For Pharmacists, How Can We Gain These Skills!Document32 pagesSoft Skills Needed For Pharmacists, How Can We Gain These Skills!shailendra patilNo ratings yet
- Lec2 PkineticsDocument18 pagesLec2 Pkineticsshailendra patilNo ratings yet
- Fact Sheet - Dublin CoreDocument2 pagesFact Sheet - Dublin CorespiderbrigadeNo ratings yet
- For PACS & Remote Primary Diagnosis: The VIDAR AdvantageDocument2 pagesFor PACS & Remote Primary Diagnosis: The VIDAR AdvantageManuelNo ratings yet
- Dns 04fDocument27 pagesDns 04fMohallalibrary NgoNo ratings yet
- Management Information System in Tata MotorsDocument14 pagesManagement Information System in Tata MotorsPRANEET KUMAR 20215066No ratings yet
- Linear Algebra With MatlabDocument5 pagesLinear Algebra With Matlabharish9No ratings yet
- $RC6QPWJDocument36 pages$RC6QPWJralph viruskyNo ratings yet
- Relativity Admin ManualDocument357 pagesRelativity Admin Manualptb2011No ratings yet
- Auth0 Solution OverviewDocument2 pagesAuth0 Solution OverviewCastNo ratings yet
- Deedy CVDocument2 pagesDeedy CVMohammad HassanNo ratings yet
- Option Switches PDFDocument348 pagesOption Switches PDFNima AriaNo ratings yet
- Hiperwall: Videowall Content and Source Management SolutionDocument3 pagesHiperwall: Videowall Content and Source Management Solutionmario maldonadoNo ratings yet
- Optimizing Infrastructure Project ManagementDocument3 pagesOptimizing Infrastructure Project ManagementrongseNo ratings yet
- Suunto TraverseAlpha UserGuide ENDocument46 pagesSuunto TraverseAlpha UserGuide ENnanokoolNo ratings yet
- User Manual Panasonic TCP42G25Document76 pagesUser Manual Panasonic TCP42G25John LingleyNo ratings yet
- ISS PresentationDocument28 pagesISS PresentationPranav PawarNo ratings yet
- Sea Measur. and Forecast - SYST Strona 21Document23 pagesSea Measur. and Forecast - SYST Strona 21MJNo ratings yet
- Con ArtsDocument29 pagesCon Artssophia lizarondoNo ratings yet
- A Review On Basic Deep LearningDocument9 pagesA Review On Basic Deep Learningyanbiao liNo ratings yet
- Huawei OceanStor 9000 Pre-Sales TrainingDocument62 pagesHuawei OceanStor 9000 Pre-Sales TrainingHUMANMANNo ratings yet
- 1.2.2 IP AddressingDocument12 pages1.2.2 IP AddressingCollins JimNo ratings yet
- 2018-2 Course List (Undergraduate) Final (Aug.14)Document4 pages2018-2 Course List (Undergraduate) Final (Aug.14)sultan9mehmed9iiiNo ratings yet
- Tekla CSC Fastrak 2018 v18.1.0 - Download Free SoftwareDocument1 pageTekla CSC Fastrak 2018 v18.1.0 - Download Free SoftwareMarvin MessiNo ratings yet
- Installing and Creating An Oracle Database 19c On Linux 7 With ASMDocument27 pagesInstalling and Creating An Oracle Database 19c On Linux 7 With ASMSamuelNo ratings yet