You might also like
- Laryngopharyngeal and Gastroesophageal Reflux: A Comprehensive Guide to Diagnosis, Treatment, and Diet-Based ApproachesFrom EverandLaryngopharyngeal and Gastroesophageal Reflux: A Comprehensive Guide to Diagnosis, Treatment, and Diet-Based ApproachesCraig H. ZalvanNo ratings yet
- Gerd Info and LinksDocument14 pagesGerd Info and Linksapi-357798429No ratings yet
- Gastroesophageal Reflux Disease PharmacotherapyDocument22 pagesGastroesophageal Reflux Disease PharmacotherapyrinirhynNo ratings yet
- Articulo DigestivoDocument7 pagesArticulo DigestivoDanae MestizoNo ratings yet
- GerdDocument8 pagesGerdLoms KotopNo ratings yet
- Case 7 Questions: I. Understanding The Disease and PathophysiologyDocument6 pagesCase 7 Questions: I. Understanding The Disease and Pathophysiologyapi-532124328No ratings yet
- Gastroesophageal Reflux Disease.Document10 pagesGastroesophageal Reflux Disease.WelhanNo ratings yet
- WJGPT 5 105 PDFDocument9 pagesWJGPT 5 105 PDFMeldhaNo ratings yet
- Gastroesophageal Reflux DiseaseDocument4 pagesGastroesophageal Reflux DiseasemariatheressamercadoNo ratings yet
- Clinical Review: Gastro-Oesophageal Reflux DiseaseDocument6 pagesClinical Review: Gastro-Oesophageal Reflux DiseaseJerome91No ratings yet
- GERDDocument24 pagesGERDBEVERLY JANE COPADANo ratings yet
- GERD SchwartzDocument10 pagesGERD SchwartzMina Tharwat AzerNo ratings yet
- Volume 8, Issue 3, December 2007 - Pathophysiology Gastroesophageal Reflux DiseaseDocument7 pagesVolume 8, Issue 3, December 2007 - Pathophysiology Gastroesophageal Reflux DiseaseIntan AnanthaNo ratings yet
- Gastroesophageal Reflux Disease: From Pathophysiology To TreatmentDocument5 pagesGastroesophageal Reflux Disease: From Pathophysiology To TreatmentQoniek Nuzulul FalakhiNo ratings yet
- S.J.M. Kraemer, HJ. Stein, H. Feussner, J.R. Siewert (Munich)Document1 pageS.J.M. Kraemer, HJ. Stein, H. Feussner, J.R. Siewert (Munich)Ilham ArabNo ratings yet
- Gastric Mucosa Protection MechanismsDocument45 pagesGastric Mucosa Protection MechanismsNicole IoanidNo ratings yet
- Gastroesophageal Reflux DiseaseDocument10 pagesGastroesophageal Reflux DiseaseMohammad Yordan GandaraNo ratings yet
- Acid Related DisordersDocument18 pagesAcid Related DisordersMinto SanjoyoNo ratings yet
- Diagnostico y Tratamiento Del Reflujo Gastroesofagico (RGE)Document9 pagesDiagnostico y Tratamiento Del Reflujo Gastroesofagico (RGE)Sebastian OsorioNo ratings yet
- (Rabeprazole Domperidone) - Product MonographDocument34 pages(Rabeprazole Domperidone) - Product MonographSonu Singh67% (3)
- Ulkus PeptikDocument26 pagesUlkus PeptikKang MunirNo ratings yet
- SSAT Maintenance of Certification: Literature Review On Gastroesophageal Reflux Disease and Hiatal HerniaDocument5 pagesSSAT Maintenance of Certification: Literature Review On Gastroesophageal Reflux Disease and Hiatal HerniaGosadorNo ratings yet
- Gastroesophagean Reflux DiseaseDocument13 pagesGastroesophagean Reflux Diseasedenisa malinaNo ratings yet
- Background: Reflux LaryngitisDocument5 pagesBackground: Reflux LaryngitisElisa Vina JayantiNo ratings yet
- Case ReportDocument6 pagesCase ReportMae GandaNo ratings yet
- 06 - Chapter 03Document4 pages06 - Chapter 03jipir64332No ratings yet
- Comprehensive Resume On Hepatitis ADocument9 pagesComprehensive Resume On Hepatitis AGeoffrey MasyhurNo ratings yet
- Role of Homeopathy in Management of GERDDocument10 pagesRole of Homeopathy in Management of GERDEditor IJTSRDNo ratings yet
- Causes, Symptoms and Treatments of Gastro-esophageal Reflux Disease (GERDDocument2 pagesCauses, Symptoms and Treatments of Gastro-esophageal Reflux Disease (GERDRadenJeremySoeriawidjajaNo ratings yet
- Gastroesophagealreflux Diseaseafterbariatric Procedures: Maria S. Altieri,, Aurora D. PryorDocument13 pagesGastroesophagealreflux Diseaseafterbariatric Procedures: Maria S. Altieri,, Aurora D. PryormaryNo ratings yet
- Gastroesophageal Reflux Disease: Heba Mohammed Abdella Professor of Tropical Medicine, Ain Shams UniversityDocument67 pagesGastroesophageal Reflux Disease: Heba Mohammed Abdella Professor of Tropical Medicine, Ain Shams Universityأحمد الجزارNo ratings yet
- Review Article: Current Pharmacological Management of Gastroesophageal Reflux DiseaseDocument13 pagesReview Article: Current Pharmacological Management of Gastroesophageal Reflux DiseaseAndre ARNo ratings yet
- Gastro-Oesophageal Reflux Disease: EpidemiologyDocument6 pagesGastro-Oesophageal Reflux Disease: EpidemiologyRehan RiyazNo ratings yet
- Laryngopharyngeal Reflux and Treatment OptionsDocument7 pagesLaryngopharyngeal Reflux and Treatment OptionsNutritistNo ratings yet
- Management of Complicated Peptic Ulcer Disease: Stephen W. Behrman, MDDocument8 pagesManagement of Complicated Peptic Ulcer Disease: Stephen W. Behrman, MDClaudia CorjăuceanuNo ratings yet
- 10.2478 - Rjim 2018 0019Document6 pages10.2478 - Rjim 2018 0019Willian HolandaNo ratings yet
- Gastroesophageal Reflux DiseaseDocument2 pagesGastroesophageal Reflux DiseaseKareliya ChiragNo ratings yet
- Gerd 1Document10 pagesGerd 1alfredo lailossaNo ratings yet
- 3B CTC08 Gerd 10.01.16Document41 pages3B CTC08 Gerd 10.01.16Adriel PizarraNo ratings yet
- Theodore Liakakos, George Karamanolis, Paul Patapis, and Evangelos P. MisiakosDocument7 pagesTheodore Liakakos, George Karamanolis, Paul Patapis, and Evangelos P. MisiakosDaniel AdityaNo ratings yet
- Clinical Biochemistry of The Gastrointestinal TractDocument4 pagesClinical Biochemistry of The Gastrointestinal TractReuben JosephNo ratings yet
- Gastroesophageal Reflux Disease Control of Symptoms, Prevention of ComplicationsDocument9 pagesGastroesophageal Reflux Disease Control of Symptoms, Prevention of ComplicationsTiurma SibaraniNo ratings yet
- Gastroesophageal Reflux Disease - StatPearls - NCBI BookshelfDocument9 pagesGastroesophageal Reflux Disease - StatPearls - NCBI BookshelfjoojoNo ratings yet
- Efectos de La Cirugía Bariátrica en El Esófago - Current Op 2018Document6 pagesEfectos de La Cirugía Bariátrica en El Esófago - Current Op 2018Cesar OrtizNo ratings yet
- Surgicaltreatmentof Gastroesophagealreflux Disease: Robert B. Yates,, Brant K. OelschlagerDocument27 pagesSurgicaltreatmentof Gastroesophagealreflux Disease: Robert B. Yates,, Brant K. OelschlagerYigit İskurtNo ratings yet
- 2014 Gastroenterology Clinics of North AmericaDocument4 pages2014 Gastroenterology Clinics of North AmericaMary CogolloNo ratings yet
- The Clinical Management of Gastroesophageal Reflux DiseaseDocument12 pagesThe Clinical Management of Gastroesophageal Reflux DiseaseMahmoud SamiNo ratings yet
- Peptic Ulcer Disease - EMEDICINE.2020Document47 pagesPeptic Ulcer Disease - EMEDICINE.2020qayyum consultantfpsc100% (1)
- HTTPS:WWW Ncbi NLM Nih gov:pmc:articles:PMC4133436:pdf:WJGPT-5-105Document9 pagesHTTPS:WWW Ncbi NLM Nih gov:pmc:articles:PMC4133436:pdf:WJGPT-5-105Doni SaragihNo ratings yet
- CTC Gerd FinalDocument36 pagesCTC Gerd FinaljaipreyraNo ratings yet
- CSPE Protocol: Gastroesophageal Reflux Disease (GERD) : Assessment & ManagementDocument24 pagesCSPE Protocol: Gastroesophageal Reflux Disease (GERD) : Assessment & ManagementHello HelloNo ratings yet
- Peptic Ulcer Treatment: Antacids, H2 Blockers, PPIs & MoreDocument6 pagesPeptic Ulcer Treatment: Antacids, H2 Blockers, PPIs & MoreHossam ArafaNo ratings yet
- GERDDocument4 pagesGERDstudy mailNo ratings yet
- Mulat B.: Gastro Esophageal Reflux Disease (Gerd)Document44 pagesMulat B.: Gastro Esophageal Reflux Disease (Gerd)NehimyaNo ratings yet
- Signs and Symptoms: AdultsDocument15 pagesSigns and Symptoms: AdultsHelen McClintock100% (1)
- Reflux EsophagitisDocument5 pagesReflux EsophagitisAlexis CrdeNo ratings yet
- Oesophageal Reflux - SearchDocument1 pageOesophageal Reflux - SearchnarayananjeyabaluNo ratings yet
- Dental Management of Diseases of The Gastrointestinal SystemDocument61 pagesDental Management of Diseases of The Gastrointestinal SystemkomalgorayaNo ratings yet
- Medical Management of Gastroesophageal Reflux Disease in AdultsDocument10 pagesMedical Management of Gastroesophageal Reflux Disease in AdultsRodica JecanNo ratings yet
- Gastroesophageal Reflux Disease - RepairedDocument40 pagesGastroesophageal Reflux Disease - RepairedSowndharyaNo ratings yet
- Abstract Case PresDocument6 pagesAbstract Case PresSMJ DRDNo ratings yet
- Head To Toe and 13 Areas of AssessmentDocument7 pagesHead To Toe and 13 Areas of AssessmentSMJ DRDNo ratings yet
- Discharged Plan CHF AFIBDocument2 pagesDischarged Plan CHF AFIBSMJ DRDNo ratings yet
- GastroDocument4 pagesGastroSMJ DRDNo ratings yet
- Alginate TherapyDocument12 pagesAlginate TherapySMJ DRDNo ratings yet
- International Journal of Arts, Sciences and Education Volume 3 Issue 1 - March 2022 ISSN: 2799 - 1091 Page No. 71-85Document19 pagesInternational Journal of Arts, Sciences and Education Volume 3 Issue 1 - March 2022 ISSN: 2799 - 1091 Page No. 71-85SMJ DRDNo ratings yet
- NCP No. 5 Risk For SuicideDocument3 pagesNCP No. 5 Risk For SuicideSMJ DRDNo ratings yet
- Schizo PathophyDocument1 pageSchizo PathophySMJ DRDNo ratings yet
- Ham TestDocument1 pageHam TestArif Indra KusumaNo ratings yet
- KENALOGDocument4 pagesKENALOGStefan Codrin CriclevitzNo ratings yet
- Articolo Originale. Documento Di Consenso Tra European Federation of Periodontology e International Diabetes FederationDocument12 pagesArticolo Originale. Documento Di Consenso Tra European Federation of Periodontology e International Diabetes Federationnensy121No ratings yet
- Hematological Abnormalities in SLE Patients at SMCH HospitalDocument1 pageHematological Abnormalities in SLE Patients at SMCH HospitalNATHANAEL SUNGTENo ratings yet
- Surgical Wound Classification Decision TreeDocument1 pageSurgical Wound Classification Decision TreeETNo ratings yet
- New Microsoft Office Word DocumentDocument11 pagesNew Microsoft Office Word DocumentMihaela AndreiNo ratings yet
- BnhyDocument2 pagesBnhybloozy freezyNo ratings yet
- Toxoplasmosis Lesson PlanDocument18 pagesToxoplasmosis Lesson PlanDoubt MudendaNo ratings yet
- Report for Vuyyooru Harish Kumar ReddyDocument5 pagesReport for Vuyyooru Harish Kumar ReddyKiran ReddyNo ratings yet
- 4.krisis Hipertensi IMELS 15Document41 pages4.krisis Hipertensi IMELS 15putusanggraNo ratings yet
- COVID19 Aanpak Van HVAC SystemenDocument4 pagesCOVID19 Aanpak Van HVAC SystemenJan Willem van BorselenNo ratings yet
- Herpes Genitalis: Causes, Symptoms, TreatmentDocument13 pagesHerpes Genitalis: Causes, Symptoms, TreatmentJimson Marc DuranNo ratings yet
- ICD Pintar PER DIAGNOSADocument30 pagesICD Pintar PER DIAGNOSAklinik annisaaNo ratings yet
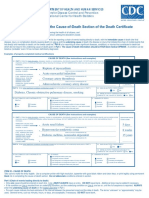
- Instructions For Completing The Cause of Death Section On Death Certificate PDFDocument2 pagesInstructions For Completing The Cause of Death Section On Death Certificate PDFpilcheritoNo ratings yet
- 900 World Fact SheetsDocument2 pages900 World Fact SheetsNik rabekNo ratings yet
- IcdDocument1,590 pagesIcdZainalAbidinNo ratings yet
- Lesson 13 - Diabetes, Cancer and Heart DiseaseDocument28 pagesLesson 13 - Diabetes, Cancer and Heart DiseaseAlejandro GuerreroNo ratings yet
- COVID-19 Workplace Safety: Agency Model Safety PrinciplesDocument7 pagesCOVID-19 Workplace Safety: Agency Model Safety PrinciplesFedSmith Inc.No ratings yet
- EmpyemaDocument1 pageEmpyemaamal abdulrahmanNo ratings yet
- Hepatitis BDocument5 pagesHepatitis BAmple CasaclangNo ratings yet
- Bell's Palsy - Symptoms and Causes - Mayo ClinicDocument6 pagesBell's Palsy - Symptoms and Causes - Mayo ClinicRoxan PacsayNo ratings yet
- Office of The Secretary: FirstDocument12 pagesOffice of The Secretary: FirstJeriz Marie GamboaNo ratings yet
- Bonyah, Badu, Asiedu-Addo - 2016 - Optimal Control Application To An Ebola ModelDocument7 pagesBonyah, Badu, Asiedu-Addo - 2016 - Optimal Control Application To An Ebola Modelgaruda unriNo ratings yet
- GastroenteritisDocument3 pagesGastroenteritisNicoleNo ratings yet
- Rudolph Newborn AtlasDocument322 pagesRudolph Newborn AtlasjprakashjjNo ratings yet
- Dental Treatment of Medical Compromised PatientsDocument50 pagesDental Treatment of Medical Compromised PatientssrinivasNo ratings yet
- Screening for Diabetes in Youth Evidence ReviewDocument127 pagesScreening for Diabetes in Youth Evidence Reviewtechindia2010No ratings yet
- Tele ConsultDocument78 pagesTele ConsultCrystal AnnNo ratings yet
- Brain Tumors - An Overview: Presented by DR - Raviraj.Ghorpade Consultant Brain & Spine Surgeon BelgaumDocument33 pagesBrain Tumors - An Overview: Presented by DR - Raviraj.Ghorpade Consultant Brain & Spine Surgeon BelgaumRAVIRAJ GHORPADE BELGAUM ADVANCED NEUROSURGERYNo ratings yet
- Adult 1 Appendicitis and Peritonitis Guide for NursesDocument6 pagesAdult 1 Appendicitis and Peritonitis Guide for NursesSamah AdnanNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (16)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- The Tennis Partner: A Doctor's Story of Friendship and LossFrom EverandThe Tennis Partner: A Doctor's Story of Friendship and LossRating: 4.5 out of 5 stars4.5/5 (4)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)