You might also like
- A Lay Persons Guide To Medicines - PDF RoomDocument383 pagesA Lay Persons Guide To Medicines - PDF RoomMaricica BotescuNo ratings yet
- Drug SuffixesDocument3 pagesDrug SuffixesjeromeasuncionNo ratings yet
- Depression and Mood - ExamineDocument2 pagesDepression and Mood - ExamineAnonymous RdHoBDhRNo ratings yet
- 11 Antiobiotics, Antifungals, and AntiviralsDocument16 pages11 Antiobiotics, Antifungals, and AntiviralseNo ratings yet
- Antimicrobials and Cytotoxic Drugs: DR Caroline Tetteyfio Koney 37 Military Hospital Accra Feb 2012Document58 pagesAntimicrobials and Cytotoxic Drugs: DR Caroline Tetteyfio Koney 37 Military Hospital Accra Feb 2012Fred OseiNo ratings yet
- Antimicrobial Drugs: Iwan Dwiprahasto Department of Pharmacology and Therapy Faculty of Medicine GMUDocument61 pagesAntimicrobial Drugs: Iwan Dwiprahasto Department of Pharmacology and Therapy Faculty of Medicine GMUadysti100% (1)
- Basic Principles of Pharmacology Handout PDFDocument111 pagesBasic Principles of Pharmacology Handout PDFRazel Kinette AzotesNo ratings yet
- WEEK 9 Antimicrobial ChemotherapyDocument25 pagesWEEK 9 Antimicrobial Chemotherapyotaibynaif100% (2)
- Antibiotics in Dentistry Final VersionDocument87 pagesAntibiotics in Dentistry Final VersionAnji SatsangiNo ratings yet
- Fentanyl Citrate Drug StudyDocument1 pageFentanyl Citrate Drug StudyArthur Christopher CorpuzNo ratings yet
- Anti MicrobialsDocument78 pagesAnti MicrobialsEmma Joel OtaiNo ratings yet
- Drug Study: Nursing DepartmentDocument1 pageDrug Study: Nursing Departmentgiselle chloeNo ratings yet
- AntibioticsDocument37 pagesAntibioticsAnwar Saeed100% (1)
- Principles of Antibiotics: Deepa V Post Graduate Student DSCDS, BangaloreDocument117 pagesPrinciples of Antibiotics: Deepa V Post Graduate Student DSCDS, BangaloreDeepa VenkateshNo ratings yet
- Sun PharmaDocument11 pagesSun PharmaParag Pise100% (1)
- Antibiotics in EndodonticsDocument74 pagesAntibiotics in EndodonticsdrishyaNo ratings yet
- Antimicrobial AgentDocument30 pagesAntimicrobial AgentShardendu MishraNo ratings yet
- Antimicrobial Therapy in Veterinary MedicineFrom EverandAntimicrobial Therapy in Veterinary MedicineSteeve GiguèreRating: 4 out of 5 stars4/5 (1)
- Principles of Antimicrobial TherapyDocument39 pagesPrinciples of Antimicrobial TherapyAsthree Nur AzizahNo ratings yet
- Microbiology Antibiotics AntimicrobialDocument12 pagesMicrobiology Antibiotics AntimicrobialSandeep KumarNo ratings yet
- Serologic Tests Part 3Document2 pagesSerologic Tests Part 3Joshua TrinidadNo ratings yet
- Antibiotics in Oral & Maxillofacial SurgeryDocument50 pagesAntibiotics in Oral & Maxillofacial SurgerysevattapillaiNo ratings yet
- Anti InfectivesDocument4 pagesAnti InfectivespaderamosNo ratings yet
- Antimicrobial Agents Micp AVG Feb2021vDocument50 pagesAntimicrobial Agents Micp AVG Feb2021vHannah RizzyNo ratings yet
- Pharma S03 SBR01 Le1Document15 pagesPharma S03 SBR01 Le1sky vallartaNo ratings yet
- Antimicrobial Therapy: ObjectivesDocument3 pagesAntimicrobial Therapy: ObjectivesSebastian MoronNo ratings yet
- Control of Microorganisms by Chemotherapeutic AgentsDocument10 pagesControl of Microorganisms by Chemotherapeutic AgentsANKITA DOGRANo ratings yet
- Chemotherapy: Dr. Rajendra Nath ProfessorDocument135 pagesChemotherapy: Dr. Rajendra Nath ProfessorHendroMaleNo ratings yet
- MICP LAB (WEEK - 5) Antimicrobial Agents in TherapydocDocument8 pagesMICP LAB (WEEK - 5) Antimicrobial Agents in Therapydoccaitie miracleNo ratings yet
- Antibiotics - PenicillinsDocument14 pagesAntibiotics - PenicillinsDheemanth veerlaNo ratings yet
- AntibioticsDocument63 pagesAntibioticsSahin mollickNo ratings yet
- Introduction To AntimicrobialDocument21 pagesIntroduction To Antimicrobialسامر الرفاعيNo ratings yet
- C.antibiotic PolicyDocument3 pagesC.antibiotic PolicySCQA SHEIKHPURANo ratings yet
- Biosafety and Quality Control (Laboratory)Document7 pagesBiosafety and Quality Control (Laboratory)kerynne dyNo ratings yet
- Week 3 & 4 AntimicrobialsDocument120 pagesWeek 3 & 4 AntimicrobialsQuerubin DandoyNo ratings yet
- Antimicrobial Agents NrsDocument24 pagesAntimicrobial Agents NrsSusmita BeheraNo ratings yet
- Health Service Organisation Aaw 2021 Powerpoint PresentationDocument77 pagesHealth Service Organisation Aaw 2021 Powerpoint Presentationhassan shahidNo ratings yet
- Antibacterial Drugs Are Used To Treat Infections Caused by Pathogenic MO & ParasitesDocument10 pagesAntibacterial Drugs Are Used To Treat Infections Caused by Pathogenic MO & ParasitesMarianne CruzNo ratings yet
- Anaerobic BacteriaDocument4 pagesAnaerobic BacteriaJesette KhoNo ratings yet
- Infection Control Pt. 2: Medical Laboratory Science - Lyceum of The Philippines BatangasDocument4 pagesInfection Control Pt. 2: Medical Laboratory Science - Lyceum of The Philippines BatangasJewel Jehd AlegriaNo ratings yet
- Chemotherapeutic AgentDocument8 pagesChemotherapeutic AgentSumanta Kumar SahooNo ratings yet
- Pharmaceutical Chemistry Ii: Second Year Diploma in PharmacyDocument79 pagesPharmaceutical Chemistry Ii: Second Year Diploma in PharmacyVampire Vampire100% (2)
- Post Test and CfuDocument13 pagesPost Test and CfuMarie Fatima Quidet UdalbeNo ratings yet
- (BACTE-LEC) 8. Antimicrobial Susceptibility TestingDocument6 pages(BACTE-LEC) 8. Antimicrobial Susceptibility TestingCarlo CataagNo ratings yet
- Antimicrobial DrugsDocument89 pagesAntimicrobial DrugsShahane AlisosoNo ratings yet
- Controlling Microbial Growth in Vivo Using Antimicrobial AgentsDocument3 pagesControlling Microbial Growth in Vivo Using Antimicrobial AgentsMaria Gloria Aquino BorjaNo ratings yet
- Antibiotics 23101Document77 pagesAntibiotics 23101TES SENNo ratings yet
- Introduction To Antimicrobials Page 1 of 6Document6 pagesIntroduction To Antimicrobials Page 1 of 6Hassan.shehriNo ratings yet
- Chemotherapy Class NoteDocument112 pagesChemotherapy Class Noteshrey patelNo ratings yet
- Veterinary Pharmacology and Therapeutics II Course OutlineDocument30 pagesVeterinary Pharmacology and Therapeutics II Course OutlineAbdusaburNo ratings yet
- Ceutical Lec 3Document31 pagesCeutical Lec 3Yousef SabaNo ratings yet
- Antibiotik Rasional - Dr. Truly SitorusDocument50 pagesAntibiotik Rasional - Dr. Truly Sitorusvina hidayatNo ratings yet
- Pharma AntimicrobialsDocument19 pagesPharma AntimicrobialsYuku BabyNo ratings yet
- Principles of Antimicrobial TherapyDocument24 pagesPrinciples of Antimicrobial Therapymoha20048100% (1)
- Laboratory Safety and Basic Laboratory EquipmentsDocument40 pagesLaboratory Safety and Basic Laboratory EquipmentsAurora Mae AmoresNo ratings yet
- AntisepsisDocument17 pagesAntisepsissharmavinayak.mf4No ratings yet
- AntibioticsDocument49 pagesAntibioticsShriefElghazalyNo ratings yet
- Microbial ResistanceDocument16 pagesMicrobial ResistanceDixa MeNo ratings yet
- Edited ANTIMICROBIAL AGENTS & SUSCEPTIBILITY TESTINGDocument18 pagesEdited ANTIMICROBIAL AGENTS & SUSCEPTIBILITY TESTINGSaid AbdelaNo ratings yet
- MICP LAB (WEEK - 4) PhysicalChemical Sterilization, Immunity, Hypersensitivity and VaccinesDocument9 pagesMICP LAB (WEEK - 4) PhysicalChemical Sterilization, Immunity, Hypersensitivity and Vaccinescaitie miracleNo ratings yet
- Antibiotics in DentistryDocument90 pagesAntibiotics in DentistryaleryaniNo ratings yet
- ChemotherapyDocument20 pagesChemotherapymeraj khanNo ratings yet
- Day 2 General Microbiology 12-1-2021Document150 pagesDay 2 General Microbiology 12-1-2021ShriefElghazalyNo ratings yet
- Antibiotic: Third Stage By: Dr. Hayfaa Rasheed Al AnssariDocument23 pagesAntibiotic: Third Stage By: Dr. Hayfaa Rasheed Al AnssariMar MaryNo ratings yet
- Multidrug Resistance 2Document74 pagesMultidrug Resistance 2Stefanus Erdana PutraNo ratings yet
- L P 6 Antibiotics - LAB - Fina - 2022Document33 pagesL P 6 Antibiotics - LAB - Fina - 2022Zakria Al-HadadNo ratings yet
- Case Report: Histopathology and Molecular Pathology Analysis On Enteric Tissue of A COVID-19 PatientDocument6 pagesCase Report: Histopathology and Molecular Pathology Analysis On Enteric Tissue of A COVID-19 PatientCaryl Jole PaligsaNo ratings yet
- J Villanueva Group 2Document22 pagesJ Villanueva Group 2Caryl Jole PaligsaNo ratings yet
- L8 MT20 Microbial GrowthDocument9 pagesL8 MT20 Microbial GrowthCaryl Jole PaligsaNo ratings yet
- Trans MT 26 Bernal Lab Topic 6Document3 pagesTrans MT 26 Bernal Lab Topic 6Caryl Jole PaligsaNo ratings yet
- Trans MT 26 Bernal Lab Topic 7Document4 pagesTrans MT 26 Bernal Lab Topic 7Caryl Jole PaligsaNo ratings yet
- History of Viruses: Lord, Tabang. Bless Us With Your Holy SpiritDocument13 pagesHistory of Viruses: Lord, Tabang. Bless Us With Your Holy SpiritCaryl Jole PaligsaNo ratings yet
- Chapter LinksDocument1 pageChapter LinksCaryl Jole PaligsaNo ratings yet
- Name: Caryl Jole O. Paligsa September 23, 2021 GE 8-Ethics Mr. Ismael MagadanDocument1 pageName: Caryl Jole O. Paligsa September 23, 2021 GE 8-Ethics Mr. Ismael MagadanCaryl Jole PaligsaNo ratings yet
- UntitledDocument3 pagesUntitledCaryl Jole PaligsaNo ratings yet
- Group 4 Kim Charles Villarosa Ramona Alexandra Hofemann Caryle Jole Paligsa Fahrodin Tahir Macarambon Jerald Junn Bongcawel John Michael BacurnayDocument1 pageGroup 4 Kim Charles Villarosa Ramona Alexandra Hofemann Caryle Jole Paligsa Fahrodin Tahir Macarambon Jerald Junn Bongcawel John Michael BacurnayCaryl Jole PaligsaNo ratings yet
- Chapter 2 Ethical Relativsm: Name: Caryl Jole O. Paligsa September 23, 2021 GE 8-Ethics Mr. Ismael MagadanDocument1 pageChapter 2 Ethical Relativsm: Name: Caryl Jole O. Paligsa September 23, 2021 GE 8-Ethics Mr. Ismael MagadanCaryl Jole PaligsaNo ratings yet
- Pharma Lec PrelimDocument40 pagesPharma Lec PrelimjoanaalpayNo ratings yet
- Initiating/ Maintaining Peripheral IV InfusionsDocument3 pagesInitiating/ Maintaining Peripheral IV InfusionsHelen May Mayde LingayoNo ratings yet
- Types of Dosage Forms Lecture2,2Document34 pagesTypes of Dosage Forms Lecture2,2Bhuvana TejaNo ratings yet
- Hormone/Contraceptive Use in O&G: Provera Acute Maintena NceDocument2 pagesHormone/Contraceptive Use in O&G: Provera Acute Maintena Ncekhangsiean89No ratings yet
- Guaifenesin: What Is in This LeafletDocument6 pagesGuaifenesin: What Is in This LeafletKate Felongco CambelNo ratings yet
- Stok Opname Ittihad 21Document20 pagesStok Opname Ittihad 21Lisa N PriskasariNo ratings yet
- Nama ObatDocument13 pagesNama Obatsahmin sahminNo ratings yet
- Antifungal Antibiotics - StatPearls - NCBI BookshelfDocument16 pagesAntifungal Antibiotics - StatPearls - NCBI BookshelfsovalaxNo ratings yet
- Laurentius Sandhie Prasetya, Sudadi : PenelitianDocument11 pagesLaurentius Sandhie Prasetya, Sudadi : PenelitianSavira Tapi-TapiNo ratings yet
- Non-Opioid Drugs: A.M.Takdir MusbaDocument38 pagesNon-Opioid Drugs: A.M.Takdir MusbaRey AlwiwikhNo ratings yet
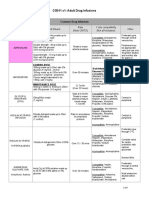
- CG011.v1: Adult Drug Infusions: Drug Dose and Diluent Rate (Note UNITS) Y Site Compatibility (Not All-Inclusive) OtherDocument8 pagesCG011.v1: Adult Drug Infusions: Drug Dose and Diluent Rate (Note UNITS) Y Site Compatibility (Not All-Inclusive) OtheriqbalNo ratings yet
- Pharmacology ReviewersDocument5 pagesPharmacology ReviewersNeisha Halil VillarealNo ratings yet
- Dishman Brochure-Generic-ApisDocument6 pagesDishman Brochure-Generic-ApisYoussef KaidNo ratings yet
- Running Head: 1: PolypharmacyDocument3 pagesRunning Head: 1: PolypharmacyjosephNo ratings yet
- Mindanao State University - Iligan Institute of Technology Student: EGAO, Vanessa Jones C. - Section:260Document1 pageMindanao State University - Iligan Institute of Technology Student: EGAO, Vanessa Jones C. - Section:260Vanessa EgaoNo ratings yet
- Final European Union Herbal Monograph Onechinacea Purpurea L Moench Radix Revision 1 - enDocument7 pagesFinal European Union Herbal Monograph Onechinacea Purpurea L Moench Radix Revision 1 - enKho Siong ThongNo ratings yet
- Pasion, James Nicole R. BSN - 2 NCM 101 Lec Assignment: 1 ML, 0.2 MGDocument4 pagesPasion, James Nicole R. BSN - 2 NCM 101 Lec Assignment: 1 ML, 0.2 MGۦۦ JamesNo ratings yet
- Neofloxin PDFDocument1 pageNeofloxin PDFRazu AhmmedNo ratings yet
- VancomycinDocument6 pagesVancomycinMohammed SaifanNo ratings yet
- Guidelines For Use of MeperidineDocument3 pagesGuidelines For Use of MeperidineAbdul RachmanNo ratings yet
- Public Enemy No 1Document15 pagesPublic Enemy No 1Renukha NallaNo ratings yet
- INCB Precursors Report-EnglishDocument98 pagesINCB Precursors Report-EnglishSi MarNo ratings yet
- Stok Opname Tahun 2022Document56 pagesStok Opname Tahun 2022yunitacahyaniiNo ratings yet