You might also like
- An Evidence-Based Approach to the Management of Nasopharyngeal Cancer: From Basic Science to Clinical Presentation and TreatmentFrom EverandAn Evidence-Based Approach to the Management of Nasopharyngeal Cancer: From Basic Science to Clinical Presentation and TreatmentBaharudin AbdullahNo ratings yet
- Quality of Life Tools in Head and Neck OncologyDocument15 pagesQuality of Life Tools in Head and Neck OncologyAnonymous 9UQNN0No ratings yet
- Afcc Asmiha 2019Document26 pagesAfcc Asmiha 2019Tia WasrilNo ratings yet
- Konker PeralmunI Malang 2021 Workshop ImunologiDocument7 pagesKonker PeralmunI Malang 2021 Workshop ImunologiMikyal BulqiahNo ratings yet
- Critical Appraisal Worksheet TherapyDocument2 pagesCritical Appraisal Worksheet TherapyiwakiwakNo ratings yet
- Kuliah Spine TraumaDocument91 pagesKuliah Spine Traumatutor tujuhNo ratings yet
- 6665 PDFDocument4 pages6665 PDFerindah puspowatiNo ratings yet
- Presentasi Dr. Basuki Rachmad, Sp. An. KICDocument39 pagesPresentasi Dr. Basuki Rachmad, Sp. An. KICinstalasi kamar bedah RSMINo ratings yet
- Pelatihan USGDocument53 pagesPelatihan USGEkoWayanNo ratings yet
- FriS41700 PhlegmasiaCeruleaDolensisaLimbThreateningProblem BhendeDocument54 pagesFriS41700 PhlegmasiaCeruleaDolensisaLimbThreateningProblem BhendeSuren VishvanathNo ratings yet
- Bimbingan ThoraksDocument71 pagesBimbingan ThoraksHedya Nadhrati SururaNo ratings yet
- Algorithms For IV Fluid Therapy in Children and Young People in Hospital Set of 6 PDF 2190274957 PDFDocument6 pagesAlgorithms For IV Fluid Therapy in Children and Young People in Hospital Set of 6 PDF 2190274957 PDFFurqon AfandriNo ratings yet
- GelafusalinfDocument5 pagesGelafusalinfToni Dafia PutraNo ratings yet
- Transcranial Magnetic Stimulation (TMS) : by Denirae DavisDocument8 pagesTranscranial Magnetic Stimulation (TMS) : by Denirae Davisapi-490032735No ratings yet
- Journal Homepage: - : Introduction:-ObjectiveDocument8 pagesJournal Homepage: - : Introduction:-ObjectiveIJAR JOURNALNo ratings yet
- Neuroradiology: Sony Sutrisno Department of Radiology Krida Wacana Christian UniversityDocument46 pagesNeuroradiology: Sony Sutrisno Department of Radiology Krida Wacana Christian UniversityPaulus AnungNo ratings yet
- Medical EmergenciesDocument32 pagesMedical EmergenciesDharani Chowdary Kilari100% (1)
- Eloesser Flap Thoracostomy WindowDocument20 pagesEloesser Flap Thoracostomy WindowJEFFRI JEFFRINo ratings yet
- Lamp.2 Sop Evakuasi MedisDocument2 pagesLamp.2 Sop Evakuasi MedisUci HasbullahNo ratings yet
- Pemeriksaan Foto Thorax Pada Anak-AnakDocument29 pagesPemeriksaan Foto Thorax Pada Anak-AnakRenaldy PamungkasNo ratings yet
- PVC Stoelting Coex 1Document29 pagesPVC Stoelting Coex 1Rudy SiahaanNo ratings yet
- Konas Perdatin 2019Document66 pagesKonas Perdatin 2019Akreditasi RSPC19No ratings yet
- Diksha SepsisDocument67 pagesDiksha SepsisDiksha SinghNo ratings yet
- Modern View of AsthmaDocument27 pagesModern View of AsthmaraisaNo ratings yet
- MYELITISDocument8 pagesMYELITISFebrina RamadhaniNo ratings yet
- Ozid Iv (Omeprazole) : Cedocard Iv (Isosorbid Dinitrat)Document15 pagesOzid Iv (Omeprazole) : Cedocard Iv (Isosorbid Dinitrat)Galih Aryo UtomoNo ratings yet
- Farmakologi Penyakit-Penyakit Degenerasi Tulang Dan SendiDocument19 pagesFarmakologi Penyakit-Penyakit Degenerasi Tulang Dan SendiCici MastaNo ratings yet
- Final 2nd Announcement Konas Perdatin Perdici 2019 - WebsiteDocument65 pagesFinal 2nd Announcement Konas Perdatin Perdici 2019 - Websitetia_drNo ratings yet
- What Do We Know About Patent Dustus Arteriosus - Dr. Adhi Teguh, Sp.a (K)Document39 pagesWhat Do We Know About Patent Dustus Arteriosus - Dr. Adhi Teguh, Sp.a (K)laurentiaNo ratings yet
- BGA Acid Base Stepwise PradikDocument43 pagesBGA Acid Base Stepwise PradikZulfadly NuralimNo ratings yet
- Dysuria Diagnosis AlgorithmDocument9 pagesDysuria Diagnosis AlgorithmM Fikri BetriandaNo ratings yet
- Makalah Bhom 2018 PDFDocument354 pagesMakalah Bhom 2018 PDFAndrian KHoerul Anwar SiiGogon100% (2)
- Shock Types and Treatments GuideDocument14 pagesShock Types and Treatments GuidenataliaNo ratings yet
- Leprosy: An Overview of Pathophysiology: Disusun OlehDocument22 pagesLeprosy: An Overview of Pathophysiology: Disusun OlehDwi Endra Juli PraditoNo ratings yet
- Wsop Asma - Prof Bambang SDocument67 pagesWsop Asma - Prof Bambang SSiti Arieanni KesumaNo ratings yet
- Hasil Tesis AdelaideDocument93 pagesHasil Tesis AdelaideAndi Alfian Zainuddin100% (1)
- Adrenergic AgonistsDocument52 pagesAdrenergic AgonistsTsegaye HailuNo ratings yet
- 2nd Announcement JakNews 2024Document19 pages2nd Announcement JakNews 2024Nando EllaNo ratings yet
- HipospadiaDocument66 pagesHipospadiaDichaNo ratings yet
- 6INVAGINASIDocument18 pages6INVAGINASIhazelelNo ratings yet
- Adult Questionnaire Self-CompletionDocument39 pagesAdult Questionnaire Self-CompletionAnnisa Ratna DNo ratings yet
- Congenital Adrenal HyperplasiaDocument14 pagesCongenital Adrenal HyperplasiabangkitayuNo ratings yet
- Extubation Criteria & Delayed EmergenceDocument3 pagesExtubation Criteria & Delayed EmergenceAnonymous OlS0WZwNo ratings yet
- Air Leak SyndromesDocument2 pagesAir Leak SyndromesIchalAzNo ratings yet
- Soac 2021 First AnnouncementDocument13 pagesSoac 2021 First AnnouncementHendi PrihatnaNo ratings yet
- Pendekatan Klinis Untuk Diagnosis Ensefalitis Autoimun Pada Pasien AnakDocument23 pagesPendekatan Klinis Untuk Diagnosis Ensefalitis Autoimun Pada Pasien AnakDino AdijayaNo ratings yet
- Anesthesia For Transsphenoidal Pituitary Surgery.Document6 pagesAnesthesia For Transsphenoidal Pituitary Surgery.ismaelNo ratings yet
- PratikPatel - Duodenal AtresiaDocument1 pagePratikPatel - Duodenal AtresiaIkhlasia Amali MahzumNo ratings yet
- Karakteristik Gangguan Tidur Pada Penyakit Parkinson Berdasarkan Parkinson Disease SleepDocument8 pagesKarakteristik Gangguan Tidur Pada Penyakit Parkinson Berdasarkan Parkinson Disease SleepAfifa NingrumNo ratings yet
- VT & VFDocument20 pagesVT & VFRafiq SamNo ratings yet
- HSC 2010 3.1 Week 1Document14 pagesHSC 2010 3.1 Week 1Andi Tenri PakkuaNo ratings yet
- Anestesi LokalDocument18 pagesAnestesi LokalTriaditya KresnaNo ratings yet
- Intravenous Fluid Therapy in Critically Ill AdultsDocument17 pagesIntravenous Fluid Therapy in Critically Ill AdultsntnquynhproNo ratings yet
- Medicinus 2011 JulDocument68 pagesMedicinus 2011 JulernawatiNo ratings yet
- Kolestasis Intrahepatal Vs EkstrahepatalDocument4 pagesKolestasis Intrahepatal Vs EkstrahepatalrikarikaNo ratings yet
- BronkiektasisDocument7 pagesBronkiektasisirenaNo ratings yet
- 2nd AnnouncementDocument2 pages2nd AnnouncementFauzan KurniawanNo ratings yet
- Dermatomycosis 2009Document29 pagesDermatomycosis 2009adystiNo ratings yet
- Cutaneous Larval MigransDocument24 pagesCutaneous Larval MigransadystiNo ratings yet
- Tropical and Infectious Subdivision of Internal Department Medical Faculty of Gadjah Mada University YogyakartaDocument95 pagesTropical and Infectious Subdivision of Internal Department Medical Faculty of Gadjah Mada University YogyakartaadystiNo ratings yet
- Erythrosquamous Diseases / Papulosquamous DiseasesDocument38 pagesErythrosquamous Diseases / Papulosquamous DiseasesadystiNo ratings yet
- House Dust Mites DLLDocument32 pagesHouse Dust Mites DLLadystiNo ratings yet
- Poisoning DecontaminationDocument14 pagesPoisoning DecontaminationadystiNo ratings yet
- Acute and Chronic Arterial Occlusion Diagnosis and TreatmentDocument43 pagesAcute and Chronic Arterial Occlusion Diagnosis and TreatmentadystiNo ratings yet
- Acute and Chronic Arterial Occlusion Diagnosis and TreatmentDocument43 pagesAcute and Chronic Arterial Occlusion Diagnosis and TreatmentadystiNo ratings yet
- Bites and VenomDocument23 pagesBites and VenomadystiNo ratings yet
- Dermatitis & Urticaria: Department of Dermato Venereology Faculty of Medicine Gadjah Mada UniversityDocument34 pagesDermatitis & Urticaria: Department of Dermato Venereology Faculty of Medicine Gadjah Mada UniversityadystiNo ratings yet
- Peripheral Arterial Occlusive DiseaseDocument49 pagesPeripheral Arterial Occlusive DiseaseadystiNo ratings yet
- 10 Tahapan Pidi - 16042016Document1 page10 Tahapan Pidi - 16042016adystiNo ratings yet
- Vaccine Preventable Diseases (VPDS) : Ida Safitri Laksono Dept of Child Health Infectious Disease Sub DivisionDocument26 pagesVaccine Preventable Diseases (VPDS) : Ida Safitri Laksono Dept of Child Health Infectious Disease Sub DivisionadystiNo ratings yet
- VTE Prophylaxis in The Hospital: Johan KurniandaDocument35 pagesVTE Prophylaxis in The Hospital: Johan KurniandaadystiNo ratings yet
- Vasculer Imaging 2012 PDFDocument72 pagesVasculer Imaging 2012 PDFadystiNo ratings yet
- Amblyopia Inter Blok 22Document30 pagesAmblyopia Inter Blok 22adystiNo ratings yet
- Tobacco LectureDocument36 pagesTobacco LecturesenoNo ratings yet
- 1 Generation: Cefalexin Cefradin Cefadroxil Cefachlor Yes Yes Yes Yes YesDocument67 pages1 Generation: Cefalexin Cefradin Cefadroxil Cefachlor Yes Yes Yes Yes YesadystiNo ratings yet
- GENITO URINARY PROBLEMS IN CHILDRENDocument78 pagesGENITO URINARY PROBLEMS IN CHILDRENadystiNo ratings yet
- Fever in Children 2010Document27 pagesFever in Children 2010adystiNo ratings yet
- DRUG ALLERGY GUIDEDocument61 pagesDRUG ALLERGY GUIDEadysti100% (1)
- Patient Autonomy: Competent and Incompetent Patient and Research Participant To ConsentDocument27 pagesPatient Autonomy: Competent and Incompetent Patient and Research Participant To ConsentadystiNo ratings yet
- AFP - Blok 3.4. IndoDocument36 pagesAFP - Blok 3.4. IndoadystiNo ratings yet
- Eritro ADocument40 pagesEritro AadystiNo ratings yet
- Immunization: Mei Neni S Pediatric Dept. Faculty of Medicine, Gadjah Mada UniversityDocument35 pagesImmunization: Mei Neni S Pediatric Dept. Faculty of Medicine, Gadjah Mada UniversityadystiNo ratings yet
- Imunol InfeksiDocument26 pagesImunol InfeksiadystiNo ratings yet
- Aging and Endocrine DisordersDocument23 pagesAging and Endocrine DisordersadystiNo ratings yet
- Alrg 10 PDFDocument59 pagesAlrg 10 PDFadystiNo ratings yet
- BasicImmunol PDFDocument56 pagesBasicImmunol PDFadystiNo ratings yet
- Oportunistic in ElderlyDocument19 pagesOportunistic in ElderlyadystiNo ratings yet
- Make the Most of Your Preventive CareDocument5 pagesMake the Most of Your Preventive CarelindytindylindtNo ratings yet
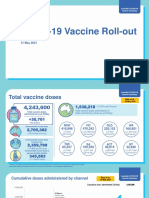
- Covid 19 Vaccine Rollout Update 31 May 2021Document7 pagesCovid 19 Vaccine Rollout Update 31 May 2021Amalia ChairunnisaNo ratings yet
- Vet advice on mites and lice treatment for horsesDocument2 pagesVet advice on mites and lice treatment for horsesJohn OneillNo ratings yet
- Latihan UtnDocument19 pagesLatihan UtnMuhammad SholehNo ratings yet
- Test Bank For Medical Microbiology 6th Edition Patrick R MurrayDocument3 pagesTest Bank For Medical Microbiology 6th Edition Patrick R MurrayJohnCampbellyacer100% (33)
- Hepa B TestDocument1 pageHepa B TestsmilingfroggyNo ratings yet
- James Madison University Immunization FormDocument1 pageJames Madison University Immunization FormMiguel EspirituNo ratings yet
- MPV Congress Schedule - Time SpeakersDocument4 pagesMPV Congress Schedule - Time SpeakersMary AntNo ratings yet
- Medication For Staph InfectionDocument7 pagesMedication For Staph InfectiondelmontlabsNo ratings yet
- Case Study Hiv Answers PDFDocument1 pageCase Study Hiv Answers PDFDaniel Skipworth100% (1)
- Nursing Foundation PROFESSIONAL Practice AssessmentDocument82 pagesNursing Foundation PROFESSIONAL Practice AssessmentdrakyboyNo ratings yet
- Microbiology Comprehensive ExamDocument15 pagesMicrobiology Comprehensive ExamArianne Joy C. TamarayNo ratings yet
- Dna VaccineDocument2 pagesDna VaccinesauravsarkarNo ratings yet
- Microbiology Guide Covering Bacteria, Viruses, Fungi & ImmunityDocument5 pagesMicrobiology Guide Covering Bacteria, Viruses, Fungi & Immunityhhg100% (1)
- BrucellosisDocument26 pagesBrucellosisVasilika GiemsaNo ratings yet
- MHC Class II Deficiency Case StudyDocument2 pagesMHC Class II Deficiency Case StudyBre GlynnNo ratings yet
- Booklet 3Document36 pagesBooklet 3AL Babaran CanceranNo ratings yet
- Homeopathic MedicinesDocument5 pagesHomeopathic MedicinesMiroslav Ilic0% (1)
- Malaria Research in South East AsiaDocument186 pagesMalaria Research in South East AsiaRizal QowiNo ratings yet
- Unang YakapDocument57 pagesUnang YakapHelen Grace Avila100% (3)
- KUMC International Observership Program GuidelinesDocument12 pagesKUMC International Observership Program Guidelinesসোমনাথ মহাপাত্রNo ratings yet
- CLSI Pak-Antibiotic Sensitivity Panels May 2018-NasrullahDocument19 pagesCLSI Pak-Antibiotic Sensitivity Panels May 2018-NasrullahdrNo ratings yet
- Everything You Need to Know About Hepatitis DDocument2 pagesEverything You Need to Know About Hepatitis DYanna Habib-MangotaraNo ratings yet
- School NursingDocument407 pagesSchool NursingKa MiiNo ratings yet
- Vaccines in Zimbabwe InformationDocument8 pagesVaccines in Zimbabwe InformationIsaac GumboNo ratings yet
- Accuracy of A Commercial Igm Elisa For The Diagnosis of Human Leptospirosis in ThailandDocument4 pagesAccuracy of A Commercial Igm Elisa For The Diagnosis of Human Leptospirosis in Thailandrestu anindityaNo ratings yet
- Surigao Education Center Nursing Case Study on Acute GastroenteritisDocument100 pagesSurigao Education Center Nursing Case Study on Acute GastroenteritisJoanne Bernadette AguilarNo ratings yet
- Immunization ScheduleDocument18 pagesImmunization Scheduledr parveen bathlaNo ratings yet
- GSIS Sues IBM, Subsidiary For P100 MillionDocument14 pagesGSIS Sues IBM, Subsidiary For P100 MillionEvaine LeBlancNo ratings yet
- Pentavalent Vaccine Guide For HWs With Answers To FAQsDocument8 pagesPentavalent Vaccine Guide For HWs With Answers To FAQsVamsidhar KavikondalaNo ratings yet
- Uncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicFrom EverandUncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicNo ratings yet
- The Wisdom of Plagues: Lessons from 25 Years of Covering PandemicsFrom EverandThe Wisdom of Plagues: Lessons from 25 Years of Covering PandemicsRating: 4.5 out of 5 stars4.5/5 (5)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisFrom EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (9)
- Do You Believe in Magic?: The Sense and Nonsense of Alternative MedicineFrom EverandDo You Believe in Magic?: The Sense and Nonsense of Alternative MedicineNo ratings yet
- Clean: Overcoming Addiction and Ending America’s Greatest TragedyFrom EverandClean: Overcoming Addiction and Ending America’s Greatest TragedyRating: 4 out of 5 stars4/5 (18)
- The Price of Health: The Modern Pharmaceutical Industry and the Betrayal of a History of CareFrom EverandThe Price of Health: The Modern Pharmaceutical Industry and the Betrayal of a History of CareRating: 4.5 out of 5 stars4.5/5 (3)
- The Invisible Rainbow: A History of Electricity and LifeFrom EverandThe Invisible Rainbow: A History of Electricity and LifeRating: 4.5 out of 5 stars4.5/5 (21)
- Epidemics and Society: From the Black Death to the PresentFrom EverandEpidemics and Society: From the Black Death to the PresentRating: 4.5 out of 5 stars4.5/5 (9)
- Epic Measures: One Doctor. Seven Billion Patients.From EverandEpic Measures: One Doctor. Seven Billion Patients.Rating: 4 out of 5 stars4/5 (13)
- Getting Pregnant Naturally: Healthy Choices To Boost Your Chances Of Conceiving Without Fertility DrugsFrom EverandGetting Pregnant Naturally: Healthy Choices To Boost Your Chances Of Conceiving Without Fertility DrugsRating: 3.5 out of 5 stars3.5/5 (8)
- Deaths of Despair and the Future of CapitalismFrom EverandDeaths of Despair and the Future of CapitalismRating: 4.5 out of 5 stars4.5/5 (30)
- The HPV Vaccine On Trial: Seeking Justice For A Generation BetrayedFrom EverandThe HPV Vaccine On Trial: Seeking Justice For A Generation BetrayedRating: 4.5 out of 5 stars4.5/5 (13)
- The Bodies of Others: The New Authoritarians, COVID-19 and The War Against the HumanFrom EverandThe Bodies of Others: The New Authoritarians, COVID-19 and The War Against the HumanRating: 4.5 out of 5 stars4.5/5 (12)
- Nutritional and Therapeutic Interventions for Diabetes and Metabolic SyndromeFrom EverandNutritional and Therapeutic Interventions for Diabetes and Metabolic SyndromeNo ratings yet
- There Are No Accidents: The Deadly Rise of Injury and Disaster—Who Profits and Who Pays the PriceFrom EverandThere Are No Accidents: The Deadly Rise of Injury and Disaster—Who Profits and Who Pays the PriceRating: 4.5 out of 5 stars4.5/5 (15)
- Quick Fixes: Drugs in America from Prohibition to the 21st Century BingeFrom EverandQuick Fixes: Drugs in America from Prohibition to the 21st Century BingeNo ratings yet
- Development of Questionnaires for Quantitative Medical ResearchFrom EverandDevelopment of Questionnaires for Quantitative Medical ResearchNo ratings yet
- Arthritis Diet: Anti-inflammatory Diet for Arthritis Pain ReliefFrom EverandArthritis Diet: Anti-inflammatory Diet for Arthritis Pain ReliefNo ratings yet
- Fatal Conveniences: The Toxic Products and Harmful Habits That Are Making You Sick—and the Simple Changes That Will Save Your HealthFrom EverandFatal Conveniences: The Toxic Products and Harmful Habits That Are Making You Sick—and the Simple Changes That Will Save Your HealthRating: 4 out of 5 stars4/5 (7)
- Microbiological Quality of FoodsFrom EverandMicrobiological Quality of FoodsL SlanetzNo ratings yet
- Doctored: The Disillusionment of an American PhysicianFrom EverandDoctored: The Disillusionment of an American PhysicianRating: 4 out of 5 stars4/5 (11)
- Covid Vaccine Adverse Reaction Survival Guide: Take Control of Your Recovery and Maximise Healing PotentialFrom EverandCovid Vaccine Adverse Reaction Survival Guide: Take Control of Your Recovery and Maximise Healing PotentialNo ratings yet