You might also like
- Ames Perception ExperimentsDocument108 pagesAmes Perception ExperimentsMichael RoseNo ratings yet
- Permanent Change and Temporary Deviation Request FormDocument1 pagePermanent Change and Temporary Deviation Request FormdrustagiNo ratings yet
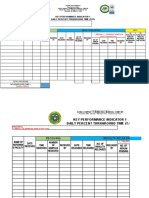
- Partnership Data Sheet QUARTER 1 (January 1, 2019 To March 31, 2019) Grade & SectionDocument4 pagesPartnership Data Sheet QUARTER 1 (January 1, 2019 To March 31, 2019) Grade & SectionKristell PungtilanNo ratings yet
- OSAS AttendanceDocument1 pageOSAS AttendanceMeg PortugalNo ratings yet
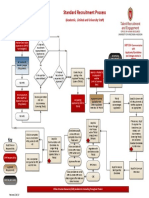
- Standard Recruitment Process MapDocument1 pageStandard Recruitment Process MapfransNo ratings yet
- Guidelines For DentistsDocument42 pagesGuidelines For DentistsNadine El Jundi OuaidaNo ratings yet
- Asset Tracking: Key & Id Card AccessDocument3 pagesAsset Tracking: Key & Id Card AccessShaikat BhaiNo ratings yet
- SFCR1 TemplateDocument3 pagesSFCR1 TemplateRonel MontillanoNo ratings yet
- Registration of Collective Bargaining AgreementsDocument4 pagesRegistration of Collective Bargaining AgreementsQueen Ann NavalloNo ratings yet
- Vehicle Service / Repair Requisition Form: Normal / Routine Service Major (Estimated Above RM3,000.00)Document1 pageVehicle Service / Repair Requisition Form: Normal / Routine Service Major (Estimated Above RM3,000.00)Wang Khong HweeNo ratings yet
- Use This As Reference For Painting Process It May Be Similar To YoursDocument7 pagesUse This As Reference For Painting Process It May Be Similar To Yoursabdelnasser hasanNo ratings yet
- TERC HR - Form 001 v1 - New Hire ChecklistDocument2 pagesTERC HR - Form 001 v1 - New Hire ChecklistMaral Inocencio AltarNo ratings yet
- Summary of Employee Covid-19 ExposureDocument3 pagesSummary of Employee Covid-19 ExposureMary Jane PabustanNo ratings yet
- KPI Daily Turnaround TimeDocument5 pagesKPI Daily Turnaround TimeZianne TremedalNo ratings yet
- CS Form No. 1 Appointment Transmittal and Action FormDocument5 pagesCS Form No. 1 Appointment Transmittal and Action FormLorna Manalo Siman100% (1)
- Checklist of Common RequirementsDocument3 pagesChecklist of Common RequirementsMary Cris SantosNo ratings yet
- Annexure 1Document1 pageAnnexure 1syed quadriNo ratings yet
- Screenshot 2023-05-14 at 12.44.49 PMDocument43 pagesScreenshot 2023-05-14 at 12.44.49 PMrq678phccNo ratings yet
- Form 7 Report FORMATDocument2 pagesForm 7 Report FORMATedgie.soquiasNo ratings yet
- Iv. Civil Service Eligibility: N/A N/A N/A N/A N/ADocument1 pageIv. Civil Service Eligibility: N/A N/A N/A N/A N/AMaria Monica SomeraNo ratings yet
- 1-Formulir SWR 1Document1 page1-Formulir SWR 1Adrianus PramudhitaNo ratings yet
- PRIME-HRM ASSESSMENT CHECKLIST OPTIMIZERDocument6 pagesPRIME-HRM ASSESSMENT CHECKLIST OPTIMIZERGezzane Ventura AlegroNo ratings yet
- CSF Form No. 2 DOLE Central Office BureausDocument1 pageCSF Form No. 2 DOLE Central Office BureausAngelica Gallos - MadijaNo ratings yet
- 80.85% On Going Ateneo de Davao University Civil Engineering Licensure ExaminationDocument1 page80.85% On Going Ateneo de Davao University Civil Engineering Licensure ExaminationreneotejrboardexamNo ratings yet
- Cs Form No. 34-d Plantilla of Casual Appointment - Lgu AccreditedDocument2 pagesCs Form No. 34-d Plantilla of Casual Appointment - Lgu AccreditedgbenjielizonNo ratings yet
- Vendor Approval Permit - Pressure & Flow Control IndustriesDocument2 pagesVendor Approval Permit - Pressure & Flow Control Industries9893203028No ratings yet
- PCUDocument5 pagesPCUashenjayawardana37No ratings yet
- Guidelines for Dentists (1)Document41 pagesGuidelines for Dentists (1)pradeep samuelNo ratings yet
- JASH Engineering LTD.: Product Nonconformity ReportDocument3 pagesJASH Engineering LTD.: Product Nonconformity ReportmanojNo ratings yet
- Project/Company Logo Title of Itp: Date of Issue: This ITP Accompanies The Method StatementDocument1 pageProject/Company Logo Title of Itp: Date of Issue: This ITP Accompanies The Method StatementAbdullahNo ratings yet
- CS Form No. 212 Revised Personal Data Sheet 02Document1 pageCS Form No. 212 Revised Personal Data Sheet 02Ryan BenzonNo ratings yet
- Graduate Admissions Deferment/Reprocessing Form: Please Print All EntriesDocument1 pageGraduate Admissions Deferment/Reprocessing Form: Please Print All Entriestin vicNo ratings yet
- Inspection Checklist For Waterproofing WorksDocument4 pagesInspection Checklist For Waterproofing WorkshishamndtNo ratings yet
- CS Form No. 1 Appointment Transmittal and Action FormDocument4 pagesCS Form No. 1 Appointment Transmittal and Action FormDeejay Rubio OpelacNo ratings yet
- Requirements Documentation for Sharjah Airport Authority ProjectDocument1 pageRequirements Documentation for Sharjah Airport Authority ProjecttawfikNo ratings yet
- Move-Out Notice and Clearance Form - Fillable v2Document1 pageMove-Out Notice and Clearance Form - Fillable v2Slumberland TradingNo ratings yet
- 5.1 Preparation Approval of Syllabus and Learning PlanDocument10 pages5.1 Preparation Approval of Syllabus and Learning PlanRezuREXionNo ratings yet
- CSC Form No. 1 Revised 2017Document5 pagesCSC Form No. 1 Revised 2017Bhogz BiyaNo ratings yet
- Tracking DepEd Division Funds for Disaster MonitoringDocument2 pagesTracking DepEd Division Funds for Disaster MonitoringMamad Tomara BatingoloNo ratings yet
- Pull Out FormDocument1 pagePull Out FormMerry Jaine OrtilloNo ratings yet
- Sample PPAP Level-3Document36 pagesSample PPAP Level-3Mr. Mafia BhargavNo ratings yet
- PDF CSC Personal Data Sheet PDS 2017 Page2Document1 pagePDF CSC Personal Data Sheet PDS 2017 Page2Shan FukasanNo ratings yet
- Material Delivered Received Inspection ReportDocument2 pagesMaterial Delivered Received Inspection ReportUbaidullah KhanNo ratings yet
- Form SWRDocument1 pageForm SWRAdrianus PramudhitaNo ratings yet
- Turn Over Checklist - Revised 2022Document1 pageTurn Over Checklist - Revised 2022jacetcane.escasinasNo ratings yet
- PTA-JSA-001-Mobilization Deployment of Manpower & Beginning of The JobDocument3 pagesPTA-JSA-001-Mobilization Deployment of Manpower & Beginning of The JobSaiyad RiyazaliNo ratings yet
- Rev.04 Action Plan - KFS-IMSF-OTP-04-Action Plan 211018Document1 pageRev.04 Action Plan - KFS-IMSF-OTP-04-Action Plan 211018Amit ChahandeNo ratings yet
- Inspection and Test Plan For Painting of Exposed Interior Beams and SlabsDocument10 pagesInspection and Test Plan For Painting of Exposed Interior Beams and SlabsMike MagatNo ratings yet
- Move-Out Notice and Clearance Form: Item NoDocument1 pageMove-Out Notice and Clearance Form: Item NoJohn Basil ManuelNo ratings yet
- Move-In Notice and Clearance Form - Fillable v2Document1 pageMove-In Notice and Clearance Form - Fillable v2Slumberland TradingNo ratings yet
- Job Contractors and SubContractorsDocument4 pagesJob Contractors and SubContractorsstanNo ratings yet
- Routing and Transmittal Slip Template ExampleDocument1 pageRouting and Transmittal Slip Template ExampleJeff TuganoNo ratings yet
- List of Sub EngineersDocument19 pagesList of Sub EngineersRavi Kumar MogilsettiNo ratings yet
- CS Form No. 1 Appointment Transmittal and Action Form EnhancedDocument4 pagesCS Form No. 1 Appointment Transmittal and Action Form EnhancedRey OliverosNo ratings yet
- RFQ & Sample Approval ProcessDocument1 pageRFQ & Sample Approval ProcessKarthik MadhavanNo ratings yet
- Plan de Surveillance Pièce PlastiqueDocument2 pagesPlan de Surveillance Pièce PlastiqueFida GhanmiNo ratings yet
- JRF TemplateDocument1 pageJRF TemplateMiguel Luis RiveraNo ratings yet
- SSS SPMS Form 1 ReviewDocument1 pageSSS SPMS Form 1 ReviewSam LagoNo ratings yet
- Iil W 03 07Document2 pagesIil W 03 07Raheel MalikNo ratings yet
- Hammad CV (1) - 1Document1 pageHammad CV (1) - 1Raheel MalikNo ratings yet
- World Standard DayDocument1 pageWorld Standard DayRaheel MalikNo ratings yet
- Ethics and ComplianceDocument14 pagesEthics and ComplianceRaheel MalikNo ratings yet
- A.B Restaurant MenuDocument28 pagesA.B Restaurant MenuRaheel MalikNo ratings yet
- OCTG Consultancy Proposes QMS for Dewan CementDocument5 pagesOCTG Consultancy Proposes QMS for Dewan CementRaheel MalikNo ratings yet
- DCL IT Department SOP for Hardware, Software & Network MaintenanceDocument11 pagesDCL IT Department SOP for Hardware, Software & Network MaintenanceRaheel MalikNo ratings yet
- Departmental Visit ReportDocument2 pagesDepartmental Visit ReportRaheel MalikNo ratings yet
- Management of Change FormDocument2 pagesManagement of Change FormRaheel MalikNo ratings yet
- Q1 9th Conformity Matrix - Rev 2Document32 pagesQ1 9th Conformity Matrix - Rev 2Raheel MalikNo ratings yet
- Evaluation Sheet To Be Filled by The Principal/Head Teacher For "Nation Builder Award" (Outstanding Teacher Award)Document1 pageEvaluation Sheet To Be Filled by The Principal/Head Teacher For "Nation Builder Award" (Outstanding Teacher Award)ckNo ratings yet
- 1 ZXMSG 5200 (V2 (1) .0.2) Technical ManualDocument69 pages1 ZXMSG 5200 (V2 (1) .0.2) Technical ManualNatan Getahun100% (2)
- About These Lesson Plans and ResourcesDocument8 pagesAbout These Lesson Plans and ResourcesAhmer TariqNo ratings yet
- The Making of A Modern Filipino HouseDocument16 pagesThe Making of A Modern Filipino HouseIvy Joy CamposNo ratings yet
- Aristotle's View of Substance as FormDocument4 pagesAristotle's View of Substance as FormYaniv AlgrablyNo ratings yet
- Amulet Felicia Brochure 1Document2 pagesAmulet Felicia Brochure 1emrenj50% (2)
- Feap Element LibraryDocument6 pagesFeap Element LibrarySnaga VjereNo ratings yet
- Impact of Hazards on Women and Children in South AsiaDocument10 pagesImpact of Hazards on Women and Children in South AsiaBepul HossenNo ratings yet
- Prep 3 S – 1st Term Virtual WorldDocument49 pagesPrep 3 S – 1st Term Virtual WorldAmarNo ratings yet
- Understanding Community Dynamics and ActionsDocument8 pagesUnderstanding Community Dynamics and ActionsChristian Guimban100% (2)
- Environmental Justice Case StudyDocument3 pagesEnvironmental Justice Case StudyIrish Pauline L. EreñoNo ratings yet
- Central Fire Station Project BriefDocument80 pagesCentral Fire Station Project Briefahmad.alatawnehNo ratings yet
- Graffiti Thesis StatementDocument7 pagesGraffiti Thesis Statementerikamorrisfortlauderdale100% (1)
- Hubungan Pelayanan Gizi, Kualitas Makanan, Dan Konseling Terhadap Kepuasan Pasien Di RSUD BalarajaDocument9 pagesHubungan Pelayanan Gizi, Kualitas Makanan, Dan Konseling Terhadap Kepuasan Pasien Di RSUD Balarajap17331174039 KUNTI ZAKIYAH MUSYRIFAHNo ratings yet
- Business meeting workshopDocument3 pagesBusiness meeting workshopEdison David GuapachoNo ratings yet
- Soal English Usbn 19Document8 pagesSoal English Usbn 19Gina Inayatul MaulaNo ratings yet
- Oracle Session Traffic LightsDocument13 pagesOracle Session Traffic Lightspiciul7001No ratings yet
- 이산수학 유석인 pptDocument29 pages이산수학 유석인 ppt최규민100% (1)
- Test 5 TransDocument7 pagesTest 5 TransNguyễn ThươngNo ratings yet
- Critical Reading-ArtsHumanities-hand Outs 5853487c802c3Document26 pagesCritical Reading-ArtsHumanities-hand Outs 5853487c802c3Rosatri HandayaniNo ratings yet
- Journal Review ChecklistsDocument7 pagesJournal Review ChecklistsAnkur ChopraNo ratings yet
- 4PH0 1P Que 20140515Document28 pages4PH0 1P Que 20140515ramexistsNo ratings yet
- Nine - Principles For Conscious Living - Bill HarrisDocument37 pagesNine - Principles For Conscious Living - Bill HarrisLorenzo Rodriguez100% (1)
- CAREL Products - Isothermal HumidifiersDocument60 pagesCAREL Products - Isothermal HumidifiersArnulfo Rafael Álvarez OliverosNo ratings yet
- University of Adelaide Business School Review MagazineDocument33 pagesUniversity of Adelaide Business School Review MagazineFaculty of the ProfessionsNo ratings yet
- Femoroacetabular Impingement: A ReviewDocument6 pagesFemoroacetabular Impingement: A ReviewSantiago Sandoval JiménezNo ratings yet
- College Interview Questions: 12 to Prepare ForDocument4 pagesCollege Interview Questions: 12 to Prepare ForMaria NistorNo ratings yet
- Eee 2018Document4 pagesEee 2018kesavantNo ratings yet
- DirectX TutorialDocument128 pagesDirectX Tutorialsilly_rabbitzNo ratings yet