You might also like
- Dizziness and VertigoDocument6 pagesDizziness and VertigoJose Luis De GuzmanNo ratings yet
- Narcolepsy, A Simple Guide to the Condition, Treatment and Related DiseasesFrom EverandNarcolepsy, A Simple Guide to the Condition, Treatment and Related DiseasesRating: 1 out of 5 stars1/5 (2)
- Respiratory System DisordersDocument353 pagesRespiratory System Disordersይደግ አብነውNo ratings yet
- NCM 116 - Nursing Care of Patients With Neurologic DysfunctionDocument11 pagesNCM 116 - Nursing Care of Patients With Neurologic DysfunctionRigel Kent C. TobiasNo ratings yet
- Syncope, A Simple Guide to the Condition, Treatment and Related DiseasesFrom EverandSyncope, A Simple Guide to the Condition, Treatment and Related DiseasesNo ratings yet
- Acupuncture PointsDocument120 pagesAcupuncture PointsmineraNo ratings yet
- Dizziness - Vertigo and HomoeopathyDocument38 pagesDizziness - Vertigo and HomoeopathyDr. Rajneesh Kumar Sharma MD HomNo ratings yet
- A Simple Guide to Parkinson's Disease and Related Brain ConditionsFrom EverandA Simple Guide to Parkinson's Disease and Related Brain ConditionsNo ratings yet
- Alsangedy Bullets For Paces Angioedema 2nd EditionDocument2 pagesAlsangedy Bullets For Paces Angioedema 2nd EditionGhulamMemonNo ratings yet
- Cerebrovascular Accident (Stroke) : - Large Artery Thromboses Are - Small Penetrating EmboliDocument7 pagesCerebrovascular Accident (Stroke) : - Large Artery Thromboses Are - Small Penetrating EmboliKimberly Joy GregorioNo ratings yet
- Paul Hellyer - Public Opinion 10102019Document4 pagesPaul Hellyer - Public Opinion 10102019House of Dust100% (1)
- Critical Care MCQsDocument514 pagesCritical Care MCQsbgman83% (18)
- Cerebrovascular AccidentDocument31 pagesCerebrovascular AccidentKoRnflakes83% (6)
- Risk Factors For Periodontal Diseases 2022Document13 pagesRisk Factors For Periodontal Diseases 2022SnowNo ratings yet
- NCM 116: Neurologic Dysfunctions: Joyce Bernadette P. Andot - Anna Delle Nicole P. Aranding, BSN-IIIDocument46 pagesNCM 116: Neurologic Dysfunctions: Joyce Bernadette P. Andot - Anna Delle Nicole P. Aranding, BSN-IIIMercy Anne EcatNo ratings yet
- DISORDERS of The EYE and EARDocument8 pagesDISORDERS of The EYE and EARAnna Carmela P. MelendezNo ratings yet
- Delirium and Its ManagmentDocument64 pagesDelirium and Its ManagmentViren Solanki100% (1)
- Administering Oral Medications: Melendez, Anna Carmela PDocument19 pagesAdministering Oral Medications: Melendez, Anna Carmela PAnna Carmela P. MelendezNo ratings yet
- Hypermagnesemia: Lim - Madalan - Madelo - MagalitDocument17 pagesHypermagnesemia: Lim - Madalan - Madelo - MagalitKyle De Sagun Oteda100% (1)
- XN - Clinical Case - ReportDocument83 pagesXN - Clinical Case - Report郑伟健No ratings yet
- Epilepsy: Alabama Brain BeeDocument15 pagesEpilepsy: Alabama Brain Beebrainbeeuab100% (1)
- 2020 Mcqs Endondontic EmergencyDocument17 pages2020 Mcqs Endondontic Emergencyareej alblowi100% (4)
- Case 5 SeizureDocument17 pagesCase 5 SeizureGrace Tanajura100% (2)
- DeliriumDocument27 pagesDeliriumBushra EjazNo ratings yet
- Entrapment Neuropathies Conversion-GateDocument76 pagesEntrapment Neuropathies Conversion-GateRam ReddyNo ratings yet
- Cerebrovascular Accidents: Julius Ceasar P. Sinco, R.NDocument30 pagesCerebrovascular Accidents: Julius Ceasar P. Sinco, R.Njayz-ceeNo ratings yet
- Metabolic EncephalopathyDocument22 pagesMetabolic Encephalopathytricia isabellaNo ratings yet
- CP 11 MX of Spinal Cord DisordersDocument44 pagesCP 11 MX of Spinal Cord DisordersNur Amaleeza Abdul MananNo ratings yet
- MS MidtermDocument3 pagesMS MidtermDaphney Ruth LeocadioNo ratings yet
- Seizures and EpilepsyDocument3 pagesSeizures and Epilepsyjoshua_villangcaNo ratings yet
- Neuro NotesDocument15 pagesNeuro NotesClyde CapapasNo ratings yet
- The Child With A Neurologic DisorderDocument42 pagesThe Child With A Neurologic DisorderLeilani FullerNo ratings yet
- Increased Intracranial Pressure (Iicp)Document3 pagesIncreased Intracranial Pressure (Iicp)رجمه ديوانNo ratings yet
- Alterations in Cognitive Systems, Cerebral Hemodynamics, and Motor FunctionDocument54 pagesAlterations in Cognitive Systems, Cerebral Hemodynamics, and Motor FunctionKeatonNo ratings yet
- Neonatal Seizures: Queensland Clinical GuidelinesDocument18 pagesNeonatal Seizures: Queensland Clinical GuidelinesAhmad WardimanNo ratings yet
- Medsurg Finals TheoryDocument27 pagesMedsurg Finals TheoryKAYE PAULINE SERVIDADNo ratings yet
- Unconscious and Comatose Patients DR Moses KazevuDocument17 pagesUnconscious and Comatose Patients DR Moses KazevuMoses Jr KazevuNo ratings yet
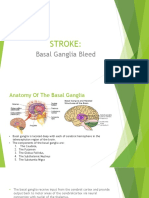
- Stroke:: Basal Ganglia BleedDocument11 pagesStroke:: Basal Ganglia BleedTito A. PutraNo ratings yet
- Hydrocephelus: - NeurologyDocument29 pagesHydrocephelus: - NeurologyImraan MohaNo ratings yet
- Module 6 - Medical - Surgical NursingDocument4 pagesModule 6 - Medical - Surgical NursingJohiarra TabigneNo ratings yet
- Cerebrovascular AcccidentDocument46 pagesCerebrovascular AcccidentFatin AmirahNo ratings yet
- Minimizing Bleeding: Late SignDocument12 pagesMinimizing Bleeding: Late SignMatth N. ErejerNo ratings yet
- Approach To Comatose Patient: Nurul Izzah Binti AriffinDocument27 pagesApproach To Comatose Patient: Nurul Izzah Binti AriffinNurul IzzahNo ratings yet
- ParkinsonsDocument2 pagesParkinsonspsyNo ratings yet
- ParkinsonsDocument2 pagesParkinsonspsyNo ratings yet
- Encephalopathies: Zerlyn T. Leonardo, M.D., FPCP, FPNADocument50 pagesEncephalopathies: Zerlyn T. Leonardo, M.D., FPCP, FPNAJanellee DarucaNo ratings yet
- PCFM Case DiscussionDocument17 pagesPCFM Case DiscussionJoherNo ratings yet
- Diabetes MellitusDocument3 pagesDiabetes MellitusShan NaseoulNo ratings yet
- Anomalies of Accommodation: Mr. Natnael L. (Lecturer) April/2017Document33 pagesAnomalies of Accommodation: Mr. Natnael L. (Lecturer) April/2017henok birukNo ratings yet
- Hepatic Encephalopathy: PRESENTER:Dr - Ch.Priyanka (DNB Junior Resident) Moderator: DR - Thirupathi Reddy (AssociateDocument19 pagesHepatic Encephalopathy: PRESENTER:Dr - Ch.Priyanka (DNB Junior Resident) Moderator: DR - Thirupathi Reddy (AssociatePriyanka ChinthapalliNo ratings yet
- Cognitive DisordersDocument67 pagesCognitive DisordersNariska CooperNo ratings yet
- Neuro DisordersDocument60 pagesNeuro DisordersLovelights ZamoraNo ratings yet
- Epilepsy and Seizures: Partial or Focal Seizures May Be Classified AsDocument2 pagesEpilepsy and Seizures: Partial or Focal Seizures May Be Classified AsMarissa AsimNo ratings yet
- NeurosurgeryDocument5 pagesNeurosurgerysusheewa100% (1)
- Cognitive DisordersDocument4 pagesCognitive DisordersJustine BayabosNo ratings yet
- Shock PPT NewDocument21 pagesShock PPT NewcjimkarlNo ratings yet
- Geriatrics...... DR Mazhar (03066980980)Document44 pagesGeriatrics...... DR Mazhar (03066980980)azamneha341No ratings yet
- English Task in Nursing 2 SondaDocument4 pagesEnglish Task in Nursing 2 SondayulisulistiyoNo ratings yet
- Care of Older Adult in Chronic ConfusionDocument7 pagesCare of Older Adult in Chronic ConfusionClaire MachicaNo ratings yet
- Cerebrovascular Accident StrokeDocument3 pagesCerebrovascular Accident StrokeLuis LazaroNo ratings yet
- Nursing Care Plan Cues Nursing Diagnosis Objective Intervention Rationale Evaluation SubjectiveDocument2 pagesNursing Care Plan Cues Nursing Diagnosis Objective Intervention Rationale Evaluation SubjectiveFreisanChenMandumotanNo ratings yet
- Pathophysiology FinalDocument3 pagesPathophysiology Finaljustineneri324No ratings yet
- Too Little Insulin: Chronic ComplicationsDocument3 pagesToo Little Insulin: Chronic ComplicationsMeryville JacildoNo ratings yet
- Spina Bifida: by DR - Zakir Uk DPT, MSPT MSK (Kmu)Document19 pagesSpina Bifida: by DR - Zakir Uk DPT, MSPT MSK (Kmu)syge zwvuNo ratings yet
- GC EncephilitisDocument1 pageGC EncephilitisCik MunirahNo ratings yet
- Home Care: How To Manage Patient With Longterm Homecare: Prevention of Hospitalization and Infection Source ControlDocument71 pagesHome Care: How To Manage Patient With Longterm Homecare: Prevention of Hospitalization and Infection Source ControlRizal ArzaniNo ratings yet
- NeuroDocument87 pagesNeuroSHANIA FUNDALNo ratings yet
- Increased Icp NoesDocument3 pagesIncreased Icp NoesDarren Mae MosadaNo ratings yet
- Week 7 - Neurological Disorders Fall 2020 - With NarrationsDocument30 pagesWeek 7 - Neurological Disorders Fall 2020 - With NarrationsM SHOAIB KHALIDNo ratings yet
- Neurological Emergencies d10Document60 pagesNeurological Emergencies d10Diana NurulNo ratings yet
- Cerebrovascular Accident CVADocument40 pagesCerebrovascular Accident CVAAndrea IlaidaNo ratings yet
- Clinical Therapeutics Oral Revalida Review Notes: CASE 1: Dr. Abraham Daniel C. CruzDocument31 pagesClinical Therapeutics Oral Revalida Review Notes: CASE 1: Dr. Abraham Daniel C. CruzNoreenNo ratings yet
- NCM 121 Skills Midterm 212023Document8 pagesNCM 121 Skills Midterm 212023Anna Carmela P. MelendezNo ratings yet
- NCM 121 LEC MIDTERM 150323 ShortDocument5 pagesNCM 121 LEC MIDTERM 150323 ShortAnna Carmela P. MelendezNo ratings yet
- Interview GuideDocument1 pageInterview GuideAnna Carmela P. MelendezNo ratings yet
- Chapter 10 Group 5Document32 pagesChapter 10 Group 5Anna Carmela P. MelendezNo ratings yet
- Escalation TherapyDocument1 pageEscalation TherapyAnna Carmela P. MelendezNo ratings yet
- Form3 6Document1 pageForm3 6Anna Carmela P. MelendezNo ratings yet
- West Visayas State University: Unified Research Ethics Review CommitteeDocument1 pageWest Visayas State University: Unified Research Ethics Review CommitteeAnna Carmela P. MelendezNo ratings yet
- Who Am I?: A Reflection PaperDocument1 pageWho Am I?: A Reflection PaperAnna Carmela P. MelendezNo ratings yet
- West Visayas State University: Unified Research Ethics Review CommitteeDocument2 pagesWest Visayas State University: Unified Research Ethics Review CommitteeAnna Carmela P. MelendezNo ratings yet
- Death: Melendez, Anna Carmela P. BSN-1B NCM 103 (LEC)Document1 pageDeath: Melendez, Anna Carmela P. BSN-1B NCM 103 (LEC)Anna Carmela P. MelendezNo ratings yet
- West Visayas State University: Unified Research Ethics Review CommitteeDocument2 pagesWest Visayas State University: Unified Research Ethics Review CommitteeAnna Carmela P. MelendezNo ratings yet
- Unified Research Ethics Review Committee: Form 3.5 Deviation / Non-Compliance / Violation ReportDocument1 pageUnified Research Ethics Review Committee: Form 3.5 Deviation / Non-Compliance / Violation ReportAnna Carmela P. MelendezNo ratings yet
- Unified Research Ethics Review Committee: Form 3.5 Deviation / Non-Compliance / Violation ReportDocument1 pageUnified Research Ethics Review Committee: Form 3.5 Deviation / Non-Compliance / Violation ReportAnna Carmela P. MelendezNo ratings yet
- West Visayas State University: Unified Research Ethics Review CommitteeDocument2 pagesWest Visayas State University: Unified Research Ethics Review CommitteeAnna Carmela P. MelendezNo ratings yet
- West Visayas State University: Unified Research Ethics Review CommitteeDocument2 pagesWest Visayas State University: Unified Research Ethics Review CommitteeAnna Carmela P. MelendezNo ratings yet
- West Visayas State University: Unified Research Ethics Review CommitteeDocument2 pagesWest Visayas State University: Unified Research Ethics Review CommitteeAnna Carmela P. MelendezNo ratings yet
- Anaplastic Thyroid CancerDocument40 pagesAnaplastic Thyroid Cancershita febrianaNo ratings yet
- Lumenis Novus Varia Indications For Use As Requested by FdaDocument8 pagesLumenis Novus Varia Indications For Use As Requested by FdaM.r SadrshiraziNo ratings yet
- NCM 105 Rle Case 1 BasigDocument17 pagesNCM 105 Rle Case 1 BasigMaria Charis Anne IndananNo ratings yet
- Arterial Disease SurgicalDocument43 pagesArterial Disease SurgicalWahid SyedNo ratings yet
- Potter & Perry: Fundamentals of Nursing, 7 EditionDocument11 pagesPotter & Perry: Fundamentals of Nursing, 7 Editionmissy23pap100% (1)
- Nephrology MCQ PDFDocument7 pagesNephrology MCQ PDFMonica J Ortiz PereiraNo ratings yet
- Drug Bulletin: Antipsychotic MonitoringDocument4 pagesDrug Bulletin: Antipsychotic MonitoringMuhammad NaufalNo ratings yet
- What Causes COPD?Document4 pagesWhat Causes COPD?Adi PutraNo ratings yet
- Sources of DrugsDocument14 pagesSources of DrugsAjmal AftabNo ratings yet
- The Relationship of Chest X-Ray in COVID-19 Patients and Disease Severity in Arifin Achmad General Hospital RiauDocument8 pagesThe Relationship of Chest X-Ray in COVID-19 Patients and Disease Severity in Arifin Achmad General Hospital RiauHangga WingitNo ratings yet
- Pathology of The Male GUTDocument108 pagesPathology of The Male GUTHoque Mohammed Newaz ShorifulNo ratings yet
- Hepatic ComaDocument4 pagesHepatic ComaAshraf Abu-ainNo ratings yet
- Drug Study-Operating RoomDocument6 pagesDrug Study-Operating RoomkathzheinNo ratings yet
- Renal BiopsyDocument4 pagesRenal BiopsyDeshan AdikariNo ratings yet
- Lung Cancer Lecture Notes (Quick Summary)Document4 pagesLung Cancer Lecture Notes (Quick Summary)Ibrahim FoondunNo ratings yet
- Posttest. Renal DisordersDocument3 pagesPosttest. Renal Disordersjbagacay100% (3)
- Anat 51 To 92qDocument48 pagesAnat 51 To 92qMuhieddin GhosnNo ratings yet
- Systemic Infections From GiDocument10 pagesSystemic Infections From GiJake MillerNo ratings yet
- Surgery Questions by DR - PawanDocument8 pagesSurgery Questions by DR - PawanPawan KandhariNo ratings yet