You might also like
- PEWS3Document2 pagesPEWS3NissaNo ratings yet
- PEWS2Document2 pagesPEWS2NissaNo ratings yet
- Paediatric Vital Signs Chart: 12 Years: Medical Staff Modification To Early Warning Score (PEWS) TriggersDocument2 pagesPaediatric Vital Signs Chart: 12 Years: Medical Staff Modification To Early Warning Score (PEWS) TriggersKomang Adhi AmertajayaNo ratings yet
- GeneralDocument1 pageGeneralBunga AzaleaNo ratings yet
- CbclprofileDocument6 pagesCbclprofileAdina Bîrsan-MarianNo ratings yet
- Kylmäpros 270121Document6 pagesKylmäpros 270121wfhtw7xxf7No ratings yet
- Memento Mori Life CalendarDocument2 pagesMemento Mori Life CalendarMartín ParrucciNo ratings yet
- full-length-June-Diagnostic TestDocument51 pagesfull-length-June-Diagnostic TestVedant YadavNo ratings yet
- Question-and-Answer Service Student GuideDocument51 pagesQuestion-and-Answer Service Student GuideBri Min100% (2)
- The Journey and Application of Risk Forecasting in Orion: Presenter: Daniel Law - Asset Lifecycle EngineerDocument13 pagesThe Journey and Application of Risk Forecasting in Orion: Presenter: Daniel Law - Asset Lifecycle Engineergalangrisky234No ratings yet
- Head-Circumference BoysDocument1 pageHead-Circumference BoysSirawit KaewchaiyaNo ratings yet
- Ballard Score Calculator: CalculatorsDocument1 pageBallard Score Calculator: Calculatorsbazlin syabrinaNo ratings yet
- Scoring Guide For CVsUPDATEDDocument3 pagesScoring Guide For CVsUPDATEDAbubakar AliyuNo ratings yet
- Curvas 0-5 Anos - 5-10 AnosDocument12 pagesCurvas 0-5 Anos - 5-10 AnosLaís LimaNo ratings yet
- The Private Sector Financial Balance As A Predictor of Financial CrisesDocument12 pagesThe Private Sector Financial Balance As A Predictor of Financial CrisesIsaac GoldNo ratings yet
- Head Circumference-For-Age BOYS: Birth To 5 Years (Z-Scores)Document1 pageHead Circumference-For-Age BOYS: Birth To 5 Years (Z-Scores)nai4141No ratings yet
- Marketing Assignment FAS S2Document17 pagesMarketing Assignment FAS S2Vedashree RelkarNo ratings yet
- DMX2 0Document1 pageDMX2 0madjidstore9No ratings yet
- Biggs, Schlüter, Schoon - Principles For Building Resilience - CH 1-An Introduction To The ResilienceDocument31 pagesBiggs, Schlüter, Schoon - Principles For Building Resilience - CH 1-An Introduction To The ResilienceLoan LaurentNo ratings yet
- CHT Wfa Girls Z 5 10yearsDocument1 pageCHT Wfa Girls Z 5 10yearsJeane Irish EgotNo ratings yet
- Gráfico - Peso para Idade - Meninas de 5 A 10 Anos - Escore Z - OMSDocument1 pageGráfico - Peso para Idade - Meninas de 5 A 10 Anos - Escore Z - OMSMais1No ratings yet
- Market Share (Graphs)Document12 pagesMarket Share (Graphs)mohd sohel100% (2)
- Plan Mobilare Cu Cote-Apt.4 CamereDocument1 pagePlan Mobilare Cu Cote-Apt.4 CamereDany MelNo ratings yet
- Grain Size Distribution: Client Mbits Project Name Po1 Project Number Po1Document1 pageGrain Size Distribution: Client Mbits Project Name Po1 Project Number Po1Dileep K NambiarNo ratings yet
- GEM Series - En12845 Fire Fighting Booster Sets in Egypt, Technical Catalog Part 2Document66 pagesGEM Series - En12845 Fire Fighting Booster Sets in Egypt, Technical Catalog Part 2Rheoserve Industrial SolutionsNo ratings yet
- LC1D - DC PowerDocument4 pagesLC1D - DC Powermarijan_123No ratings yet
- Selection of Companies TORs For IT-ITeS Companies Lot4Document7 pagesSelection of Companies TORs For IT-ITeS Companies Lot4shaikhaman1No ratings yet
- LoBiancoT GraphingDocument3 pagesLoBiancoT GraphingSn CarbonelNo ratings yet
- Head Circumference-For-Age BOYS: Birth To 5 Years (Z-Scores)Document5 pagesHead Circumference-For-Age BOYS: Birth To 5 Years (Z-Scores)santhoshNo ratings yet
- PhillyforeDocument16 pagesPhillyforeapi-25887578No ratings yet
- Koordinasi Supply Chain: Program Peningkatan Kompetensi KaryawanDocument19 pagesKoordinasi Supply Chain: Program Peningkatan Kompetensi KaryawanBudhi SuwarsonoNo ratings yet
- Gráfico - Peso para Idade - Meninos de 5 A 10 Anos - Escore Z - OMSDocument1 pageGráfico - Peso para Idade - Meninos de 5 A 10 Anos - Escore Z - OMSMais1No ratings yet
- Who Weight-For-Age Boys 5 10yearsDocument1 pageWho Weight-For-Age Boys 5 10yearsAulia Rahman NasrunNo ratings yet
- Weight-For-Age BOYS: 5 To 10 Years (Z-Scores)Document1 pageWeight-For-Age BOYS: 5 To 10 Years (Z-Scores)MaysacamposmotaNo ratings yet
- Technical FlowpakDocument3 pagesTechnical FlowpakAmjad HussainNo ratings yet
- Trapped Fluid in Compressor Coupling SpacerDocument26 pagesTrapped Fluid in Compressor Coupling SpacerHamid JNo ratings yet
- Sustainable DietDocument7 pagesSustainable DietfrankowskaNo ratings yet
- RM Numerical DataDocument17 pagesRM Numerical DataPearlNo ratings yet
- Corte Transversal - pdf1Document1 pageCorte Transversal - pdf1NikerParionaFloressNo ratings yet
- Head Circumference-For-Age BOYS: Birth To 5 Years (Percentiles)Document1 pageHead Circumference-For-Age BOYS: Birth To 5 Years (Percentiles)febi novrizalNo ratings yet
- 2024 Estimates - Global Pepper Balance SheetDocument15 pages2024 Estimates - Global Pepper Balance SheetJasvinder SethiNo ratings yet
- Grain Size Distribution: Client Mbits Project Name P05 Project Number Po5Document1 pageGrain Size Distribution: Client Mbits Project Name P05 Project Number Po5Dileep K NambiarNo ratings yet
- Introduction To StatsDocument8 pagesIntroduction To StatsSaiNo ratings yet
- HPLC Teaching Assistant en v1.3Document951 pagesHPLC Teaching Assistant en v1.3Lluis Otero de MullerNo ratings yet
- Grandon Society Large GroupDocument5 pagesGrandon Society Large GroupRussell ThayerNo ratings yet
- 5 Pews ScottishDocument40 pages5 Pews ScottishKomang Adhi AmertajayaNo ratings yet
- Question-and-Answer Service Student GuideDocument16 pagesQuestion-and-Answer Service Student GuideRohan JacobNo ratings yet
- Kingdom Hearts Medley: KaythepianistDocument2 pagesKingdom Hearts Medley: KaythepianistAtodivariusNo ratings yet
- Projeto FinalDocument1 pageProjeto FinalVitória ElisaNo ratings yet
- Data Analysis Mutual FundDocument9 pagesData Analysis Mutual Fundjayswalhiralal899No ratings yet
- Pediatric Primary Care 6Th Edition Catherine E Burns Editor All ChapterDocument67 pagesPediatric Primary Care 6Th Edition Catherine E Burns Editor All Chaptermargie.lee200100% (7)
- Sushil KumatDocument33 pagesSushil Kumat123456789OOOOOONo ratings yet
- Dashcam Graphs by RamisDocument7 pagesDashcam Graphs by RamisMohsin JalilNo ratings yet
- Franklin COVID Profile Report 8.17.20Document2 pagesFranklin COVID Profile Report 8.17.20manager2738No ratings yet
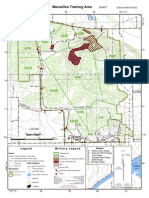
- MTC Map 1 To 25000Document1 pageMTC Map 1 To 25000bussens2012No ratings yet
- Sons 2Document2 pagesSons 2JosephNo ratings yet
- 0 - 5 Tahun - PDF Lingkar Kepala Menurut UsiaDocument1 page0 - 5 Tahun - PDF Lingkar Kepala Menurut UsiaGilang GidhanNo ratings yet
- WHO-CDC Print PDFDocument37 pagesWHO-CDC Print PDFRumaisha HasnahNo ratings yet
- Data OUtputDocument10 pagesData OUtputiyan morankNo ratings yet
- Meriem Chatti - RéférencesDocument22 pagesMeriem Chatti - RéférencesOussama SghaïerNo ratings yet
- Consumer Awareness or Disease Mongering - GlaxoSmithKline and The Restless Legs SyndromeDocument5 pagesConsumer Awareness or Disease Mongering - GlaxoSmithKline and The Restless Legs SyndromeonyebuchiannabelNo ratings yet
- Cefuroxime Drug StudyDocument4 pagesCefuroxime Drug StudyDona Jane BritosNo ratings yet
- Sgot & SGPTDocument2 pagesSgot & SGPT우영박No ratings yet
- Osteosarcoma and Its Variants Compressed PowerpointDocument126 pagesOsteosarcoma and Its Variants Compressed PowerpointSehrish SiddiqueNo ratings yet
- Common Health Problems Associated With AgingDocument7 pagesCommon Health Problems Associated With AgingAnjo AprueboNo ratings yet
- Patient Blepharitis LeafletDocument2 pagesPatient Blepharitis LeafletPrincess ErickaNo ratings yet
- Case 1 AbortionDocument18 pagesCase 1 AbortionEduard GarchitorenaNo ratings yet
- 2002, Vol.25, Issues 1, Psychiatry in The Medically IllDocument239 pages2002, Vol.25, Issues 1, Psychiatry in The Medically IllGonzalo Sepulveda EstayNo ratings yet
- Comparing Ultra-Hypofractionated Proton Versus Photon Therapy in Extremity Soft Tissue SarcomaDocument10 pagesComparing Ultra-Hypofractionated Proton Versus Photon Therapy in Extremity Soft Tissue SarcomaRaul Matute MartinNo ratings yet
- Causes and Risk Factors For Attention-Deficit Hyperactivity DisorderDocument8 pagesCauses and Risk Factors For Attention-Deficit Hyperactivity DisorderFranthesa LayloNo ratings yet
- Hemolytic AnemiaDocument99 pagesHemolytic AnemiaSagar Chandrakant Mhetre100% (3)
- Amniocentesis: Contact: Innoclazz Academy For Best Home Tutors in Bangalore, Hyderabad, Chennai, Mumbai and Pune WebsiteDocument14 pagesAmniocentesis: Contact: Innoclazz Academy For Best Home Tutors in Bangalore, Hyderabad, Chennai, Mumbai and Pune WebsiteInnoclazz AcademyNo ratings yet
- Gerontological Nursing 2021Document157 pagesGerontological Nursing 2021Andrew Isiah BonifacioNo ratings yet
- Online Practice Tests, Live Classes, Tutoring, Study Guides Q&A, Premium Content and MoreDocument112 pagesOnline Practice Tests, Live Classes, Tutoring, Study Guides Q&A, Premium Content and MoreYoAmoNYC100% (2)
- Physiotherapy in Geriatric Rehabilitation: PatientDocument3 pagesPhysiotherapy in Geriatric Rehabilitation: PatientGrace LNo ratings yet
- Apogeotropic Variant of Posterior Canal Benign Paroxysmal Positional VertigoDocument7 pagesApogeotropic Variant of Posterior Canal Benign Paroxysmal Positional VertigojorgepierreNo ratings yet
- Oncocytoma of The Nasal CavityDocument2 pagesOncocytoma of The Nasal CavityInes Camilla PutriNo ratings yet
- Syndrome of Inappropriate Vasopressin Sexretion (Siadh)Document22 pagesSyndrome of Inappropriate Vasopressin Sexretion (Siadh)Moni RethNo ratings yet
- Usos de Bite Blocks PDFDocument25 pagesUsos de Bite Blocks PDFNatasha RiveraNo ratings yet
- Pancreatic Pathology For The SurgeonDocument10 pagesPancreatic Pathology For The SurgeonSanjaya SenevirathneNo ratings yet
- Rheumatic FeverDocument26 pagesRheumatic FeverAhmed Ben Bella100% (2)
- 10 Topnotch Obstetrics Gynecology SuperExam1 PDFDocument84 pages10 Topnotch Obstetrics Gynecology SuperExam1 PDFvardhan100% (3)
- Lesson Plan Nephrotic SyndromeDocument9 pagesLesson Plan Nephrotic SyndromeEllen Angel50% (2)
- A Study of Ocular Abnormalities in Children With Cerebral PalsyDocument6 pagesA Study of Ocular Abnormalities in Children With Cerebral PalsySuvratNo ratings yet
- Recurrent Takotsubo CardiomyopathyDocument6 pagesRecurrent Takotsubo CardiomyopathyProdi S1- 1BNo ratings yet
- DrHur - Internal Meidcine 2014 KrokDocument135 pagesDrHur - Internal Meidcine 2014 Krokgaurav100% (1)
- Appendix 8 PDQ39 PDFDocument3 pagesAppendix 8 PDQ39 PDFdrrselvarajNo ratings yet
- Anxiety Depression QuestionnaireDocument2 pagesAnxiety Depression QuestionnairetatacrtNo ratings yet
- Pruritic Metastatic Crohn'sDocument3 pagesPruritic Metastatic Crohn'sHerald Scholarly Open AccessNo ratings yet