You might also like
- Etiology of Pelvic Organ ProlapseDocument9 pagesEtiology of Pelvic Organ ProlapseAlandey e TatianaNo ratings yet
- At-Home Workouts and Resources For Health and Fitness ProfessionalsDocument8 pagesAt-Home Workouts and Resources For Health and Fitness ProfessionalsNury QuintanarNo ratings yet
- BHW Reference ManualDocument116 pagesBHW Reference ManualGa B B Orlongan67% (3)
- Clinical Practice Guidelines in The Evaluation and Management of PCAPDocument38 pagesClinical Practice Guidelines in The Evaluation and Management of PCAPJames de Jesus86% (7)
- GynecologyDocument251 pagesGynecologyمحمد ابو مناضل الافينشNo ratings yet
- Maternal Health ServicesDocument24 pagesMaternal Health ServicesMuna Hassan MustafaNo ratings yet
- Health Teaching PlanDocument11 pagesHealth Teaching PlanVic Intia Paa100% (1)
- Adolecent Pregnancy, Elderly Primigravida, Grand Multipara IntroductionDocument3 pagesAdolecent Pregnancy, Elderly Primigravida, Grand Multipara IntroductionmercyNo ratings yet
- CHC - 2Document15 pagesCHC - 2Babita Dhruw75% (4)
- Associated Risk Factors of Placenta Previa A Matched Case Control StudyDocument4 pagesAssociated Risk Factors of Placenta Previa A Matched Case Control StudyFitri Nur DiniNo ratings yet
- Prevencion CesareaDocument19 pagesPrevencion CesareaNatalia MartínezNo ratings yet
- Background: Placenta Previa. Placenta Previa Covering The Entire CervicalDocument9 pagesBackground: Placenta Previa. Placenta Previa Covering The Entire CervicalOkto Sofyan HasanNo ratings yet
- Placenta Previa: View Media GalleryDocument7 pagesPlacenta Previa: View Media GalleryMargaret AssilasNo ratings yet
- Women's Health Care Physicians: Member Login Join Pay Dues Follow UsDocument24 pagesWomen's Health Care Physicians: Member Login Join Pay Dues Follow UsNazif Aiman IsmailNo ratings yet
- Placenta Previa - MedscapeDocument5 pagesPlacenta Previa - MedscapeAnonymous jh87ryNo ratings yet
- Maternal, Labor, Delivery, and Perinatal Outcomes Associated With Placental Abruption: A Systematic ReviewDocument23 pagesMaternal, Labor, Delivery, and Perinatal Outcomes Associated With Placental Abruption: A Systematic ReviewasfwegereNo ratings yet
- Elective Primary Cesarean Delivery: Sounding BoardDocument6 pagesElective Primary Cesarean Delivery: Sounding BoardNicole Grace VillegasNo ratings yet
- Breech Za NigeriaqDocument10 pagesBreech Za NigeriaqRendra Artha Ida BagusNo ratings yet
- Frey 2015Document2 pagesFrey 2015Anonymous YyLSRdNo ratings yet
- Ijrm 11 385Document6 pagesIjrm 11 385Obgyn Maret 2019No ratings yet
- Hemorragia y EmbrazoDocument6 pagesHemorragia y Embrazoana catalinaNo ratings yet
- Placental Abruption.Document6 pagesPlacental Abruption.indahNo ratings yet
- Maternal and Perinatal Outcome in Antepartum HemorrhageDocument5 pagesMaternal and Perinatal Outcome in Antepartum HemorrhagebayukolorNo ratings yet
- To Ignore or Not To Ignore Placental Calcifications On Prenatal Ultrasound: A Systematic Review and Meta-AnalysisDocument22 pagesTo Ignore or Not To Ignore Placental Calcifications On Prenatal Ultrasound: A Systematic Review and Meta-AnalysisMaulida HalimahNo ratings yet
- Placenta Accreta and The Risk of Adverse Maternal and Neonatal OutcomesDocument10 pagesPlacenta Accreta and The Risk of Adverse Maternal and Neonatal OutcomesAulia Putri ANo ratings yet
- Systematic Review Placenta Calcification and Fetal OutcomeDocument22 pagesSystematic Review Placenta Calcification and Fetal OutcomeRizka AdiNo ratings yet
- Journal (Preterm Labor)Document5 pagesJournal (Preterm Labor)Zhyraine Iraj D. CaluzaNo ratings yet
- BJMG 20 005 PDFDocument5 pagesBJMG 20 005 PDFRakka Fawwaz IlhamNo ratings yet
- Jurnal Obgyn 2018 2Document15 pagesJurnal Obgyn 2018 2aulNo ratings yet
- Placenta Previa PDFDocument15 pagesPlacenta Previa PDFDamaris GonzálezNo ratings yet
- Determinants and Obstetrics Outcome of Umbilical Cord Prolapse at University of Calabar Teaching Hospital, Calabar, NigeriaDocument6 pagesDeterminants and Obstetrics Outcome of Umbilical Cord Prolapse at University of Calabar Teaching Hospital, Calabar, NigeriaIOSRjournalNo ratings yet
- Silver 2015Document15 pagesSilver 2015Farlinda AlyaNo ratings yet
- Articulo 8Document15 pagesArticulo 8Monica ReyesNo ratings yet
- Is Fetal Growth Restriction Associated With A More Severe Maternal Phenotype in The Setting of Early Onset Pre-Eclampsia? A Retrospective StudyDocument6 pagesIs Fetal Growth Restriction Associated With A More Severe Maternal Phenotype in The Setting of Early Onset Pre-Eclampsia? A Retrospective StudyYessie ErNo ratings yet
- Postpartum HemorrhageDocument22 pagesPostpartum HemorrhageReynaldiReikyHadiwijayaNo ratings yet
- Article 262063-PrintDocument15 pagesArticle 262063-PrintAhsan AuliyaNo ratings yet
- Placenta PreviaDocument8 pagesPlacenta PreviaBj DuquesaNo ratings yet
- Chapter TwoDocument7 pagesChapter Twohanixasan2002No ratings yet
- The Relationship Between Hemoglobin and Hematocrit in The First Trimester of Pregnancy and The Incidence of PreeclampsiaDocument3 pagesThe Relationship Between Hemoglobin and Hematocrit in The First Trimester of Pregnancy and The Incidence of PreeclampsiaBaru Chandrasekhar RaoNo ratings yet
- The Placenta: Transcriptional, Epigenetic, and Physiological Integration During DevelopmentDocument10 pagesThe Placenta: Transcriptional, Epigenetic, and Physiological Integration During Developmentpam!!!!No ratings yet
- Term and Posterm PDFDocument7 pagesTerm and Posterm PDFRorschach VargasNo ratings yet
- Jurnal Placenta PreviaDocument9 pagesJurnal Placenta Previasheva25No ratings yet
- Risk factors for preeclampsia عبدالسلامDocument5 pagesRisk factors for preeclampsia عبدالسلامmqbljbr529No ratings yet
- Artigo 3Document7 pagesArtigo 3Cirineu NetoNo ratings yet
- Correlation Between Risk Factors and Pelvic Organ Prolapse in Gynecology Outpatient Clinic, Dr. Soetomo Hospital Surabaya, 2007 - 2011Document6 pagesCorrelation Between Risk Factors and Pelvic Organ Prolapse in Gynecology Outpatient Clinic, Dr. Soetomo Hospital Surabaya, 2007 - 2011AndivaNo ratings yet
- Assessment and Management of Bleeding in The First Trimester of PregnancyDocument9 pagesAssessment and Management of Bleeding in The First Trimester of PregnancyManuel MagañaNo ratings yet
- Comparative Study of Placental Cytoarchitecture in Mild and Severe Hypertensive Disorders Occurring During Pregnancy.Document54 pagesComparative Study of Placental Cytoarchitecture in Mild and Severe Hypertensive Disorders Occurring During Pregnancy.prasadNo ratings yet
- Placenta Previa: ObjectivesDocument6 pagesPlacenta Previa: ObjectivesAllan Lyndon LariosNo ratings yet
- Indication For CsDocument20 pagesIndication For CsSandiNo ratings yet
- Safe Prevention of The Primary CS DeliveryDocument19 pagesSafe Prevention of The Primary CS DeliveryCleoGomezNo ratings yet
- Sutura CesareasDocument10 pagesSutura CesareasalexNo ratings yet
- Article PDFDocument10 pagesArticle PDFGilang Hadi FNo ratings yet
- A 5-Year Review of Pattern of Placenta Previa in Ilorin, NigeriaDocument6 pagesA 5-Year Review of Pattern of Placenta Previa in Ilorin, Nigeriaamalia chairunnisaNo ratings yet
- Threatened Abortion A Risk Factor For Poor PregnanDocument8 pagesThreatened Abortion A Risk Factor For Poor PregnanBaiiqDelaYulianingtyasNo ratings yet
- Jurnal Abrupsio PlasentaDocument13 pagesJurnal Abrupsio Plasentaperussi pranadiptaNo ratings yet
- Placenta PreviaDocument5 pagesPlacenta PreviaKuro HanabusaNo ratings yet
- Effect of Placenta Previa On Fetal Growth: ObstetricsDocument5 pagesEffect of Placenta Previa On Fetal Growth: ObstetricsAnonymous 4OpLzzt6No ratings yet
- Neonatal and Maternal Complications of Placenta Praevia and Its Risk Factors in Tikur Anbessa Specialized and Gandhi Memorial Hospitals. Unmatched Case-Control StudyDocument10 pagesNeonatal and Maternal Complications of Placenta Praevia and Its Risk Factors in Tikur Anbessa Specialized and Gandhi Memorial Hospitals. Unmatched Case-Control StudyLarassati YayaNo ratings yet
- Practice Bulletin: Premature Rupture of MembranesDocument13 pagesPractice Bulletin: Premature Rupture of MembranesMarcela Catalina Fandiño VargasNo ratings yet
- Age As The Risk Factor That Affected The Increased Degree of Uterine ProlapseDocument5 pagesAge As The Risk Factor That Affected The Increased Degree of Uterine Prolapsehypebeast dopeNo ratings yet
- Threatened MisscariageDocument16 pagesThreatened MisscariageDinda BasriNo ratings yet
- AbruptionDocument13 pagesAbruptionAnghelo Aldair Velásquez CarrilloNo ratings yet
- EctopicwDocument9 pagesEctopicwdrnunungNo ratings yet
- The Relationship Between Hemoglobin and Hematocrit in The First and Second Trimester of Pregnancy and The Incidence of PreeclampsiaDocument3 pagesThe Relationship Between Hemoglobin and Hematocrit in The First and Second Trimester of Pregnancy and The Incidence of PreeclampsiaBaru Chandrasekhar RaoNo ratings yet
- Postpartum Hemorrhage (PPH) : BackgroundDocument43 pagesPostpartum Hemorrhage (PPH) : BackgroundMuhammad Haris FirdausNo ratings yet
- AbruptionDocument13 pagesAbruptionMauricio Lopez MejiaNo ratings yet
- Knowledge, Attitudes, and Perceptions of Preeclampsia Among First-Generation Nigerian Women in the United StatesFrom EverandKnowledge, Attitudes, and Perceptions of Preeclampsia Among First-Generation Nigerian Women in the United StatesNo ratings yet
- Diminished Ovarian Reserve and Assisted Reproductive Technologies: Current Research and Clinical ManagementFrom EverandDiminished Ovarian Reserve and Assisted Reproductive Technologies: Current Research and Clinical ManagementOrhan BukulmezNo ratings yet
- Leptospirosis FactsDocument1 pageLeptospirosis FactsZenitha FauziaNo ratings yet
- Ebp Final PaperDocument40 pagesEbp Final Paperapi-557314921No ratings yet
- Environmental SanitationDocument46 pagesEnvironmental SanitationggalicinaoNo ratings yet
- SmokingDocument116 pagesSmokingyuy21No ratings yet
- Updated NCCN Guidelines For Cervical Cancer.22Document2 pagesUpdated NCCN Guidelines For Cervical Cancer.22Hari NugrohoNo ratings yet
- Sf2 2015 Grade 10 CopernicusDocument19 pagesSf2 2015 Grade 10 CopernicusGab IlaganNo ratings yet
- Table 2: Summary of WHO Position Papers - Recommended Routine Immunizations For ChildrenDocument11 pagesTable 2: Summary of WHO Position Papers - Recommended Routine Immunizations For ChildrenNehaNo ratings yet
- COVID-19 Technical Briefing - Friday April 4 2020Document17 pagesCOVID-19 Technical Briefing - Friday April 4 2020james1572100% (3)
- Resume For FulbrightDocument5 pagesResume For Fulbrightmango chaunsaNo ratings yet
- Sanitation and Hygiene Promotion Programming GuidanceDocument94 pagesSanitation and Hygiene Promotion Programming GuidancevanasiareyesNo ratings yet
- Health Policy Analysis: A Simple Tool For Policy MakersDocument6 pagesHealth Policy Analysis: A Simple Tool For Policy Makerspang downloadNo ratings yet
- UntitledDocument1 pageUntitledTerence SalamatNo ratings yet
- Conn With Chomicz Et Al 2016 BioMed Research International Special Issue Newly Emerging Parasitic ThreatsDocument74 pagesConn With Chomicz Et Al 2016 BioMed Research International Special Issue Newly Emerging Parasitic ThreatsAnonymous 6OPLC9UNo ratings yet
- Nutrition (Healthy Eating and Food Borne)Document12 pagesNutrition (Healthy Eating and Food Borne)airene olivaNo ratings yet
- Eo 2021 004 Referral Psychosocial ServicesDocument2 pagesEo 2021 004 Referral Psychosocial ServicesWaldz Renales100% (1)
- 2020 Rak Sanit SWDocument19 pages2020 Rak Sanit SWHatem TNo ratings yet
- Cancer Cervix: BY Ahmed Magdy ElmohandesDocument34 pagesCancer Cervix: BY Ahmed Magdy ElmohandesAhmed ElmohandesNo ratings yet
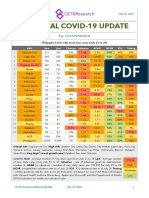
- National COVID-19 Update by Octa Research On July 30, 2021Document2 pagesNational COVID-19 Update by Octa Research On July 30, 2021RapplerNo ratings yet
- Nursing Manangement and Administration Assignment ON Standard Protocol of The UnitDocument9 pagesNursing Manangement and Administration Assignment ON Standard Protocol of The UnitNisha MwlzNo ratings yet
- 15b. FANC - Focused Antenatal Care - Koros E.KDocument71 pages15b. FANC - Focused Antenatal Care - Koros E.KMercy KeruboNo ratings yet
- Pengoperasian Compressor Ingersoll Rand P90CWIRDocument24 pagesPengoperasian Compressor Ingersoll Rand P90CWIRelvandiNo ratings yet
- Antenatal Care During Pregnancy PamphletDocument2 pagesAntenatal Care During Pregnancy PamphletKatherina NaguiNo ratings yet