Professional Documents
Culture Documents
Oncologic Emergencies and Urgencies A Comprehensive Review
Uploaded by
Marco Antonio Morales GonzálezOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Oncologic Emergencies and Urgencies A Comprehensive Review
Uploaded by
Marco Antonio Morales GonzálezCopyright:
Available Formats
CA CANCER J CLIN 2022;0:1–24
Oncologic emergencies and urgencies:
A comprehensive review
1
Bonnie E. Gould Rothberg, MD, PhD, MPH ; Tammie E. Quest, MD2; Sai-Ching J. Yeung, MD, PhD3; Lorraine C. Pelosof, MD, PhD4;
David E. Gerber, MD ; Justin A. Seltzer, MD6; Jason J. Bischof, MD7; Charles R. Thomas, Jr, MD8; Nausheen Akhter, MD9;
5
Mira Mamtani, MD, MSEd10; Robin E. Stutman, MD11; Christopher W. Baugh, MD, MBA12;
Venkataraman Anantharaman, MBBS, FRCP Edin.13; Nicholas R. Pettit, DO, PhD14; Adam D. Klotz, MD11; Michael A. Gibbs, MD15;
Demetrios N. Kyriacou, MD, PhD16,17
1
Yale Cancer Center Innovations
Laboratory, Yale Comprehensive Cancer Abstract: Patients with advanced cancer generate 4 million visits annually to emer-
Center, New Haven, Connecticut;
2 gency departments (EDs) and other dedicated, high-acuity oncology urgent care
Department of Emergency Medicine,
Emory University, Atlanta, Georgia; centers. Because of both the increasing complexity of systemic treatments overall
3
Department of Emergency Medicine, and the higher rates of active therapy in the geriatric population, many patients expe-
The University of Texas MD Anderson riencing acute decompensations are frail and acutely ill. This article comprehensively
Cancer Center, Houston, Texas; reviews the spectrum of oncologic emergencies and urgencies typically encountered
4
Office of Oncologic Diseases, US Food in acute care settings. Presentation, underlying etiology, and up-to-date clinical path-
and Drug Administration, Silver Spring, ways are discussed. Criteria for either a safe discharge to home or a transition of
Maryland; 5 Division of Hematology-
care to the inpatient oncology hospitalist team are emphasized. This review extends
Oncology, Harold C. Simmons
Comprehensive Cancer Center, University beyond familiar conditions such as febrile neutropenia, hypercalcemia, tumor lysis
of Texas Southwestern Medical School, syndrome, malignant spinal cord compression, mechanical bowel obstruction, and
Dallas, Texas; 6 Department of Emergency breakthrough pain crises to include a broader spectrum of topics encompassing the
Medicine, University of California syndrome of inappropriate antidiuretic hormone secretion, venous thromboembolism
San Diego, San Diego, California; and malignant effusions, as well as chemotherapy-induced mucositis, cardiomyopa-
7
Department of Emergency Medicine,
thy, nausea, vomiting, and diarrhea. Emergent and urgent complications associated
The Ohio State University Wexner
Medical Center, Columbus, Ohio;
with targeted therapeutics, including small molecules, naked and drug-conjugated
8
Department of Radiation monoclonal antibodies, as well as immune checkpoint inhibitors and chimeric an-
Oncology, Geisel School of Medicine tigen receptor T-cells, are summarized. Finally, strategies for facilitating same-day
at Dartmouth, Norris Cotton Cancer direct admission to hospice from the ED are discussed. This article not only can
Center, Lebanon, New Hampshire; serve as a point-of-care reference for the ED physician but also can assist outpatient
9
Department of Medicine, Division of oncologists as well as inpatient hospitalists in coordinating care around the ED visit.
Cardiology, Northwestern University
Feinberg School of Medicine, Chicago,
Illinois; 10 Department of Emergency
Keywords: emergency medicine, hematology/medical oncology, internal medicine,
Medicine, University of Pennsylvania palliative care
Perelman School of Medicine,
Philadelphia, Pennsylvania;
11
Department of Medicine, Division of
Urgent Care Services, Memorial Sloan
Kettering Cancer Center, New York,
New York; 12 Department of Emergency Introduction
Medicine, Brigham and Women’s There are currently 16 million Americans living with cancer who account for
Hospital, Harvard Medical School,
approximately 4 million visits to emergency departments (EDs) each year.1 Patients
Boston, Massachusetts;
13
Department of Emergency with advanced cancer, especially those older than 65 years, exhibit a comparatively
Medicine, Singapore General Hospital, high frailty index characterized by the prevalence of disability, multiple medical
SingHealth Duke–National University of comorbidities, and ensuing polypharmacy such that the level of acuity among pa-
Singapore Academic Medical Center,
Singapore, Singapore; 14 Department of tients with cancer who are seeking emergency care is substantial.2 As oncology care
Emergency Medicine, Indiana University delivery has largely shifted to the outpatient clinic, complications are most likely
School of Medicine, Indianapolis, Indiana;
15
to arise outside of the hospital to require a separate acute care visit.3 These emer-
Department of Emergency Medicine,
Atrium Health-Carolinas Medical Center,
gencies represent a wide spectrum of disorders resulting from initial manifestations
Charlotte, North Carolina; of malignancy, progression of known disease, recurrence of a previous cancer, and
16
Department of Emergency Medicine, adverse effects from therapy, and some can be life-threatening. Although growing
Northwestern University Feinberg School
numbers of large community oncology practices and tertiary cancer centers have
of Medicine, Chicago, Illinois;
17
Department of Preventive established dedicated, high-acuity, same-day oncology urgent care centers, many
Medicine, Northwestern University patients still require general ED care for acute symptom management.4,5 Here, we
Feinberg School of Medicine, Chicago, present a comprehensive review of the clinical aspects of oncologic urgencies and
Illinois.
VOLUME 0 | NUMBER 0 | MONTH 2022 1
Oncologic emergencies and urgencies
emergencies, including sections discussing paraneoplas- Table 1 enumerates 15 common primary cancers frequently
tic syndromes, structural complications, and adverse events diagnosed in the ED7 along with their expected number of
associated with chemotherapy, radiotherapy, and targeted new cases in 2021, 5-year survival rates when diagnosed at
therapies, with the latter including each of small-molecule, advanced stage, and presenting signs and symptoms likely
monoclonal antibody, and cell-based therapeutics. We also encountered in the ED.11-14
include sections that discuss the management of previously
undiagnosed cancers that present emergently, pain crisis, and Paraneoplastic Syndromes
end-of-life care in the ED as well as discuss areas of future Paraneoplastic syndromes occur in up to 15% of patients
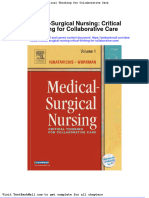
research (Fig. 1). with cancer. The vast majority of paraneoplastic syndromes
are endocrine-mediated and involve the secretion of bioac-
Cancer Presentation as an Emergent Diagnosis tive substances. Syndrome of inappropriate antidiuretic hor-
Emergently diagnosed cancers account for 11% to 29% of mone (SIADH) is a hallmark of small cell lung cancer with
newly diagnosed cancers and are associated with lower 1- 10% to 15% of patients affected and otherwise is most com-
year survival rates, increased hospitalization rates, and poorer monly observed across a broad spectrum of aerodigestive tract
quality of life compared with cancers diagnosed during rou- tumors, in particular nonsmall cell lung cancer, as well as in
tine primary care.6 Lower socioeconomic status, older age, breast cancer and lymphomas.15 SIADH can also arise as a
race, underlying comorbidities, and, depending on the spe- physiologic response to extreme cancer pain. Eight percent
cific cancer, sex correlate with increased prevalence of ED- of patients with cancer develop paraneoplastic hypercalcemia
based cancer diagnoses.7 Decreased access to primary care because of tumor-based parathyroid hormone-related protein
and established screening schedules as well as more frequent secretion. This is most frequently observed in squamous cell
use of the ED for urgent care likely contribute.8 Thirty per- cancers, renal cell cancer, gynecologic malignancies, breast
cent of cancers that present emergently will already demon- cancer, and some lymphomas.16 Secretion of ectopic vitamin
strate distant metastases compared with 14% of electively D or parathyroid hormone rarely occurs. Hypercalcemia can
diagnosed cancers.9 Even among cancers for which robust, additionally present with local osteolytic metastases, such as
validated screening is available, those diagnosed as emer- in breast cancer and multiple myeloma, accounting for 20%
gencies are more likely to be higher grade and have arisen of malignancy-related hypercalcemia. Ectopic adrenocortico-
de novo between screening intervals.10 The most common tropic hormone syndrome is rare and difficult to treat. Most
emergently diagnosed malignancies are those in which commonly observed in small cell lung cancer (1%-6% of
patients present either with nonspecific symptoms (eg, cases) and bronchial carcinoids (1% of all cases), it can present
intra-abdominal malignancies that present with diffuse gas- in other tumors with neuroendocrine differentiation such as
trointestinal discomfort) or with minimal symptoms until a small cell prostate tumors.17,18 Up to 40% of upper gastro-
dramatic event occurs (eg, generalized seizure as the sentinel intestinal neuroendocrine tumors produce a broad spectrum
event for primary brain tumor or new cerebral metastases).6 of paraneoplastic syndromes, each determined according to
Corresponding Author: Bonnie E. Gould Rothberg, MD, PhD, MPH, Yale Cancer Center Innovations Laboratory, Yale Comprehensive Cancer Center, 35 Park Street
15th Floor, New Haven, CT 06510 (bonnie.gouldrothberg@gmail.com).
DISCLOSURES: No external funding sources were used to support the writing of this article. Bonnie E. Gould Rothberg reports stock or stock options in Butterfly
Networks Inc, Quantum Si, Hyperfine Research, AI Therapeutics, Detect Labs, Tesseract, Protein Evolution Inc, and Electric Futures outside the submitted work; in
addition, her children have been employed by 4 Catalyzer; her spouse has a leadership or fiduciary role in Butterfly Networks Inc, Quantum Si, Hyperfine Research,
AI Therapeutics, Detect Labs, and Tesseract; has patents planned, issued, or pending at ThermoFisher, Butterfly Networks Inc, Quantum Si, Hyperfine Research,
AI Therapeutics, Detect Labs, and Tesseract; and owns stock or stock options in Butterfly Networks Inc, Quantum Si, Hyperfine Research, AI Therapeutics,
Detect Labs, Tesseract, Protein Evolution Inc, Electric Futures, AbbVie, Amgen, Biocryst Pharma, Gilead, Regeneron, and Roche Holdings. Sai-Ching J. Yeung
reports research funding from Bausch Health, Bristol-Myers Squibb, and DepoMed, Inc; personal fees from Celgene, Inc; and honoraria from Medscape outside
the submitted work. David E. Gerber reports institutional grants from AstraZeneca, BerGenBio ASA, Karyopharm Pharmaceuticals, and Novocure; personal fees
from Adjuvant Genomics, Regeneron Pharmaceuticals, Catalyst Pharmaceuticals, Sanofi, BeiGene LtD, Mirati Therapeutics Inc, and Janssen Scientific Affairs LLC;
royalties from Oxford University Press; participation on a data safety monitoring board or advisory board for Janssen Pharmaceuticals, Regeneron, and Sanofi
Aventis; and stock ownership in Gilead all outside the submitted work. Justin A. Seltzer reports long-term stock ownership in Pfizer, Inc, outside the submitted
work and is a PEER Section Editor for the American College of Emergency Physicians. Charles R. Thomas, Jr, is Deputy Editor of JAMA Oncology and CA: A Cancer
Journal for Clinicians. Christopher W. Baugh reports grants/research support from Visby Medical, Inc; personal fees from AcelRx Pharmaceuticals, Inc, Lucia Health
Guidelines, LLC, Nabriva Therapeutics, Roche Diagnostics, and Salix Pharmaceuticals; and honoraria from Roche Diagnostics all outside the submitted work.
Demetrios N. Kyriacou reports personal fees from Wellstat Therapeutics, Genetesis, and Remagine Ventures outside the submitted work. The remaining authors
report no conflicts of interest.
The views contained in this article represent those of the authors and not necessarily those of the US Food and Drug Administration.
CA Cancer J Clin 2022;0:2-24 © 2022 The Authors. CA: A Cancer Journal for Clinicians published by Wiley Periodicals LLC on behalf of American Cancer
Society. This is an open access article under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs License, which permits use and
distribution in any medium, provided the original work is properly cited, the use is non-commercial and no modifications or adaptations are made.
doi: 10.3322/caac.21727. Available online at cacancerjournal.com
2 CA: A Cancer Journal for Clinicians
CA CANCER J CLIN 2022;0:1–24
FIGURE 1. Spectrum of Oncologic Urgencies and Emergencies. Oncologic emergencies can be caused by either the malignancy itself or the applied
treatments. Disease-based emergencies include those precipitated by paraneoplastic syndromes or because of structurally based complications that arise
from compressive, expansive, space-occupying, or erosive effects of the malignancy. Emergent de novo presentations of previously undiagnosed cancers also
contribute. At the treatment level, complications can be subdivided according to systemic, generally cytotoxic chemotherapies; radiotherapy; and the newer
classes of small-molecule, antibody-based, and cellular targeted therapies as well as immunotherapeutics. Finally, both pain and palliative care reflect the
convergence of both cancer-related and treatment-related adverse events and require emergent consideration throughout the disease trajectory to culminate
in addressing end of life and goals of care in the emergency care setting.
its secreted hormone. Insulinomas form the largest subset of antibodies; <1%)36 are most commonly observed although
functional pancreatic neuroendocrine tumors, representing case reports have been noted in other malignancies. Because
50% of all such lesions, with gastrinomas occurring in 35%. these rare neurologic conditions may be the first sign of an
The remaining 15% are comprised of a mixture of glucagono- occult malignancy, evaluation must extend beyond a standard
mas, somatostatinomas, vasoactive intestinal peptide- omas neurologic workup to include serologic testing of both the pe-
and pancreatic polypeptide-omas, each producing a unique ripheral blood and the cerebrospinal fluid for onconeural au-
metabolic derangement that requires appropriate electrolyte toantibodies. If found, these should prompt a thorough search
and nutritional repletion.19 Bronchopulmonary and jejuno- for an underlying tumor.37 At the same time, onconeural an-
ileal carcinoids arise from enterochromaffin cells and with tibodies are neither sensitive nor specific because only 60%
a subset being functional tumors that secrete serotonin and of Lambert–Eaton myasthenic syndrome cases and <25%
other vasogenic amines. Carcinoid syndrome only occurs when of dermatomyositis cases are paraneoplastic.38,39 Immune
monoamines are injected into the systemic circulation, either modulation is the mainstay of therapy and includes cortico-
directly through the pulmonary circulation or from hepatic steroids, corticosteroid-sparing agents like cyclophosphamide,
or retroperitoneal metastases of the bowel lesions.20 Table 2 anti-CD20 monoclonal antibodies, intravenous immunoglob-
describes the presentations and management strategies of the ulins, and plasmapheresis.40,41 Acetylcholinesterase inhibitors
most common endocrine paraneoplastic syndromes.19,21-32 for myasthenia gravis and potassium channel blockers for
Humoral paraneoplastic syndromes result when an im- Lambert–Eaton myasthenic syndrome may be useful.
mune response occurs to tumor antigens that also yields au-
toantibodies against normal cellular components to trigger
corresponding autoimmune syndromes. Autoimmune para- Cancer-Related Structural Complications
neoplasias are altogether rare, affecting <1% of patients with Major oncologic structural complications are related to pro-
cancer, and most commonly present as neurologic, rheumato- voked impingement of adjacent end organs through external
logic, and dermatologic syndromes. Thymomas causing myas- compression, internal expansion, or space occupation as well
thenia gravis and myositis (antiacetylcholine receptor, antititin, as erosion through mucosae by the primary tumor or its me-
antiryanodine receptor antibodies; 50% of cases),33 small cell tastases. Although these complications can be the initial pre-
lung cancer causing paraneoplastic cerebellar degeneration senting symptom, many occur in the setting of progression
(anti-Hu antibodies; 5%-15%),34 Hodgkin and non-Hodgkin of disease or as a consequence of treatment (Table 3).42-69
lymphomas causing a spectrum of central or peripheral nervous Vascular complications include venous thromboembolism
system and neuromuscular junction syndromes (multiple35; (VTE), superior vena cava syndrome, carotid blowout syn-
1%), and testicular cancers causing encephalitis (anti-Ma2 drome, pulmonary hemorrhage, and gastrointestinal bleeding.
VOLUME 0 | NUMBER 0 | MONTH 2022 3
Oncologic emergencies and urgencies
TABLE 1. Fifteen Common Cancers Frequently Diagnosed as Emergencies and Associated Typical Presenting Signs and
Symptoms
5-Y RELATIVE SURVIVAL FOR
% CASES DIAGNOSED NO. OF CASES EXPECTED CANCERS DIAGNOSED AT TYPICAL EMERGENT SIGNS AND
CANCER TYPE EMERGENTLYa IN US, 2021b ADVANCED STAGE: 2021,% SYMPTOMS
Acute myelogenous 31.0 20,240 26.0 (adults)c Pancytopenias with or without blasts on
leukemia peripheral smear, mucosal bleeding,
bruising, petechiae, bone pain, fatigue.
Acute lymphocytic 28.9 5690 38.0 (adults)c
leukemia
Chronic myelogenous 26.4 9110 72.0c Extreme granulocytosis with or without
leukemia blasts, tumor lysis syndrome, throm-
botic events after leukostasis, fatigue.
Multiple myeloma 24.2 34,920 54.0c Hypercalcemia, diffuse bony achiness,
acute kidney injury, hyperviscosity,
spinal cord compression.
Lymphoma (Hodgkin and 26.0 90,390 66.0b Lymphadenopathy, fever, night sweats,
non-Hodgkin) weight loss anorexia, seizures (CNS
lymphoma), visceral organ obstruction.
Esophageal cancer 26.3 19,260 5.0b Hematemesis, anorexia, weight loss,
midepigastric pain, dysphagia to liquids
Stomach cancer 24.7 26,560 38.0d
and solids, odynophagia, vomiting
without nausea.
Pancreatic cancer 30.9 60,430 3.0b Painless jaundice, ascites, pruritus,
anorexia, weight loss, epigastric pain,
Gallbladder/liver/biliary 27.8 54,210 3.0b
steatorrhea, back pain.
cancer
Colon cancer 27.2 104,270 14.0b Iron deficiency, rectal bleeding, change
in bowel habits, abdominal pain.
Cancer of unknown 26.3 32,880 11.0 at 1 ye General malaise, fatigue, focal discom-
primary fort that maps to the anatomic location
of the mass.
Ovarian cancer 28.5 21,410 30.0b Bloating, ascites, lower abdominal
pain, flank pain, lower extremity deep
venous thrombosis.
Renal cancer 21.0 76,080 13.0b Painless hematuria, flank pain.
b
Bladder cancer 20.2 83,730 6.0 Acute kidney injury (because of ureteral
obstruction), irritation with voiding,
urinary frequency, and urgency.
Lung cancer 20.9 235,760 6.0b Cough, dyspnea, chest pain, hemoptysis.
Abbreviation: CNS, central nervous system.
a
Data from Herbert 2019.7
b
Data from Seigel 2021.11
c
Data from American Society of Clinical Oncology 2021.12
d
Data from Kao 2019.13
e
Data from Lee & Sanoff 2020.14
From 2% to 15% of patients with cancer, especially those and pericardial effusions, intracranial bleeding, seizures, and
with aerodigestive and genitourinary cancers, develop VTE death.73 The intercalation of tumor tissue with the struc-
(15-fold greater than the general population) to represent a tural matrix of large-caliber blood vessels risks significant
significant cause of associated morbidity and mortality.70,71 and potentially catastrophic hemorrhage after tumor necro-
Recurrent VTE occurs in 4% to 6% of patients after comple- sis or treatment-based erosion of the vascular wall. Carotid
tion of initial therapy.72 Superior vena cava syndrome results blowout syndrome (CBO) is an infrequent consequence of
from partial or complete obstruction of blood return from the either postsurgical wound breakdown or reirradiation of re-
head and neck to the right heart either by mechanical com- current head and neck cancer.74 Patients with impending
pression or by thromboembolic occlusion of the superior vena CBO who present with a self-resolving sentinel hemorrhage
cava, and most cases are attributed to regionally advanced require prompt referral to vascular surgeons. Acute CBO is
lung cancer and non-Hodgkin B-cell lymphoma with the usually fatal. Pulmonary hemorrhage can result from either
subsequent risk for edema of the brain and trachea, pleural radiotherapy-driven erosion of the pulmonary vasculature or
4 CA: A Cancer Journal for Clinicians
CA CANCER J CLIN 2022;0:1–24
TABLE 2. Paraneoplastic Syndromes: Common Presentations and Management Strategies
SYNDROME PRESENTATION MANAGEMENT
Syndrome of inappropri- • Urine osmolarity >100 mOsm coincident with euvolemic hypo- • In the ED, symptomatic hyponatremia requires 100 mL 3%
ate antidiuretic hormone tonic hyponatremia. normal saline bolus to acutely raise serum sodium by 2-3
(SIADH) • Corresponding serum sodium levels: mEq/L.
◦ Mild: 130 mEq/dL –134 mEq/dL • Total increase of serum sodium by no more than 4-6 mEq/L
◦ Moderate: 125 mEq/dL –129 mEq/dL in 24 hrs to avoid central pontine myelinolysis.
◦ Severe: <125 mEq/dL (Ellison & Berl21).
• Acute hyponatremia associated with headaches and neurocogni- • Free water restriction and sodium chloride tablets are
tive slowing. preferred for correcting chronic hyponatremia.
• Severe hyponatremia can be associated with seizures and death. • Correction of hyponatremia is usually necessary prior to
• Must be distinguished from hypovolemic hyponatremia due to initiating systemic therapy.
excessive gastrointestinal losses where urine osmolarity >300
mOsm but urine sodium < 20 mEq/L. (Raftopoulos 201722)
Hypercalcemia • Corresponding serum calcium levels: • Immediate aggressive intravenous hydration with normal
◦ Mild: 10.5 mg/dL –11.9 mg/dL saline, typically 1-2 L in the first hour followed by 2 L at
◦ Moderate: 12.0 mg/dL –13.9 mg/dL 200 mL/hr with close monitoring of volume status.
◦ Severe: ≥14.0 mg/dL • Early intravenous bisphosphonate administration (most
• In patients with hypoalbuminemia, observed serum calcium must commonly zolendronic acid). (Stewart 200523)
be further increased by 0.8*(4.0 –serum albumin) mg/dL. • Supplemental calcitonin can be administered during the
• Presents with altered mental status, generalized muscle weakness first 48 hours while the bisphosphonate is not yet at peak
and constipation due to generalized slowing of central, peripheral efficacy. (Khan 202124)
and autonomic nervous systems. • Denosumab (monoclonal antibody inhibitor of osteoclast
• Dehydration with ensuing acute kidney injury. activity) is alternatively administered in bisphosphonate-
• Urolithiasis can be observed with subacute presentations. refractory cases. (Fizazi 201125)
• Loop diuretics are generally now avoided as they can
exacerbate hypercalcemia and kidney injury in inadequately
hydrated patients. (LeGrand 200826)
Ectopic ACTH Syndrome • Hypertensive urgency/emergency. • Acute management of electrolyte disturbances and hyper-
• Hypokalemia and associated muscle weakness. tensive crisis.
• Generalized edema. (Fanous 202028) • Ketoconazole and metyrapone, agents that inhibit steroido-
genesis are often used. (Toivanen 202127)
Insulinoma • Fasting hypoglycemia in the absence of diabetes associated with • Oral and parenteral dextrose to maintain glucose levels.
diaphoresis, anxiety and altered mental status. • Diazoxide or streptozocin can inhibit insulin secretion from
β-islet cells. (Giannis 202029)
Gastrinoma • Extensive and pervasive peptic ulcers. • Proton pump inhibitors or histamine-2 receptor blockers,
initially at maximal twice-daily parenteral dosing. (Krampitz
& Norton 201330)
Carcinoid syndrome • Acute watery diarrhea, flushing, bronchospasm, hypotension from • Definitive therapy requires complete surgical resection.
excess serotonin secretion. • When curative-intent surgery is not possible, systemic
• Elevated urinary hydroxy-indoleacetic acid. therapy using long-acting somatostatin receptor inhibitors,
• Right heart disease including valvular compromise. (Oronsky peptide receptor radioligand therapy or hepatic artery
201719) embolization is performed. (Tella 202131)
• Niacin deficiency and hypoproteinemia from preferential tryptophan • Antidiarrheals, bronchodilators and vasoconstrictors can
diversion towards serotonin production. (Castiello & Lynch 197232) provide acute symptomatic relief.
necrosis of a large tumor, most frequently squamous cell car- also develop if increased intracranial pressure is not promptly
cinoma, with high morbidity and mortality owing to interfer- identified.77 Malignant spinal cord compression occurs in 20%
ence with alveolar gas exchange.75 Gastrointestinal bleeding of patients with spinal metastases and is most commonly as-
is most frequent with either erosive gastrointestinal tumors or sociated with breast, lung, prostate, and kidney cancers as well
the concurrent use of anticoagulants. as lymphoma and multiple myeloma.78 This occurs either by
Neurologic compromise can arise from tumor mass effect hematogenous spread into a vertebral-body mass, by patho-
on the brain or spinal cord. Increased intracranial pressure logic fractures resulting in epidural compression, or by direct
results from vasogenic edema associated with primary brain tumor extension into the vertebral column. Compression of
tumors, discrete foci of intraparenchymal solid tumor metas- the thecal sac and epidural venous plexus precipitates va-
tases, disseminated leptomeningeal metastases or postradia- sogenic edema of the white matter and demyelination.79
tion necrosis of previously treated lesions which then critically Major viscus obstruction in the thorax, abdomen, and
exceed the capacity of the nonexpendable cranium or precip- pelvis results from primary tumor- derived endoluminal
itate hydrocephalus.76 The most immediate emergent threat filling defects or external compression from either solid
is a herniation syndrome. Irreversible neurologic deficits can tumor regional disease or lymphomas. Overall, management
VOLUME 0 | NUMBER 0 | MONTH 2022 5
Oncologic emergencies and urgencies
TABLE 3. Cancer-Related Structural Complications: Common Presentations and Management Strategies
SYNDROME PRESENTATION MANAGEMENT
Vascular complications
Venous thromboembolism • Chief complaints of shortness of breath, unilateral leg • Computed tomographic (CT) angiography of the chest is the
swelling, or reduced oxygenation on pulse oximetry. definitive study because it not only can rule out other processes
but also can confirm right ventricular strain.
• D-dimer levels are not informative because they can • When IV contrast is contraindicated, a ventilation-perfusion
be elevated generally in patients with cancer (Moore scan along with cardiac echography is appropriate.
201842).
• Systemic thrombolysis is indicated for massive PE with hemo-
dynamic compromise except in patients with a high risk of
bleeding for whom catheter-assisted thrombectomy is indicated
(Kearon 201843).
• Factor Xa inhibitors have been shown to be noninferior to low-
molecular-weight heparin with apixaban demonstrating fewer
major bleeding events (Agnelli 202044).
• Patients without risk of bleeding can be immediately started on
long-acting agents; those at increased risk are first given a trial
of IV heparin.
• Patients with small, incidental PEs and no functional or vital
sign compromise are eligible to initiate anticoagulation in the
ED then be safely discharged home with close follow-up.
• Resumption of anticoagulation is recommended for recurrent VTE.
• The benefit of thromboprophylaxis has not been demonstrated
(Khorana 201945).
Superior vena cava syndrome • Facial edema and subcutaneous vein engorgement in • Elevate the head to minimize venous congestion.
the head, neck, and chest regions.
• Complete obstructions additionally present with • Diuretic use should be minimized (Sonavane 201547).
plethora, dyspnea, orthopnea, cough, hoarseness,
cyanosis, headache, seizures, and coma (Thomas &
Edmondson 199146).
• Mediastinal widening (66%) or pleural effusions • IV corticosteroids decrease extrinsic pressure on the vena cava.
(25%) on chest x-ray.
• CT with contrast venography is the gold standard for • Urgent thrombolysis, thrombectomy, or placement of a venous
measuring vena cava patency. stent may alleviate stridor, altered mental status, and hemody-
namic compromise although vascular intervention risks luminal
perforation (Friedman 201748).
• Fibrinolytic therapy can reduce the risk of thromboembolism
(Kee 199849).
• Medical and radiation oncology consultation should be expe-
dited to initiate systemic therapy because reducing tumor bulk
is definitive.
Gastrointestinal bleeding • Frank hematemesis or hematochezia. • Emergent gastroenterology consultation.
• Melena or coffee-ground emesis. • Volume repletion using crystalloid and blood products, as
determined by hemodynamics and hemoglobin levels.
• Reversal of anticoagulation where appropriate.
• Endoscopic administration of hemostatic powders provides the
lowest rebleeding rates (Tjwa 199850).
Neurologic complications
Malignant spinal cord • A gradual onset may only be demonstrated by back • Comprehensive neurologic examination followed by total spine
compression pain and weakness. MRI is the gold standard.
• Acute sensory loss, urinary retention, constipation, • For patients unable to tolerate MRI, a CT scan with and without
perineal numbness, or sudden inability to walk may IV contrast can be attempted, but the diagnostic yield because
suggest irreversible vascular injury and spinal cord of inferior imaging resolution is limited.
infarction.
(Continued)
6 CA: A Cancer Journal for Clinicians
CA CANCER J CLIN 2022;0:1–24
TABLE 3. (Continued)
SYNDROME PRESENTATION MANAGEMENT
Malignant spinal cord • Opiate pain control and dexamethasone 10 mg IV loading dose
compression (Continued) followed by 4 mg every 6 h are initiated along with urgent
neurosurgical and radiation oncology consultation (Barzilai
201851).
• If surgery is not indicated, palliative stereotactic body radio-
therapy of 16-24 Gy in 1 fraction or 24-30 Gy in 3 fractions is
administered (Eckstein 202152).
Increased intracranial pressure • Intractable headaches or nausea and vomiting are • An expedited noncontrast CT scan to evaluate for midline shift
most common; vomiting is significantly correlated is then followed by a nonurgent brain MRI with and without
with infratentorial lesions that risk brainstem contrast to further characterize the posterior fossa and deline-
impingement. ate smaller lesions (Schellinger 199953).
• Altered mental status, focal neurologic deficits, • Dexamethasone dosing as above is recommended except
vision changes or seizures are less frequent but more when lymphoma is suspected because this can compromise the
concerning (Esquenazi 201754). diagnostic biopsy by shrinking the mass (Ryken 201055).
• Hemorrhagic metastases are most likely to cause • Nonenzyme-inducing anticonvulsants (eg, levetiracetam) are
stroke-like focal deficits (Achrol 201956). typically administered in oncology patients because the risk of
drug-drug interactions is minimized, although there are mixed
data supporting their use (Kong 201557).
• Although hypertonic (3%) saline or mannitol can be
used emergently to create an osmotic gradient across the
blood-brain barrier, the priority is alleviating the mass effect
(Prabhakar 201458).
• Gamma Knife stereotactic radiosurgery has emerged as the pre-
ferred modality for managing solid intracranial masses because
of its favorable risk/benefit ratio; surgical approaches may be
necessary for addressing radiation necrosis (Brown 201659).
• Lumbar puncture increases the risk for herniation and is
contraindicated.
Thoracoabdominopelvic viscus
obstructions
Airway obstruction • Symptoms range from mild, subjective shortness of • Tracheal or bronchial stenting is the least invasive and pre-
breath to stridor and severe respiratory compromise. ferred intervention; laser therapy, balloon bronchoplasty, and
mechanical debulking are alternatives (Varadharajan 201660).
• Intubation, cricothyroidotomy, or tracheotomy may be required
to establish an emergency airway.
• The anatomical distortion in patients with previously resected
head and neck cancers may require otolaryngology consulta-
tion if airway management is needed.
• Postobstructive pneumonia requires broad-spectrum antibiotics
that cover both Pseudomonas spp. and methicillin-resistant
Staphylococcus aureus (Rolston & Nesher 201861).
• Interventional management of multiple small-airway obstruc-
tions from excessive tumor burden is not recommended.
Bowel obstruction • Vomiting, occasionally in the absence of nausea, is • Intractable vomiting is relieved by gastric decompression in
ubiquitous. combination with anticholinergics and octreotide to reduce
secretions (Franke 201762).
• Vomitus with upper tract obstructions often includes • Following decompression, complete bowel rest should be initi-
undigested food and liquids and occurs a short time ated with diet advancement, as tolerated.
after eating; lower tract obstructions are associated
with bilious or feculent vomiting (Alese 201563).
• Unrelenting abdominal pain. • Adynamic ileus additionally requires motility agents.
• Dilated loops of bowel on plain and cross-sectional • For esophageal, gastric outlet and rectosigmoid obstructions,
radiography. Mechanical obstruction has a transition consultation with interventional gastroenterology can deter-
point whereas, in functional obstructions, the bowel mine whether stenting is feasible.
is dilated throughout (Vilz 201764).
(Continued)
VOLUME 0 | NUMBER 0 | MONTH 2022 7
Oncologic emergencies and urgencies
TABLE 3. (Continued)
SYNDROME PRESENTATION MANAGEMENT
Bowel obstruction (Continued) • Persistent obstructions may require venting gastrostomy
tubes for permanent decompression of gastrointestinal
secretions.
• Although parenteral nutrition can be considered for highly
functioning patients with persistent obstructions, the evidence
for improved quality of life or survival is equivocal (Sowerbutts
201865).
Biliary tract obstruction • Painless jaundice or cholangitis-related febrile sepsis. • Hemodynamic stabilization followed by broad spectrum
antibiotics to cover enteral Enterobacteriaceae species and
anaerobes (Gomi 201866).
• Evaluation by endoscopic retrograde cholangiopancreatogram
to reestablish bile duct patency through stenting (Perone
201667).
• If the obstruction cannot be stented, transhepatic biliary drain-
age should be performed (Duan 201768).
Obstructive uropathy • Flank pain, oliguria, or an asymptomatic elevation of • Ultrasonography can identify hydronephrosis with a subsequent
serum creatinine on routine examination. CT scan to identify the location of the obstruction.
• Prolonged obstruction can precipitate permanent • Ureteral stents or percutaneous nephrostomy tubes can be
kidney injury. placed to decompress the obstruction (Tan 201969).
Abbreviations: ED, emergency department; Gy, grays; IV, intravenous; MRI, magnetic resonance imaging; PE, pulmonary embolism; VTE, venous
thromboembolism.
involves minimally invasive attempts at stenting the ob- represents 25% of malignant ascites cases.84 Pleural effusions
structed viscus and, if that is impossible, placing an exter- can also occur after poor cardiopulmonary circulation from
nal vent or drain to decompress the blockage. Patients with pulmonary emboli or external vascular compression, whereas
anaplastic thyroid cancer as well as head and neck cancers, pericardial effusions are also adverse effects of cyclophos-
in particular laryngeal cancer, are at risk for tracheal ob- phamide, cytarabine, dasatinib, doxorubicin, and gemcit-
struction with impending airway collapse.80 Lower airway abine treatment.85 Malignant effusions typically accumulate
obstruction is defined as ≥50% luminal narrowing of the insidiously over weeks to months, with the most common
mainstem bronchi, bronchus intermedius, or lobar bronchi. symptoms being pain and shortness of breath or nausea and
Concurrent postobstructive pneumonia significantly in- vomiting due to compression of visceral organs. In patients
creases morbidity and mortality. Obstructions of the gastro- with pericardial effusion, the classically described syndrome
intestinal tract can manifest from the most proximal regions of Beck triad (hypotension, jugular venous distention, and
of the esophagus through to the rectum. Upper gastrointes- muffled heart sounds) is rarely seen.86 Overall management
tinal tract obstructions can be caused not only by intrinsic involves initially draining the effusion, with hemodynamic
esophageal and gastric malignancies but also by pancreatic stability dictating the timing, coadministration of volume
cancer and locoregional lymphomas.81 Primary gastrointes- expanders (eg, albumin) as necessary, evaluation for locu-
tinal, genitourinary, and gynecologic cancers, in addition to lation and infection, and monitoring for re-accumulation.
metastatic peritoneal carcinomatosis, can cause small bowel Recurrent effusions may require membrane decortication
and large bowel obstructions. Postsurgical adhesions also or placement of indwelling drainage catheters to eliminate
contribute. Biliary tract obstruction is often the presenting the need for frequent instrumentation. The median survival
symptom associated with pancreatic, periampullary, and ex- after positive cytology is <12 months.87
trahepatic cholangiocarcinomas and with hepatic metasta-
ses. Obstructive uropathy is most common with pelvic or Cytotoxic Chemotherapy and Radiotherapy
retroperitoneal malignancies. Complications
Malignant effusions can occupy the pleural, pericardial, Classical cytotoxic chemotherapeutics and radiotherapy
and intraabdominal spaces and are largely precipitated by largely mediate their antineoplastic effects through affect-
tumor implants to the cavity membranes. Greater than 90% ing DNA replication. Substantial numbers of recognized
of pleural effusions are unilateral, and 56% to 65% arise from side effects, including tumor lysis syndrome (TLS), febrile
either breast or lung cancers.82 Similarly, malignant pericar- neutropenia, severe anemia, oral mucositis and esophagi-
dial effusions are most prevalent in breast and lung cancers tis, and chemotherapy-induced diarrhea (CID), are direct
in addition to melanoma and lymphoma.83 Ovarian cancer consequences. TLS results when a large volume of cells
8 CA: A Cancer Journal for Clinicians
CA CANCER J CLIN 2022;0:1–24
simultaneously releases its contents into the blood stream distress that negatively affects performance status, and aggres-
faster than their corresponding renal excretion rates to yield sive prophylaxis with loperamide and diphenoxylate/atropine
hyperkalemia and, from metabolism of the excess nucleo- combinations is standard.99 Breakthrough CID is commonly
tides, hyperphosphatemia and hyperuricemia.88 Although observed among patients receiving fluoropyrimidines, irino-
TLS can occur spontaneously with any tumor type, it is tecan, and tyrosine kinase inhibitors and those who have
more likely with treatment for high-grade lymphomas, acute incomplete compliance with prophylactic antidiarrheals.100
leukemias, and other rapidly proliferating tumors, such as Additional diarrheal etiologies, including graft- versus-
host
germ cell tumors.89 Seven days immediately after therapy disease and Clostridioides difficile, must also be entertained in
initiation reflects the highest vulnerability.90 the appropriate host. C. difficile colonization in patients with
Febrile neutropenia (FN) is a potentially life-threatening cancer is common due to frequent clinical touchpoints and
condition and is defined as a single oral temperature mea- gut microbiome depletion with either antibiotic use or cyto-
surement of ≥38.3 °C (101 °F) or a temperature of ≥38.0 toxic chemotherapy treatment can activate dormant spores to
°C (100.4 °F) sustained over a 1-hour period, combined trigger infection.101 Gastrointestinal graft-versus-host disease,
with severe neutropenia, defined as an absolute neutrophil characterized by a profuse secretory watery diarrhea, can occur
count (ANC) <500 cells/mm3 or an ANC that is expected as either an acute or chronic complication of allogeneic HSCT
to decrease to <500 cells/mm3 during the next 48 hours.91 and is a significant adverse prognostic factor.102
FN is a complication in up to 50% of patients with solid Radiotherapy and anthracyclines can cause late effects
tumors and in >80% of patients with hematologic malig- of tissue remodeling and subsequent fibrosis that can com-
nancies on active chemotherapy or after hematopoietic stem promise the cardiopulmonary system. Thoracic radiation
cell transplantation (HSCT) and most frequently occurs as a is a mainstay for locoregional lung cancer management. It
consequence of gut bacterial translocation in the absence of
is also common in patients being treated for breast, thy-
neutrophil-precipitated direct antimicrobiosis and immune-
mic, esophageal, and hematologic malignancies. Radiation
effector responses.92 Risk factors for FN include an ANC
pneumonitis, which is observed in up to 60% of patients
<100 cells/mm3 for >7 days, older age, poor performance
receiving intensity- modulated radiation therapy, can be
status, the presence of comorbid conditions, and advanced-
the dose- limiting toxicity.103 Incidence is substantially
stage disease.93 FN is considered a medical emergency, with
lower in patients receiving stereotactic beam radiotherapy.
an overall mortality of 5% to 20%, which can rise to 50%
Cardiomyopathy as a consequence of cardiac myofibril drop-
among patients with shock.94
out with subsequent necrosis and ensuing fibrosis can result
Although mild anemia (serum hemoglobin < 11.0 g/dL)
from a broad range of cytotoxic chemotherapies (primarily
is present in the majority of patients with cancer, severe ane-
anthracyclines), newer targeted therapies, and external-beam
mia (serum hemoglobin < 7.0 g/dL) occurs in 1 % to 7% of
radiotherapy to the chest, each in a dose-dependent fash-
patients and is associated with poor outcomes and decreased
quality of life.95 Severe anemia is usually a complication of ion usually after a latency period of ≥1 year after therapy.104
systemic therapy but can also occur from bone marrow in- Because early detection of presymptomatic heart failure can
filtration, gastrointestinal or genitourinary bleeding, poor improve outcomes,105 echocardiographic surveillance is rec-
overall nutrition or specific vitamin/mineral deficiency, as ommended in patients who receive high-dose anthracycline,
well as chronic infection. Tumor-provoked or treatment- ≥30 Gy of mediastinal radiation, the combination of a low-
provoked inflammatory cytokines may additionally precip- dose anthracycline and low-dose radiation, or a low-dose
itate chronic kidney disease and subsequent erythropoietin anthracycline and 2 cardiovascular risk factors within 6 to
deficiency. Profound anemia can delay chemotherapy cycles 12 months of completing therapy.106 The role of advanced
to further negatively affect prognosis.96 cardiac imaging for surveillance and early detection is being
Gastrointestinal distress is ubiquitous with standard che- explored.
motherapy and radiotherapy. Whereas chemotherapy can affect Reactive oxygen species are the acute irritants that un-
the entire gastrointestinal tract, radiotherapy selectively affects derlie hemorrhagic cystitis. Radiotherapy and chemotherapy
those regions within the field of radiation. Oropharyngeal and with select agents, including cyclophosphamide, ifosfamide,
esophageal mucositis can result not only from direct radia- busulfan, idarubicin and carboplatin, as well as intravesicular
tion damage to or high-dose chemotherapy effects on basal treatment with a broader range of chemotherapeutics and
epithelial cells but also from the release of reactive oxygen HSCT conditioning regimens are causative.107 Cessation of
species that triggers a proinflammatory cascade.97 Treatment chemotherapeutic therapy usually resolves the bleeding in a
with the mammalian target of rapamycin inhibitor everolimus few weeks once the bladder epithelium is restored. However,
also yields oral mucositis, with approximately 50% of patients radiotherapy-induced hemorrhagic cystitis can persist for
affected.98 CID contributes to physical and psychological years due to scarring and fibrosis of the bladder lining.108
VOLUME 0 | NUMBER 0 | MONTH 2022 9
Oncologic emergencies and urgencies
Chemotherapy-induced nausea and vomiting (CINV) inhibitor-induced dermatologic adverse events, and hand-
and peripheral neuropathy are mediated through diverse foot skin reaction (HFSR).
neurologic mechanisms, which include cell death and disrup- QTc prolongation with subsequent risk for ventricular
tion of synaptic vesicle transport with subsequent discharge. arrythmias has been observed among each of the subclasses
CINV results from discharge of gut enterochromaffin cell of small-molecule agents. Both tyrosine kinase inhibitors
serotonin.109 Depending on the emetogenic potential of and HDAC inhibitors can prolong QTc, with a mean in-
the chemotherapeutic or radiation regimen, prevention of crease of 15 msec and the largest effects observed from van-
CINV can include up to a 4-drug combination, compris- detanib, ibrutinib, and ribociclib.104 EGFR inhibitors induce
ing a 5-HT3 receptor antagonist, a neurokinin-1 antagonist, a spectrum of dermatologic complications, including pap-
dexamethasone, and, olanzapine.110 Topics regarding the ulopustular acneiform rash, dry skin, itching, and hair and
development, diagnosis, and management of peripheral neu- periungual alterations.137 Although these are rarely severe,
ropathy are discussed elsewhere in this review. they cause significant psychological distress, with the rash
Finally, infusion reactions to both classical chemothera- having the greatest negative impact on quality of life.138
pies and biologic therapies are common. Although they are HFSR is a dermatologic complication of the multityrosine
most frequently observed with platinum-based compounds kinase inhibitors sorafenib and regorafenib (60%) and the
(12%-24%),111 taxanes (30%),111 ofatumumab (60%),112 vascular edothelial growth factor (VEGF) inhibitors suni-
obinutuzumab (60%),113 and rituximab (70%-80%),114 they tinib and axitinib (30%), resulting from the simultaneous
can occur after any systemic therapy. Both IgE-mediated disruption of epithelial and vascular remodeling necessary
allergic and anaphylactoid mechanisms are noted. Table 4 after routine touch-induced microtrauma. Although mecha-
summarizes the most common complications observed with nistically different, HFSR is similar to hand-foot syndrome
these therapeutic modalities and the current standards for or palmar-plantar erythrodysesthesia, an epidermal irritation
their management.90,91,110,115-132 seen with certain cytotoxic chemotherapies (eg, capecitabine,
liposomal doxorubicin, docetaxel, and continuously infused
Targeted Therapeutic-Related Complications 5-fluorouracil).139 The significant pain associated with rou-
Targeted therapies represent the subclass of antineoplastic tinely applied pressure to eroded surfaces adversely affects
140
agents deliberately engineered to interfere with oncogenic quality of life and is often a dose-limiting toxicity.
signal transduction pathways and are divided into small- Monoclonal antibodies are subdivided into naked
molecule inhibitors, monoclonal antibody-based pharma- monoclonal antibodies, which halt signal transduction by
ceuticals, and cell-based agents. In general, targeted agents inhibiting ligand- receptor interactions (eg, trastuzumab,
are less toxic than nonspecific cytotoxic chemotherapeutics; bevacizumab, and pembrolizumab); antibody-drug/radiola-
however, because many agents require long-term use, both bel conjugates, which deliver cytotoxic agents specifically to
acute and chronic treatment- related toxicities should be malignant cells (eg, gemtuzumab ozogamicin, brentuximab
133
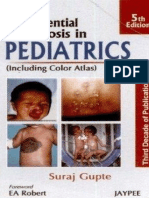
considered (Fig. 2). Finally, certain adverse events reflect vedotin, and sacituzumab govitecan); and bispecific anti-
an on-target effect to nonneoplastic tissues.134 bodies, which recruit immune cells to the immediate can-
Small- molecule compounds represent an increasingly cer microenvironment (eg, blinatumomab). Antiangiogenic
prevalent class of antineoplastic agents, with a total of 89 therapy is a frequently used modality that includes mono-
novel antineoplastic small molecules having been approved clonal antibodies that bind circulating VEGF-A (beva-
through 2020.135 The largest group of small-molecule anti- cizumab) or the VEGF receptor-2 extracellular domain
neoplastics are kinase inhibitors, but additional targets in- (ramucirumab and alacizumab pegol) in addition to small
clude epigenetic regulatory proteins (eg, histone deacylase molecules that bind the VEGF receptor intracellular tyro-
(HDAC) inhibitors), DNA damage- repair enzymes (eg, sine kinase domain (eg, axitinib, sunitinib). Because VEGF
poly- [ADP- ribose] polymerase inhibitors), and protea- signaling plays an important role in vascular homeostasis,
somes. These agents can also cause cytopenias (eg, olaparib, patients receiving antiangiogenic therapy may develop hy-
niraparib, and, entrectinib), nausea, vomiting and diarrhea pertensive urgency or emergency, hemorrhagic stroke, un-
(eg, ribociclib, palbociclib, vemurafenib, and dabrafenib), and stable angina, or myocardial infarction as well as venous
cardiomyopathy (eg, cobimetinib, trametinib, sunitinib, and thromboembolism, atherosclerosis, and platelet activa-
pazopanib).104,136 Management of these complications par- tion.141 Antiangiogenic drugs can also trigger posterior re-
allels previously described algorithms. Cataloguing the spe- versible encephalopathy syndrome (PRES) which involves
cific toxicities associated with each approved small-molecule direct injury to the cerebrovascular endothelium with an
agent can be accessed in the reviews cited above. Three ensuing inflammatory response and cytokine release that
toxicities unique to these small-molecule agents are QTc triggers vasogenic edema. This is mediated through break-
prolongation, epidermal growth factor receptor (EGFR) down of the blood- brain barrier, which preferentially
10 CA: A Cancer Journal for Clinicians
CA CANCER J CLIN 2022;0:1–24
TABLE 4. Cytotoxic Chemotherapy and Radiotherapy Complications: Common Presentations and Management Strategies
SYNDROME PRESENTATION MANAGEMENT
Tumor lysis syndrome • Laboratory tumor lysis syndrome is defined according to serum • Aggressive hydration with crystalloid improves renal perfusion
levels of uric acid, potassium, phosphorus, and calcium and and glomerular filtration as well as reduces uric acid or calcium
requires either a 25% change in value or ≥2 abnormal values phosphate crystallization and tubular deposition.
among these (Cairo & Bishop 2004115).
• Hyperkalemia destabilizes myocardial and other muscular con- • Continuous cardiac monitoring and re-evaluation of serum
ductivity and can trigger nausea, numbness, heart palpitations, electrolytes, creatinine, and uric acid every 4-6 h track the clini-
arrythmias, seizures, and possible sudden death. cal course.
• Both uric acid and calcium phosphate can precipitate in the • In patients with urine output <2 mL/kg per h, a loop diuretic
renal tubules to trigger an intrarenal acute kidney injury. may be considered.
• Flank pain raises concern for ureteral stones. • Allopurinol reduces the formation of uric acid and is prophylac-
tically administered to at-risk patients.
• Rasburicase metabolizes uric acid and is the preferred
medication for extreme hyperuricemia; 0.2 mg/kg is initially
administered with repeated dosing as necessary but should be
avoided in patients with G6PD deficiency because it can lead
to methemoglobinemia and hemolysis (Bosly 2003116).
• Renal replacement therapy may be required for severe kidney
injury or persistent electrolyte abnormalities (Jones 201590).
Febrile neutropenia • A single oral temperature measured at ≥38.3 °C (101 °F) or • The current door-to-antibiotics guideline is <1 h after ED pres-
a temperature of ≥38.0 °C (100.4 °F) sustained over a 1-h entation, although recent research has shown that delays up to
period combined with severe neutropenia, defined as an abso- 3 h do not substantially affect outcomes (Daniel 2019117).
lute neutrophil count (ANC) <500 cells/mm3 or an ANC that is
expected to decrease to <500 cells/mm3 during the next 48 h
(Zimmer & Freifeld 201991).
• Presentation can bridge the spectrum from otherwise asympto- • Blood cultures, both peripheral and from in-dwelling lines,
matic to moribund with florid hemodynamic collapse. should be universally collected because the established rate of
bacteremia is 10%-25%.
• Empiric monotherapy with an antipseudomonal β-lactam is
recommended with the following exceptions:
◦ Carbapenems for patients with a high risk of infection by an
extended-spectrum β-lactamase-expressing organism
◦ Polymyxin-colistin in patients at high risk for a
carbapenemase-producing Klebsiella
◦ Aztreonam, fluoroquinolones, or aminoglycosides for
patients with an anaphylactic β-lactam allergy (Zimmer &
Freifeld 201991).
• Vancomycin, linezolid, or daptomycin should be given only
when either methicillin-resistant Staphylococcus aureus or
indwelling catheter infections are likely and should be discon-
tinued once these are ruled out (Niessen 2020118).
• Empiric antifungal coverage is not recommended at the time
of presentation; however, in patients with prolonged, profound
neutropenia, invasive fungal disease markers should be assayed
and empiric therapy begun after 4-7 d of persistent fevers and
no apparent bacterial source with echinocandins being the
preferred choice (Chen 2017119).
• The MASCC criteria defines patients with scores ≥21 as low-
risk patients safe for ED discharge and outpatient management
(Klastersky & Paesmans 2013120) with appropriate regimens
comprised of broad-spectrum β-lactams combined with a
fluoroquinolone (Klastersky 2006121).
Severe anemia • Because of decreased oxygen-carrying capacity, debilitating • Reticulocyte count and haptoglobin, iron studies, serum vitamin
fatigue and dyspnea, initially with exertion then at rest, are the B12 and folate levels, liver function tests (including albumin,
predominant presenting symptoms. prealbumin, total and direct bilirubin), and lactate dehydroge-
nase concentrations as well as a peripheral blood smear should
be obtained in addition to the complete blood count.
(Continued)
VOLUME 0 | NUMBER 0 | MONTH 2022 11
Oncologic emergencies and urgencies
TABLE 4. (Continued)
SYNDROME PRESENTATION MANAGEMENT
Severe anemia • In the appropriate situations, hemagglutinins can be assessed
(Continued) to rule out hemolysis.
• Ensuring adequate nutrition can partially remediate chronic
causes.
• Transfusion should be used as sparingly as possible and should
target a hemoglobin level of 7.0 mg/dL unless the patient has
established cardiac disease or continues to be overtly sympto-
matic where 8.0 mg/dL is appropriate (Watkins 2015122).
• Completing transfusions in the ED can offset the additional
financial toxicity of an inpatient admission.
• Erythropoiesis-stimulating agents are no longer indicated for
cancer-related anemia (Schoen 2020123).
Oral mucositis and • Intractable breakthrough pain with multiple open mouth sores. • Pain control often requires opiate analgesia in addition to topi-
esophagitis cal anti-inflammatory, lidocaine-containing mouthwashes.
• Severe dehydration and failure to thrive because of inadequate • Nystatin is indicated for thrush.
oral intake.
• When mucositis is expected to persist for several wks (eg,
in patients with head and neck cancers requiring extended
courses of radiotherapy), placement of a percutaneous feeding
tube may be required.
Chemotherapy-induced • Multiple, frequent, liquid bowel movements per d, typically as- • Intravenous hydration with deliberate potassium and magne-
diarrhea sociated with urgency, which can be provoked by or independ- sium supplementation to offset gastrointestinal losses.
ent of meals or with nocturnal arousal.
• Superinfections with Escherichia coli or Salmonella species
whose virulence is accentuated in patients with cancer must
also be considered (Chao 2017,124 Ku 2012125).
• Clostridioides difficile is ruled out through toxin enzyme
immunoassays combined with nucleic acid amplification tests.
• Oral vancomycin or fidaxomicin for 10 d is the first-line therapy
for mild-to-moderate C. difficile infections; intravenous met-
ronidazole is added in more severe cases characterized by signs
of peritonitis, leukemoid reaction, toxic megacolon, or severe
sepsis (Guh & Kutty 2018126).
• Graft-versus-host disease is treated with aggressive hydration
and electrolyte repletion along with systemic steroids dosed at
2 mg/kg with supplemental oral budesonide; ibrutinib, ruxoli-
tinib, belumosidil, and basiliximab are useful secondary agents
in refractory cases (Ruutu 2014,127 Waller 2019,128 Zeiser
2021,129 Jagasia 2021,130 Liu 2020131).
Radiation pneumonitis • Radiation pneumonitis is a diagnosis of exclusion that typically • Initiation of a slow steroid taper and optimization of
presents 3-12 wks after completion of radiotherapy. oxygenation.
• Characterized by a low-grade fever, shortness of breath, • Patients with a new oxygen requirement may benefit from brief
nonproductive cough, crackles on physical examination. inpatient observation.
• Cross-sectional imaging is notable for fibrosis in the field of
radiation.
Cardiomyopathy • Patients present with asymptomatic or symptomatic left • Management is consistent with standard heart failure protocols
ventricular dysfunction. that include admission to telemetry and escalation to intensive
care, as appropriate.
• Increased susceptibility in patients with prior history of heart
failure.
• Patients with cancer and survivors must be surveyed for prior
anthracycline or radiation exposure.
Hemorrhagic cystitis • Bleeding is primarily microscopic, but persistent bleeding can • Blood transfusion to correct ensuing anemia.
precipitate intravesicular blood clot formation with subsequent
urinary tract obstruction (Manikandan 2010132).
(Continued)
12 CA: A Cancer Journal for Clinicians
CA CANCER J CLIN 2022;0:1–24
TABLE 4. (Continued)
SYNDROME PRESENTATION MANAGEMENT
Hemorrhagic cystitis • Continuous bladder irrigation using a large-bore, 3-way
(Continued) catheter with saline infusion may be necessary to evacuate a
substantial clot burden.
Chemotherapy-induced • Weakness and dehydration from decreased oral intake because • Intravenous hydration corrects volume deficits.
nausea and vomiting of ongoing symptoms.
• Breakthrough episodes are treated with short-acting antiemet-
ics (eg, ondansetron, lorazepam, prochlorperazine, or olanzap-
ine) prioritized to complement the patient’s existing outpatient
regimen (Hesketh 2017110).
• Inpatient admission is required for patients unable to tolerate
enteral nutrition.
Hypersensitivity • Common clinical manifestations include: • The infusion should be terminated immediately if not already
reactions ◦ Fatigue, myalgia, fever, headache finished.
◦ Rash, urticaria, pruritus, flushing • Respiration and hemodynamics must first be stabilized.
◦ Nausea, vomiting, abdominal pain
◦ Dyspnea, throat irritation, pharyngeal or laryngeal edema, • If severe anaphylaxis or angioedema is suspected, intramuscular
bronchospasm epinephrine should be administered immediately.
◦ Dizziness, hypotension, tachycardia. • For milder reactions, use of H1 and H2 receptor antagonists and
glucocorticoids may be sufficient.
• Symptomatic wheezing additionally requires nebulized β-
agonist bronchodilators.
Abbreviations: C. difficile, Clostridioides difficile; ED, emergency department; MASCC, Multinational Association for Supportive Care in Cancer.
affects the bilateral parieto-occipital region because of the HER2-targeting agents (pertuzumab, neratinib, and lapa-
paucity of sympathetic innervation of the posterior fossa.142 tinib) are substantially less cardiotoxic.146
Nearly one-half of patients with PRES have autoimmune Administration of ozogamicin-conjugated gemtuzumab
disorders; patients who have cancer with these comor- or inotuzumab monoclonal antibodies can lead to hepatic
bidities are at increased risk.143 Trastuzumab-associated sinusoid occlusion syndrome/venous occlusive disease, an
cardiomyopathy arises from and occurs concurrently with obliterative terminal hepatic venulitis caused by a prothrom-
ongoing therapy.144 Because it is mediated through HER2 botic, hypofibrinolytic state which can also be observed in
signal-transduction pathways within endocardial cells, left the first 60 days after allogeneic HSCT.147 In the presence
ventricular function improves when therapy is withdrawn of multiorgan failure, the mortality rate of sinusoid occlusion
although 25% of patients never fully recover.145 Other syndrome may reach 80%.
FIGURE 2. Mechanisms of Targeted Therapeutics Toxicities. Targeted therapies can be subdivided into small molecules, cell-based therapies (eg, chimeric
antigen receptor [CAR] T-cells), and antibody-based therapies, with the latter including the specific subclasses of antibody-drug conjugates and immune
checkpoint inhibitors. Although some toxicities, such as immune-related adverse events, QTc prolongation, and sinusoidal occlusion syndrome, are class-
specific, angiogenesis-related toxicities and cytokine release syndrome are demonstrated with multiple classes.
VOLUME 0 | NUMBER 0 | MONTH 2022 13
Oncologic emergencies and urgencies
Immune checkpoint inhibitors (ICIs) represent a sub- workup occurring in the ED.163 The spectrum of targeted
class of naked monoclonal antibodies that undermine a therapeutic toxicities is presented in Table 5.137,142,152,163-185
tumor cell’s ability to evade detection by the patient’s im-
mune system by abrogating the patient’s natural antitumor Cancer Pain Management
T-cell response.148 To date, 3 immune checkpoint targets Cancer-related pain results from either the malignancy itself
(cytotoxic T-lymphocyte–associated protein 4 (CTLA-4), or its treatment and it affects both patients on active treat-
programmed cell death 1 (PD-1), and programmed cell ment and long-term cancer survivors alike. Pain is the most
death ligand 1 (PD-L1)) have agents approved as first- common chief complaint upon ED presentation for patients
line, standard-of-care treatment for a broad spectrum of with end-stage disease. Severe pain correlates with increased
solid and liquid tumors.149,150 Relatlimab, an anti-L AG3 hospital readmissions, morbidity, and mortality.186 Among
monoclonal antibody, is in late-stage clinical trials.151 By survivors, approximately 40% will experience chronic pain
interfering with this immunologic balance of self-tolerance, posttreatment, and 5% to 10% will have pain that interferes
the primary adverse events associated with ICIs mimic au- with daily living.187 Acute pain crises can be triggered by
toimmune disorders.152 Altogether, the incidence rate of disease progression, tolerance to prescribed therapy, and sub-
immune- related adverse events (irAEs) of any intensity optimal use of a prescribed regimen or can be provoked by
exceeds 80%, and that for severe toxicities leading to hospi- ongoing systemic chemotherapy/radiotherapy. Nociceptive
talization or death approaches 30% across all classes of med- (visceral or somatic) and neuropathic pain mechanisms can
ications.153 Toxicities peak at 12 to 16 weeks after initiation present either independently or in combination.
(around the fourth dose) but have been reported to occur Algorithms for evaluating cancer- related pain are de-
even after the first dose, after many months of treatment, termined by the patient’s primary cancer, prior and ongoing
or even after stopping treatment.154 Combination therapy treatments, as well as established locations for known disease.
with 2 ICIs precipitates irAEs earlier than monotherapy.155 Skeletal surveys should be considered for patients in whom
The presence of irAEs correlates with overall response, lytic or sclerotic bony lesions are suspected. In patients at risk
and improved survival has been observed among patients for peritoneal carcinomatosis, a computed tomographic scan of
with multisystem, mild-to-moderate irAEs after adjusting the abdomen and pelvis should be obtained. Comparison with
for treatment duration. Most irAEs respond to high-dose prior imaging can corroborate progression of disease as the
glucocorticoids (1-2 mg/kg daily), and acute management etiology of observed breakthrough pain. The physical relation-
involves urgently starting therapy in consultation with the ship between a tumor and proximate nerve trunks and plexuses
primary oncologist.156 should be considered because this may suggest the likelihood
Chimeric antigen receptor (CAR) T- cells are a cell- of mixed pain syndromes and the possible need for advanced,
based therapy in which the patient’s T-cells are extracted multimodal interventions that combine both pharmacologic
using leukapheresis and then are genetically modified in and nonpharmacologic strategies. Cancer-related pain must
the laboratory through the insertion of DNA encoding a also be discriminated from both chronic pain that predated the
recombinant CAR whose extracellular domain recognizes malignancy and acute pain episodes from comorbid pathol-
a cancer-specific antigen, whereas the intracellular domain ogies, such as gallstones, renal stones, and headaches, each of
contains signaling components to activate the T-cell im- which requires management according to standard practices.
munogenic, antineoplastic response.157,158 The cells are Opioids are the first-line treatment for cancer-related
subsequently reinfused into the patient and can persist for nociceptive pain. Standard outpatient regimens include
>2 years.159 There are currently 2 approved CD19-specific scheduled short-acting and extended-release oral formula-
CAR T-cells treatments: tisagenlecleucel for patients with tions, breakthrough as-needed oral agents, and transdermal
relapsed or refractory B-cell acute lymphoblastic leukemia160 fentanyl. Tolerance (ie, muted therapeutic response) to a
and axicabtagene ciloleucel for patients with relapsed or re- previously effective dose frequently develops, such that dose
fractory diffuse large B-cell lymphoma.161 Antigens useful escalation is necessary to maintain adequate pain control.
for multiple myeloma, chronic lymphocytic leukemia, me- Patients who are receiving a daily oral morphine equiva-
sothelioma, ovarian cancer, pancreatic cancer, and prostate lency >200 mg per day may be at higher risk for under-
cancer are currently under investigation.162 Severe adverse treatment of their cancer pain.188 Because it is common for
reactions are seen in up to 88% of treated patients. Although patients to either underuse an as-needed prescription or to
myelosuppression after conditioning regimens and cytokine develop confusion regarding their correct schedule, confirm-
release syndrome is typically observed in the inpatient set- ing compliance with the prescribed regimen coupled with
ting 24 to 72 hours immediately after CAR T-cells infusion, ED-facilitated re-education and supervised administration
immune cell-associated neurologic syndrome (ICANS) can of scheduled oral pain medications can promote a straight-
first manifest up to 12 weeks after infusion, with the initial forward, same-day safe discharge to home.
14 CA: A Cancer Journal for Clinicians
CA CANCER J CLIN 2022;0:1–24
TABLE 5. Targeted Therapy Complications: Common Presentations and Management Strategies
SYNDROME PRESENTATION MANAGEMENT
Small-molecule
therapeutic-related
toxicities
QTc prolongation • QTc >450 msec in males or >470 msec in females. • Routine electrolyte assessment to ensure serum K+ >4.0 and Mg2+
• Tyrosine kinase inhibitors display a mean increase of 15 msec; >2.0.
the largest QTc prolongation occurs with vandetanib, ibrutinib, • Routine serial EKG monitoring.
and ribociclib. • Ventricular arrythmias are managed according to advanced cardiac
• Crizotinib, dasatinib, lapatinib, nilotinib, pazopanib, sunitinib, life support algorithms.
sorafenib and vemurafenib, as well as romedepsin should
be administered cautiously in patients with preexisting QTc
prolongation.
EGFR inhibitor skin • Rash typically presents within 2 wks after initiating treatment • Topical calcineurin inhibitors which should be prescribed with
toxicities and forms around hair follicles, therefore is densest on the dermatologic consultation (Lacouture 2006137).
scalp, face, and upper torso which correlates with hair follicle
density (Tsimboukis 2009164).
• Most frequent with erlotinib, afatinib, cetuximab, and
panitumumab; among these, presence of the rash positively
correlates with survival (Chu 2018,165 Petrelli 2013166).
Hand-foot skin • Most commonly observed with regorafenib, sorafenib, axitinib, • A cocktail of topical high-dose steroids, a nonsteroidal anti-
reaction and sunitinib. inflammatory, and an emollient is effective.
• Characterized by palmar-plantar numbness, tingling or burning • Ultimately, dose reduction or switching to an alternate regimen is
pain alongside yellowish, hyperkeratotic plaques in high- required.
pressure areas of the hands and feet (Nikolaou 2016167).
Monoclonal antibody-
related toxicities
Sinusoid occlusion • Elevated liver function tests, and hyperbilirubinemia in a • High-dose glucocorticoids for moderate-to-severe disease (Al
syndrome patient treated with ozogamicin-conjugated monoclonal Beihany 2008168).
antibodies, or after allo-HSCT. • Defibrotide, an anti-inflammatory, antithrombotic, profibrinolytic
• Tender hepatomegaly and ascites. agent, can be administered in severe cases after normalization of
platelet count, fibrinogen, and prothrombin time with appropriate
blood products (Ho 2008169).
Angiogenesis-related • Hypertensive urgency or emergency. • Acute hemodynamic stabilization with advanced cardiac life support,
toxicities • Altered mental status. as indicated.
• Unstable angina or myocardial infarction from atherosclerosis • Noncontrast head CT to evaluate for hemorrhagic stroke in patients
and platelet activation. with altered mental status.
• PRES presents with nonspecific neurologic findings including • If posterior reversible encephalopathy syndrome (PRES) is suspected,
headache (50%), seizures (65%-70%), encephalopathy (up to an MRI should be obtained to evaluate for vasogenic edema in the
80%), visual disturbances (33%), and focal neurologic defects parieto-occipital region bilaterally on T2-weighted images, which is
(15%) (Fugate & Rabinstein 2015142). diagnostic.
• There is no specific treatment for PRES, and care is usually
supportive.
• Optimal preventive strategies for cardiac and cerebrovascular events
are still under investigation, but current standards include high-
dose statins, aspirin, and aggressive blood pressure control (Touyz
2018170).
(Continued)
VOLUME 0 | NUMBER 0 | MONTH 2022 15
Oncologic emergencies and urgencies
TABLE 5. (Continued)
SYNDROME PRESENTATION MANAGEMENT
Immune-related adverse General management across all irAEs:
events (irAEs)a
Dermatitis • Rash, pruritis, or bullous dermatitis occurs in 50% and typically • First-line therapy for all irAEs is high-dose glucocorticoids
appears in the first 2 cycles. (1-2 mg/kg), either oral or parenteral as clinically indicated.
• Niklosky sign, Stevens-Johnson syndrome, toxic epidermal • With mild reactions, trend abnormal laboratory values (eg, serum
necrolysis, and drug rash with eosinophilia and systemic lipase, liver function tests, troponin, or creatinine).
symptoms can occur (Belum 2016171).
• Severe reactions require hospitalization.
• After severe events, urgent subspecialty consultation may be
required.
• Second-line immunosuppressants for steroid-refractory patients
include:
◦ Infliximab (antitumor necrosis factor-α)
◦ Mycophenolate mofetil (nucleic acid depletion)
◦ Antithymocyte globulin (T-cell depletion)
◦ Tocilizumab (anti-interleukin-6)
Colitis • Colitis typically occurs within 5-8 wks of initiating therapy in ◦ Vedolizumab (anti-α4β7 integrin; regulates T-cell trafficking)
the absence of comorbid infections. ◦ Intravenous immunoglobulin (broad immunosuppression)
• It is a dose-limiting toxicity with severe disease present in 10% ◦ Rituximab (anti-CD20; B-cell depletion)
(Rajha 2020172). ◦ Tacrolimus (calcineurin inhibitor) (Sullivan & Weber 2021152).
Hepatitis and • Hepatitis occurs in about 5% of patients and is defined as
pancreatitis serum transaminase or serum bilirubin levels >1 times the
upper limit of normal (ULN); severe disease is noted at serum
transaminase levels >3 times or bilirubin >5 times the ULN.
• Exocrine pancreatitis, noted by isolated levels of serum lipase,
is rare.
• Most cases are asymptomatic, but severe cases may warrant Organ-specific considerations in irAEs:
discontinuation (Dougan 20211173).
Hypophysitis • Mild presentations include headache, fatigue, and general • High-grade pruritis requires supplemental gabapentin or pregabalin
weakness that can be misattributed to the malignancy itself (Wu & Lacouture 2018175).
(Faje 2016174). • Administer levothyroxine for patients who have hypophysitis and
• Central adrenal insufficiency represents a significant source of thyroiditis; mineralocorticoid is additionally required for hypophysitis.
morbidity and mortality. • Adrenal crisis-driven hypotension and hyponatremia require emer-
• Subtherapeutic TSH levels with concomitant low thyroid func- gent intervention.
tion tests in the absence of supplementation can corroborate • Severe thyrotoxicosis can be treated with methimazole or
the diagnosis. propylthiouracil.
• Patients with diabetes mellitus will require initiation of subcutane-
ous insulin following ketoacidosis resolution.
• MRI without contrast is the preferred imaging modality to evaluate for
encephalitis and can demonstrate T2 hyperintensities in 25% of cases.
• Supplemental oxygen may be required for pneumonitis; antibiotics
should be withheld unless infection is strongly suspected.
• Aggressive hydration and monitoring of renal function are necessary
with myositis-induced rhabdomyolysis.
• Mild ophthalmic involvement requires ophthalmologic consultation
for intraocular steroid administration.
Thyroiditis • Occurs in up to 20% of patients.
• Can initially present as thyrotoxicosis but ultimately manifests
as hypothyroidism.
• Myxedema with altered mental status, bradycardia, and hypo-
thermia can occur in severe cases (de Filette 2016176).
Islet cell-mediated • New-onset diabetes mellitus has been reported in 1% and
diabetes mellitus most frequently presents as acute-onset diabetic ketoacidosis
(Maamari 2019177).
Encephalitis • Mild and nonspecific neurologic findings (eg, headaches, dizzi-
ness, and sensory impairment) are reported in 6%-12%.
• Severe encephalitis, manifested by confusion, ataxia, abnormal
behavior, altered mental status, and seizures occurs in 0.1%.
(Continued)
16 CA: A Cancer Journal for Clinicians
CA CANCER J CLIN 2022;0:1–24
TABLE 5. (Continued)
SYNDROME PRESENTATION MANAGEMENT
Pneumonitis • Occurs in only 3%-5% of patients, but severe cases can be
fatal.
• Presents with new persistent cough or shortness of breath
along with new ground-glass opacities or interlobular septal
thickening on CT scan in the absence of infection or tumor
progression (Suresh 2018178).
Arthritis, parotitis, and • Rheumatologic irAEs occur in 5%-11%, with myositis being
myositis the most severe (Steven & Fisher 2019179).
• Myositis presents with myalgias and proximal muscle weak-
ness concurrent with elevations in serum muscle enzymes (cre-
atine phosphokinase, aldolase, and, occasionally, troponins).
Nephritis • Intrinsic nephrotoxicity occurs in 2%-5%; most commonly as
acute interstitial nephritis with or without tubular injury or
glomerular disease (Cortazar 2016180).
• Serum creatinine can peak as high as 3-4 g/dL and may not re-
turn to baseline after adequate therapy, even among patients
with no prior renal disease.
Uveitis • Occurs in 1%. Although most cases are mild nongranuloma-
tous anterior inflammation, panuveitis can lead to impaired
visual acuity (Cunningham 2020181).
Myocarditis • Occurs in <1% but can present with decompensated heart
failure or with highly morbid arrhythmias, including ventricular
tachycardia or complete atrioventricular block (Eschudier
2017182).
Hemophagocytic • Rare but potentially fatal.
lymphohistiocytosis
• Presents with fever, cytopenias, splenomegaly and elevated
serum triglycerides, fibrinogen, ferritin,
C-reactive protein, and soluble interleukin-2 (Sadaat & Jang
2018183).
CAR T-cell therapy
toxicities
Cytokine release • Clinical and pathologic variant of sepsis marked by fever and • Hemodynamic stabilization and respiratory support may require ag-
syndrome fatigue along with elevated levels of serum C-reactive protein, gressive IV fluid support, vasopressors, and mechanical ventilation.
ferritin, and interleukin-6 (Lee 2014184). • If supportive care measures are insufficient, patients first receive to-
• Hemodynamic collapse occurs in 27%-43%. cilizumab, then corticosteroids, concurrently or sequentially (Reigler
2019185).
• Up to 95% of cases will resolve with supportive measures, although
high-dose IV corticosteroids are given for severe ICANS.
• Tocilizumab is not effective in preventing or managing neurotoxicity.
Immune cell-associated • ICANS manifests as confusion, dysarthria, ataxia, tremors,
neurologic syndrome expressive aphasia, somnolence, memory problems, seizures, or
(ICANS) obtundation and occurs in 21%-38% of patients (Santomasso
2019163).
a
Abbreviations: allo-HSCT, allogenic hematopoietic stem cell transplantation; CAR T-cells, chimeric antigen receptor T cells; CT, computed tomography; EKG, elec-
trocardiogram; IV, intravenous; MRI, magnetic resonance imaging; TSH, thyroid-stimulating hormone.
When breakthrough therapy is necessary, intravenous opi- intravenous opioids; 2-6 hours for short-acting oral medica-
oids are indicated. Optimal initial breakthrough dosing for tions).190 In cases of moderate-to-severe hepatic capsulitis or
adults is 10% of the total daily opiate dose (5% in the elderly). bony pain, steroids or nonsteroidal anti-inflammatory agents
Converting between different opiates and intravenous and oral can be useful as adjunctive therapies.191 Patients in whom sus-
formulations of the same opiate is conducted using calibration tained analgesia is achieved using combinations of oral and
against morphine-equivalents (Table 6).189 Redosing should be transdermal formulations can discharge to home. Hospital ad-
conducted if the pain is still not adequately managed at the mission is required for those experiencing ongoing, intractable
expected peak pharmacokinetic concentration (15 minutes for pain despite repeated intravenous dosing.
VOLUME 0 | NUMBER 0 | MONTH 2022 17
Oncologic emergencies and urgencies
Patients who are tolerant to extremely high daily mor- TABLE 6. Equianalgesic Dosing Among Opiate Agonists
phine equivalents are at risk for acute neurotoxic effects EQUIANALGESIC DOSEa
such as confusion, hallucination, respiratory depression, and
PO (ONSET
constipation. Patients at highest risk include those who are MEDICATION IM/IV (ONSET 15-30 MIN) 30-60 MIN)
relatively opioid-naive, are elderly, have a comorbid mood
Morphine 10 mg 30 mg
disorder, or are concurrently requiring sedative-hypnotics.192
Oxycodone — 20 mg
Moreover, because opioids are metabolized by the liver and
cleared by the kidney, both chronic and breakthrough dosing Codeine 130 mg 200 mg
should be adjusted in patients with hepatic or renal dysfunc- Hydrocodone — 30 mg
tion.193,194 Morphine should be generally avoided in patients Hydromorphone 1.5 mg 7.5 mg
with an acute kidney injury. To guard against constipation, all Fentanyl 12.5 mcg/h patch = 30-59 mg oral morphine 24 h dose
patients should concurrently initiate a daily bowel regimen 25 mcg/h patch = 60-134 mg oral morphine 24 h dose
using guidelines that recommend a tiered approach with the 50 mcg/h patch = 135-224 mg oral morphine 24 h dose
initial introduction of stool softeners (eg, docusate) in com- 75 mcg/h patch = 225-314 mg oral morphine 24 h dose
bination with stimulant laxatives (eg, bisacodyl, senna) and 100 mcg/h patch = 315-404 mg oral morphine 24 h dose
the subsequent addition of osmotic agents (eg, polyethylene Abbreviations: IM, intramuscular; IV, intravenous; PO, per os (oral).
glycol, magnesium citrate, lactulose).195 Opioid-induced
a
Data are from Quill 2019.189
constipation that is refractory to ≥2 traditional laxatives is
eligible for peripherally acting μ-opioid receptor antagonists aggressive end-of-life care, oncologists’ hesitation to directly
(eg, nadelmidine, naloxegol).196 For respiratory depression in and clearly discuss transitions of care with patients also con-
which urgent reversal is required, 1 mL of low-dose nalox- tributes.205 Consequently, some patients are first confronted
one (0.4 mg naloxone in 10 mL normal saline) is admin- with end-of-life decision making when they present to the
istered every 5 minutes until a satisfactory respiratory rate ED for acute management of terminal cancer complications.
is restored. More aggressive treatment with naloxone may Moreover, when de-escalated goals of care are not previ-
cause a traumatic return of severe, uncontrollable pain.197 ously documented in the medical record, ED clinicians are
Neuropathic pain is most often characterized as numb- defaulted into initiating an aggressive treatment plan that
ness, either hot or cold prickling, or electric sensations, with may be contrary to the patient’s underlying preferences.206
or without muscle weakness. It can be tumor-related, such as To avoid this gap, the American College of Emergency
with invasion of the celiac plexus in pancreatic cancer,198 or, Physicians Choosing Wisely Campaign expressly states that,
more commonly, a consequence of certain chemotherapies, in the absence of advance directives, goals-of-care discussions
such as platinum-based compounds.199 Neuropathic pain should begin in the ED.207 These conversations should use
syndromes respond variably to opioids.200 Gabapentin, pre- strategies such as SPIKES208 or EMAP,209 which are rubrics
gabalin, duloxetine, and glucocorticoids are commonly used for breaking bad news, to align care escalation plans with
but typically require several weeks to attain maximal ther- near-term prognosis while accounting for patient preference
apeutic impact and many patients are nonetheless refrac- and addressing their spiritual, psychological, and social care
tory. For patients with major nerve plexus invasion, referral needs.210 Care coordination for any home care services and
to chronic pain specialists for procedural interventions (eg, durable medical equipment required to support a safe dis-
nerve block or neurolysis201) may also be indicated. charge to home directly from the ED should be facilitated.
Finally, completing a same-day transfer to inpatient or home
End-of-Life Care in the ED hospice that circumvents an inpatient transition of care is
Aggressive active cancer therapy at the end of life care leads favorable. Although many systems- based barriers persist,
to poor patient outcomes and quality of life. Early referral including ED time constraints, timely access to care coor-
to palliative care services while the patient is still undergo- dination, and the uneasiness of initiating an intimate goals-
ing active disease management has been shown to minimize of-care conversation with a new patient, Quality- driven
acute care use during the last months of life.202,203 Current programs that develop this infrastructure will ameliorate
statistics indicate that >50% of patients experience at least overall management of the oncology patient in the ED.211
one acute care inpatient admission in the last 30 days of
life, with close to 60% of these admissions requiring trans- Conclusion
fer to the intensive care unit. Many of these end-stage ad- Acute care use represents a major contributor to the cost of
missions are triaged through the ED.204 Although patient oncology care and accounts for a substantial portion of the re-
factors, including strong preference for active therapy and gional variation in the cost of cancer care. Optimizing the ur-
denial of current disease state, do account for the majority of gent and emergent care of patients with cancer through timely
18 CA: A Cancer Journal for Clinicians
CA CANCER J CLIN 2022;0:1–24
symptom recognition and initiation of recommended clinical neurofilament light chain as a marker of neuronal injury212)
algorithms, including the effective triage of patients who are and the use of immunomodulators (eg, anakinra213) in the hy-
safe for discharge home, is essential for improving the quality peracute setting. Quality-based research focuses on optimiz-
and value of oncology care. Active areas of research include the ing ED-driven care coordination to facilitate direct discharge
ongoing optimization of FN clinical pathways with a focus on to hospice and improving transitions of care between the ED
refining criteria to identify patients who are sufficiently stable and the oncology hospitalist. Together, these provide a unique
for outpatient management, developing active pain-control resource for the ED physician, the outpatient oncologist, the
interventions within a 24-hour or 48-hour timeframe to man- primary care physician, and the oncology hospitalist, with the
age acute pain crises in the ED, and approaches to identify potential for improving the management of oncology patients
targeted therapeutic-related complications in the ED to de- who require urgent or emergent care. ■
velop protocols for their early management. Within the lat-
ter, efforts to improve the management of ICANS include the Acknowledgments: We acknowledge the Comprehensive Oncologic Emergency
identification of early serum-based diagnostic markers (eg, Research Network (CONCERN) consortium for their support of this article.
References A longitudinal data- linkage study in 19. Oronsky B, Ma PC, Morgensztern D,
England. Br J Cancer. 2016;115:866-875. Carter CA. Nothing but NET: a review of
1. Hsu J, Donnelly JP, Moore JX, Meneses K, neuroendocrine tumors and carcinomas.
9. National Cancer Intelligence Network,
Williams G, Wang HE. National character- Neoplasia. 2017;19:991-1002.
Public Health England. Routes to diagno-
istics of emergency department visits by 20. Ahmed M. Gastrointestinal neuro-
sis of cancer by stage, 2012-2013. Public
patients with cancer in the United States. endocrine tumors in 2020. World J
Health England; 2015. Accessed November
Am J Emerg Med. 2018;36:2038-2043. Gastrointest Oncol. 2020;12:791-807.
16, 2021. ncin.org.uk/view?rid=3071
2. Ethun CG, Bilen MA, Jani AB, Maithel 21. Ellison DH, Berl T. Clinical practice. The
10. Comber H, Sharp L, de Camargo Cancela
SK, Ogan K, Master VA. Frailty and can- syndrome of inappropriate antidiuresis.
M, Haase T, Johnson H, Pratschke J.
cer: implications for oncology surgery, N Engl J Med. 2007;356:2064-2072.
Causes and outcomes of emergency pre-
medical oncology, and radiation oncol-
sentation of rectal cancer. Int J Cancer. 22. Raftopoulos H. Diagnosis and manage-
ogy. CA Cancer J Clin. 2017;67:362-377.
2016;139:1031-1039. ment of hyponatremia in cancer patients.
3. Mayer DK, Travers D, Wyss A, Leak A, Support Care Cancer. 2007;15:1341-1347.
11. Siegel RL, Miller KD, Fuchs HE, Jemal A.
Waller A. Why do patients with cancer
Cancer statistics, 2021. CA Cancer J Clin. 23. Stewart AF. Clinical practice. Hyper
visit emergency departments? Results of a
2021;71:7-33. calcemia associated with cancer. N Engl
2008 population study in North Carolina. J Med. 2005;352:373-379.
J Clin Oncol. 2011;29:2683-2688. 12. American Society of Clinical Oncology.
Cancer.Net. Accessed November 20, 24. Khan AA, Gurnani PK, Peksa GD, Whittier
4. Gould Rothberg BE, Canavan ME, Mun S, WL, DeMott JM. Bisphosphonate ver-
2021. cancer.net/cancer-types
et al. Impact of a dedicated cancer urgent sus bisphosphonate and calcitonin for
care center on acute care utilization. JCO 13. Kao YC, Fang WL, Wang RF, et al.
the treatment of moderate to severe
Oncol Pract. 2022;18:e129-e136. Clinicopathological differences in signet
hypercalcemia of malignancy. Ann
ring cell adenocarcinoma between early
5. Hong AS, Chang H, Courtney DM, et al. Pharmacother. 2021;55:277-285.
and advanced gastric cancer. Gastric
Patterns and results of triage advice be- 25. Fizazi K, Carducci M, Smith M, et al.
Cancer. 2019;22:255-263.
fore emergency department visits made Denosumab versus zoledronic acid for
by patients with cancer. JCO Oncol Pract. 14. Lee MS, Sanoff HK. Cancer of unknown
treatment of bone metastases in men
2021;17:e564-e574. primary. BMJ. 2020;371:m4050.
with castration-
resistant prostate can-
6. Zhou Y, Abel GA, Hamilton W, et al. 15. Pelosof LC, Gerber DE. Paraneoplastic cer: a randomised, double-blind study.
Diagnosis of cancer as an emergency: a syndromes: an approach to diagnosis Lancet. 2011;377:813-822.
critical review of current evidence. Nat and treatment. Mayo Clin Proc. 2010;85:
26. LeGrand SB, Leskuski D, Zama I.
Rev Clin Oncol. 2017;14:45-56. 838-854. Narrative review: furosemide for hyper-
7. Herbert A, Abel GA, Winters S, McPhail 16. Lumachi F, Brunello A, Roma A, Basso calcemia: an unproven yet common prac-
S, Elliss-
Brookes L, Lyratzopoulos G. U. Medical treatment of malignancy- tice. Ann Intern Med. 2008;149:259-263.
Cancer diagnoses after emergency GP associated hypercalcemia. Curr Med 27. Toivanen S, Leijon H, Arola A, et al.
referral or A&E attendance in England: Chem. 2008;15:415-421. Characteristics and outcomes of the
determinants and time trends in Routes 17. Nagy-Mignotte H, Shestaeva O, Vignoud Finnish ectopic ACTH syndrome cohort.
to Diagnosis data, 2006-2015. Br J Gen L, et al. Prognostic impact of paraneo- Endocrine. 2021;74:387-395.
Pract. 2019;69:e724-e730. plastic Cushing’s syndrome in small-cell 28. Fanous N, Schwartz C, Gargus N, Casella
8. Renzi C, Lyratzopoulos G, Card T, Chu TP, lung cancer. J Thorac Oncol. 2014;9: JL. Ectopic Cushing syndrome: a rare
Macleod U, Rachet B. Do colorectal can- 497-505. cause of electrolyte derangements. Am J
cer patients diagnosed as an emergency 18. Morandi U, Casali C, Rossi G. Bronchial Med. 2020;133:e173-e176.
differ from non- emergency patients in typical carcinoid tumors. Semin Thorac 29. Giannis D, Moris D, Karachaliou GS,
their consultation patterns and symptoms? Cardiovasc Surg. 2006;18:191-198. et al. Insulinomas: from diagnosis to
VOLUME 0 | NUMBER 0 | MONTH 2022 19
Oncologic emergencies and urgencies
treatment. A review of the literature. CHEST Guideline and Expert Panel 57. Kong X, Guan J, Yang Y, Li Y, Ma W,
J BUON. 2020;25:1302-1314. Report. Chest. 2016;149:315-352. Wang R. A meta-analysis: do prophylac-
30. Krampitz GW, Norton JA. Current man- 44. Agnelli G, Becattini C, Meyer G, et al. tic antiepileptic drugs in patients with
agement of the Zollinger-Ellison syn- Apixaban for the treatment of venous brain tumors decrease the incidence
drome. Adv Surg. 2013;47:59-79. thromboembolism associated with can- of seizures? Clin Neurol Neurosurg.
cer. N Engl J Med. 2020;382:1599-1607. 2015;134:98-103.
31. Tella SH, Starr JS, Kommalapati A, Sonbol
MB, Halfdanarson TR. Management of 45. Khorana AA, Soff GA, Kakkar AK, et al. 58. Prabhakar H, Singh GP, Anand V,
well-differentiated neuroendocrine tu- Rivaroxaban for thromboprophylaxis in Kalaivani M. Mannitol versus hypertonic
mors. Clin Adv Hematol Oncol. 2021;19: high-risk ambulatory patients with can- saline for brain relaxation in patients un-
582-593. cer. N Engl J Med. 2019;380:720-728. dergoing craniotomy. Cochrane Database
46. Thomas CR Jr, Edmondson EA. Common Syst Rev. 2014;2014:CD010026.
32. Castiello RJ, Lynch PJ. Pellagra and the
carcinoid syndrome. Arch Dermatol. emergencies in cancer medicine: cardio- 59. Brown PD, Jaeckle K, Ballman KV, et al.
1972;105:574-577. vascular and neurologic syndromes. Effect of radiosurgery alone vs radiosur-
J Natl Med Assoc. 1991;83:1001-1017. gery with whole brain radiation therapy
33. Mygland A, Vincent A, Newsom- Davis
47. Sonavane SK, Milner DM, Singh SP, on cognitive function in patients with 1
J, et al. Autoantibodies in thymoma-
Abdel Aal AK, Shahir KS, Chaturvedi to 3 brain metastases: a randomized clin-
associated myasthenia gravis with my-
A. Comprehensive imaging review of ical trial. JAMA. 2016;316:401-409.
ositis or neuromyotonia. Arch Neurol.
2000;57:527-531. the superior vena cava. Radiographics. 60. Varadharajan K, Mathew R, Odutoye B,
2015;35:1873-1892. Williamson P, Madden B. Use of tracheal
34. Graus F, Dalmou J, Rene R, et al. Anti-Hu
48. Friedman T, Quencer KB, Kishore SA, stenting in the palliation of anaplastic
antibodies in patients with small- cell
lung cancer: association with complete Winokur RS, Madoff DC. Malignant thyroid carcinoma: tertiary centre experi-
response to therapy and improved sur- venous obstruction: superior vena cava ence. J Laryngol Otol. 2015;129:568-571.
vival. J Clin Oncol. 1997;15:2866-2872. syndrome and beyond. Semin Intervent 61. Rolston KVI, Nesher L. Post-obstructive
Radiol. 2017;34:398-408. pneumonia in patients with cancer: a re-
35. Graus F, Arino H, Dalmau J.
Paraneoplastic neurological syndromes 49. Kee ST, Kinoshita L, Razavi MK, Nyman view. Infect Dis Ther. 2018;7:29-38.
in Hodgkin and non- Hodgkin lympho- UR, Semba CP, Dake MD. Superior vena 62. Franke AJ, Iqbal A, Starr JS, Nair RM,
mas. Blood. 2014;123:3230-3238. cava syndrome: treatment with catheter- George TJ Jr. Management of malignant
directed thrombolysis and endovascular bowel obstruction associated with GI
36. Kimura M, Onozawa M, Fujisaki A, et al.
stent placement. Radiology. 1998;206: cancers. J Oncol Pract. 2017;13:426-434.
Anti-Ma2 paraneoplastic encephalitis as-
187-193.
sociated with testicular germ cell tumor 63. Alese OB, Kim S, Chen Z, Owonikoko
50. Tjwa ET, Holster IL, Kuipers EJ.
treated by carboplatin, etoposide and TK, El-Rayes BF. Management patterns
Endoscopic management of nonvari-
bleomycin. Int J Urol. 2008;15:942-943. and predictors of mortality among US
ceal, nonnuclear upper gastrointestinal
37. Sheikhbahaei S, Marcus CV, Fragomeni patients with cancer hospitalized for
bleeding. Gastroenterol Clin North Am.
RS, Rowe SP, Javadi MS, Solnes LB. malignant bowel obstruction. Cancer.
2014;43:707-719.
Whole-body (18)F-FDG PET and (18)F- 2015;121:1772-1778.
51. Barzilai O, Fisher CG, Bilsky MH. State
FDG PET/CT in patients with suspected 64. Vilz TO, Stoffels B, Strassburg C, Schild
of the art treatment of spinal metastatic
paraneoplastic syndrome: a systematic HH, Kalff JC. Ileus in adults. Dtsch
disease. Neurosurgery. 2018;82:757-769.
review and meta-analysis of diagnostic Arztebl Int. 2017;114:508-518.
accuracy. J Nucl Med. 2017;58:1031-1036. 52. Eckstein J, Koffler D, Parashar B, Potters
65. Sowerbutts AM, Lal S, Sremanakova J,
L, Narayana A. Guidelines for palli-
38. Thiers BH, Sahn RE, Callen JP. Cutaneous et al. Home parenteral nutrition for peo-
ative treatment of spinal metastases:
manifestations of internal malignancy. ple with inoperable malignant bowel ob-
choosing between stereotactic body ra-
CA Cancer J Clin. 2009;59:73-98. struction. Cochrane Database Syst Rev.
diation therapy and conventional frac-
39. Honnorat J, Antoine JC. Paraneoplastic tionation. Oncology (Williston Park). 2018;8:CD012812.
neurological syndromes. Orphanet J 2021;35:63-69. 66. Gomi H, Solomkin JS, Schlossberg D, et
Rare Dis. 2007;2:22. al. Tokyo guidelines 2018: antimicrobial
53. Schellinger PD, Meinck HM, Thron A.
40. Orange D, Frank M, Tian S, et al. Diagnostic accuracy of MRI compared to therapy for acute cholangitis and cho-
Cellular immune suppression in para- CCT in patients with brain metastases. lecystitis. J Hepatobiliary Pancreat Sci.
neoplastic neurologic syndromes target- J Neurooncol. 1999;44:275-281. 2018;25:3-16.
ing intracellular antigens. Arch Neurol. 67. Perone JA, Riall TS, Olino K. Palliative care
54. Esquenazi Y, Lo VP, Lee K. Critical care
2012;69:1132-1140. for pancreatic and periampullary cancer.
management of cerebral edema in brain
41. de Beukelaar JW, Sillevis Smitt PA. tumors. J Intensive Care Med. 2017;32: Surg Clin North Am. 2016;96:1415-1430.
Managing paraneoplastic neurological 15-24. 68. Duan F, Cui L, Bai Y, Li X, Yan J, Liu
disorders. Oncologist. 2006;11:292-305. 55. Ryken TC, McDermott M, Robinson PD, et X. Comparison of efficacy and compli-
42. Moore AJE, Wachsmann J, Chamarthy al. The role of steroids in the management cations of endoscopic and percutaneous
MR, Panjikaran L, Tanabe Y, Rajiah of brain metastases: a systematic review biliary drainage in malignant obstructive
P. Imaging of acute pulmonary embo- and evidence-based clinical practice guide- jaundice: a systematic review and meta-
lism: an update. Cardiovasc Diagn Ther. line. J Neurooncol. 2010;96:103-114. analysis. Cancer Imaging. 2017;17:27.
2018;8:225-243. 56. Achrol AS, Rennert RC, Anders C, et al. 69. Tan S, Tao Z, Bian X, et al. Ureteral stent
43. Kearon C, Akl EA, Ornelas J, et al. Brain metastases. Nat Rev Dis Primers. placement and percutaneous nephrostomy
Antithrombotic therapy for VTE disease: 2019;5:5. in the management of hydronephrosis
20 CA: A Cancer Journal for Clinicians
CA CANCER J CLIN 2022;0:1–24
secondary to cervical cancer. Eur J Obstet Society Pleural Disease Guideline 2010. prospective survey defining the preva-
Gynecol Reprod Biol. 2019;241:99-103. Thorax. 2010;65(suppl 2):ii32-ii40. lence, incidence, and treatment of anae-
70. Chew HK, Wun T, Harvey D, Zhou H, 83. Jeong TD, Jang S, Park CJ, Chi HS. mia in cancer patients. Eur J Cancer.
White RH. Incidence of venous throm- Prognostic relevance of pericardial effu- 2004;40:2293-2306.
boembolism and its effect on survival sion in patients with malignant diseases. 96. Family L, Xu L, Xu H, et al. The effect of
among patients with common cancers. Korean J Hematol. 2012;47:237-238. chemotherapy-induced anemia on dose
Arch Intern Med. 2006;166:458-464. 84. Hodge C, Badgwell BD. Palliation of malig- reduction and dose delay. Support Care
nant ascites. J Surg Oncol. 2019;120:67-73. Cancer. 2016;24:4263-4271.
71. Cohen AT, Katholing A, Rietbrock S,
Bamber L, Martinez C. Epidemiology of 85. Ala CK, Klein AL, Moslehi JJ. Cancer 97. Al-
Dasooqi N, Sonis ST, Bowen JM,
first and recurrent venous thromboem- treatment-associated pericardial disease: et al. Emerging evidence on the pathobi-
bolism in patients with active cancer. A epidemiology, clinical presentation, di- ology of mucositis. Support Care Cancer.
population-based cohort study. Thromb agnosis, and management. Curr Cardiol 2013;21:3233-3241.
Haemost. 2017;117:57-65. Rep. 2019;21:156. 98. Baselga J, Campone M, Piccart M, et al.
72. Wysokinski WE, Houghton DE, Casanegra 86. Sherbino J. Evidence- based emergency Everolimus in postmenopausal hormone-
AI, et al. Comparison of apixaban to rivar- medicine/rational clinical examination receptor-
positive advanced breast can-
oxaban and enoxaparin in acute cancer- abstract. Does this patient with a pericar- cer. N Engl J Med. 2012;366:520-529.
associated venous thromboembolism. Am dial effusion have cardiac tamponade? 99. McQuade RM, Stojanovska V, Abalo R,
J Hematol. 2019;94:1185-1192. Ann Emerg Med. 2009;53:390-391. Bornstein JC, Nurgali K. Chemotherapy-
73. Zimmerman S, Davis M. Rapid fire: su- 87. Antony VB, Loddenkemper R, Astoul P, induced constipation and diarrhea:
perior vena cava syndrome. Emerg Med et al. Management of malignant pleural pathophysiology, current and emerging
effusions. Eur Respir J. 2001;18:402-419. treatments. Front Pharmacol. 2016;7:414.
Clin North Am. 2018;36:577-584.
88. Howard SC, Jones DP, Pui CH. The 100. Stein A, Voigt W, Jordan K. Chemotherapy-
74. Alterio D, Turturici I, Volpe S, et al. Carotid
tumor lysis syndrome. N Engl J Med. induced diarrhea: pathophysiology, fre-
blowout syndrome after reirradiation for
2011;364:1844-1854. quency and guideline-based management.
head and neck malignancies: a compre-
Ther Adv Med Oncol. 2010;2:51-63.
hensive systematic review for a pragmatic 89. Cairo MS, Coiffier B, Reiter A, Younes
multidisciplinary approach. Crit Rev Oncol A. Recommendations for the evalua- 101. Anand A, Glatt AE. Clostridium difficile
Hematol. 2020;155:103088. tion of risk and prophylaxis of tumour infection associated with antineoplastic
lysis syndrome (TLS) in adults and chil- chemotherapy: a review. Clin Infect Dis.
75. Ito M, Niho S, Nihei K, Yoh K, Ohmatsu
dren with malignant diseases: an expert 1993;17:109-113.
H, Ohe Y. Risk factors associated with
fatal pulmonary hemorrhage in locally ad- TLS panel consensus. Br J Haematol. 102. Naymagon S, Naymagon L, Wong SY, et
vanced non-small cell lung cancer treated 2010;149:578-586. al. Acute graft-versus-host disease of the
with chemoradiotherapy. BMC Cancer. 90. Jones GL, Will A, Jackson GH, Webb NJ, gut: considerations for the gastroenter-
2012;12:27. Rule S. Guidelines for the management ologist. Nat Rev Gastroenterol Hepatol.
of tumour lysis syndrome in adults and 2017;14:711-726.
76. Papadopoulos MC, Saadoun S, Binder
DK, Manley GT, Krishna S, Verkman AS. children with haematological malignan-
103. Bledsoe TJ, Nath SK, Decker RH.
Molecular mechanisms of brain tumor cies on behalf of the British Committee Radiation pneumonitis. Clin Chest Med.
for Standards in Haematology. Br J 2017;38:201-208.
edema. Neuroscience. 2004;129:1011-1020.
Haematol. 2015;169:661-671. 104. Herrmann J. Adverse cardiac effects of can-
77. Laine FJ, Shedden AI, Dunn MM,
91. Zimmer AJ, Freifeld AG. Optimal man- cer therapies: cardiotoxicity and arrhyth-
Ghatak NR. Acquired intracranial herni-
agement of neutropenic fever in patients mia. Nat Rev Cardiol. 2020;17:474-502.
ations: MR imaging findings. AJR Am J
with cancer. J Oncol Pract. 2019;15: 105. Cardinale D, Colombo A, Lamantia G, et
Roentgenol. 1995;165:967-973.
19-24. al. Anthracycline- induced cardiomyop-
78. Barzilai O, Laufer I, Yamada Y, et al.
92. Klastersky J. Management of fever in athy: clinical relevance and response to
Integrating evidence-based medicine for
neutropenic patients with different pharmacologic therapy. J Am Coll Cardiol.
treatment of spinal metastases into a de-
risks of complications. Clin Infect Dis. 2010;55:213-220.
cision framework: neurologic, oncologic,
2004;39(suppl 1):S32-S37. 106. Armenian SH, Lacchetti C, Barac A,
mechanicals stability, and systemic dis-
ease. J Clin Oncol. 2017;35:2419-2427. 93. Baluch A, Shewayish S. Neutropenic et al. Prevention and monitoring of car-
fever. In: Velez AP, Lamarche J, Greene diac dysfunction in survivors of adult
79. Prasad D, Schiff D. Malignant spinal-cord
JN, eds. Infections in Neutropenic cancers: American Society of Clinical
compression. Lancet Oncol. 2005;6:15-24.
Cancer Patients. Springer; 2019:105-116. Oncology Clinical Practice Guideline.
80. Avenia N, Vannucci J, Monacelli M, et J Clin Oncol. 2017;35:893-911.
94. Carmona-Bayonas A, Jimenez-Fonseca
al. Thyroid cancer invading the airway:
P, Virizuela Echaburu J, et al. Prediction
107. Lipe DN, Mann PB, Babakhanlou
diagnosis and management. Int J Surg.
of serious complications in patients with R, Cruz Carreras MT, Guido Hita A,
2016;28(suppl 1):S75-S78.
seemingly stable febrile neutropenia: Wattana MK. Evaluation and manage-
81. Troncone E, Fugazza A, Cappello A, validation of the Clinical Index of Stable ment of genitourinary emergencies in
et al. Malignant gastric outlet obstruc- Febrile Neutropenia in a prospective co- patients with cancer. Emerg Med Int.
tion: which is the best therapeutic option? hort of patients from the FINITE study. 2021;2021:4511968.
World J Gastroenterol. 2020;26:1847-1860. J Clin Oncol. 2015;33:465-471. 108. Payne H, Adamson A, Bahl A, et al.
82. Roberts ME, Neville E, Berrisford RG, 95. Ludwig H, Van Belle S, Barrett-
Lee P, Chemical-and radiation-induced haem-
Antunes G, Ali NJ. Management of a ma- et al. The European Cancer Anaemia orrhagic cystitis: current treatments and
lignant pleural effusion: British Thoracic Survey (ECAS): a large, multinational, challenges. BJU Int. 2013;112:885-897.
VOLUME 0 | NUMBER 0 | MONTH 2022 21
Oncologic emergencies and urgencies
109. Livshits Z, Rao RB, Smith SW. An ap- score: 10 years of use for identifying low- 133. Sodergren SC, White A, Efficace F, et al.
proach to chemotherapy- associated risk febrile neutropenic cancer patients. Systematic review of the side effects as-
toxicity. Emerg Med Clin North Am. Support Care Cancer. 2013;21:1487-1495. sociated with tyrosine kinase inhibitors
2014;32:167-203. 121. Klastersky J, Paesmans M, Georgala A, used in the treatment of gastrointestinal
110. Hesketh PJ, Kris MG, Basch E, et al. et al. Outpatient oral antibiotics for fe- stromal tumours on behalf of the EORTC
Antiemetics: American Society of Clinical brile neutropenic cancer patients using a Quality of Life Group. Crit Rev Oncol
Oncology Clinical Practice Guideline score predictive for complications. J Clin Hematol. 2014;91:35-46.
Update. J Clin Oncol. 2017;35:3240-3261. Oncol. 2006;24:4129-4134.
134. Shah DR, Shah RR, Morganroth J.
111. Park HJ, Lee JH, Kim SR, et al. A new 122. Watkins T, Surowiecka MK, McCullough Tyrosine kinase inhibitors: their on-
practical desensitization protocol for J. Transfusion indications for patients with target toxicities as potential indicators of
oxaliplatin-
induced immediate hyper- cancer. Cancer Control. 2015;22:38-46. efficacy. Drug Saf. 2013;36:413-426.
sensitivity reactions: a necessary and 135. Zhong L, Li Y, Xiong L, et al. Small mole-
123. Schoen MW, Hoque S, Witherspoon BJ,
useful approach. J Investig Allergol Clin cules in targeted cancer therapy: advances,
et al. End of an era for erythropoiesis-
Immunol. 2016;26:168-176. challenges, and future perspectives. Signal
stimulating agents in oncology. Int J
112. Ohmachi K, Tobinai K, Kinoshita T, et al. Cancer. 2020;146:2829-2835. Transduct Target Ther. 2021;6:201.
Efficacy and safety of obinutuzumab in 136. Rapoport BL, Cooksley T, Johnson DB,
124. Chao AW, Bhatti M, DuPont HL, Nataro
patients with previously untreated fol- Anderson R. Supportive care for new
JP, Carlin LG, Okhuysen PC. Clinical
licular lymphoma: a subgroup analysis cancer therapies. Curr Opin Oncol.
features and molecular epidemiology
of patients enrolled in Japan in the ran- 2021;33:287-294.
of diarrheagenic Escherichia coli patho-
domized phase III GALLIUM trial. Int J
types identified by fecal gastrointestinal 137. Lacouture ME. Mechanisms of cutane-
Hematol. 2018;108:499-509.
multiplex nucleic acid amplification in ous toxicities to EGFR inhibitors. Nat
113. Amitai I, Gafter-Gvili A, Shargian-Alon patients with cancer and diarrhea. Diagn Rev Cancer. 2006;6:803-812.
L, Raanani P, Gurion R. Obinutuzumab- Microbiol Infect Dis. 2017;89:235-240.
related adverse events: a systematic re-
138. Joshi SS, Ortiz S, Witherspoon JN,
125. Li CW, Chen PL, Lee NY, et al. Non- et al. Effects of epidermal growth fac-
view and meta-analysis. Hematol Oncol.
typhoidal Salmonella bacteremia among tor receptor inhibitor-induced dermato-
2021;39:215-221.
adults: an adverse prognosis in patients logic toxicities on quality of life. Cancer.
114. Wong JT, Long A. Rituximab hypersen- with malignancy. J Microbiol Immunol 2010;116:3916-3923.
sitivity: evaluation, desensitization, and Infect. 2012;45:343-349.
potential mechanisms. J Allergy Clin
139. Lipworth AD, Robert C, Zhu AX.
126. Guh AY, Kutty PK. Clostridioides dif- Hand- foot syndrome (hand- foot skin
Immunol Pract. 2017;5:1564-1571.
ficile infection. Ann Intern Med. reaction, palmar- plantar erythrodyses-
115. Cairo MS, Bishop M. Tumour lysis
2018;169:ITC49-ITC64. thesia): focus on sorafenib and sunitinib.
syndrome: new therapeutic strate-
127. Ruutu T, Gratwohl A, de Witte T, et al. Oncology. 2009;77:257-271.
gies and classification. Br J Haematol.
2004;127:3-11. Prophylaxis and treatment of GVHD:
140. Urakawa R, Tarutani M, Kubota K,
EBMT-ELN Working Group recommen- Uejima E. Hand foot syndrome has
116. Bosly A, Sonet A, Pinkerton CR, et al.
dations for a standardized practice. Bone the strongest impact on QOL in skin
Rasburicase (recombinant urate oxi-
Marrow Transplant. 2014;49:168-173. toxicities of chemotherapy. J Cancer.
dase) for the management of hyperurice-
128. Waller EK, Miklos D, Cutler C, et al. 2019;10:4846-4851.
mia in patients with cancer: report of an
international compassionate use study. Ibrutinib for chronic graft-
versus-
host 141. Riondino S, Del Monte G, Fratangeli F,
Cancer. 2003;98:1048-1054. disease after failure of prior therapy: Guadagni F, Roselli M, Ferroni P. Anti-
1-
year update of a phase 1b/2 study. angiogenic drugs, vascular toxicity
117. Daniels LM, Durani U, Barreto JN, et al.
Biol Blood Marrow Transplant. 2019;25: and thromboembolism in solid cancer.
Impact of time to antibiotic on hospital
2002-2007. Cardiovasc Hematol Agents Med Chem.
stay, intensive care unit admission, and
mortality in febrile neutropenia. Support
129. Zeiser R, Polverelli N, Ram R, et al. 2017;15:3-16.
Care Cancer. 2019;27:4171-4177. Ruxolitinib for glucocorticoid-refractory
142. Fugate JE, Rabinstein AA. Posterior
chronic graft-versus-host disease. N Engl reversible encephalopathy syndrome:
118. Niessen FA, van Mourik MSM, Bruns
J Med. 2021;385:228-238. clinical and radiological manifestations,
AHW, Raijmakers RAP, de Groot MCH,
van der Bruggen T. Early discontinua-
130. Jagasia M, Lazaryan A, Bachier CR, pathophysiology, and outstanding ques-
tion of empirical antibiotic treatment in et al. ROCK2 inhibition with belumosudil tions. Lancet Neurol. 2015;14:914-925.
neutropenic patients with acute myeloid (KD025) for the treatment of chronic
143. Shaharir SS, Remli R, Marwan AA,
leukaemia and high-risk myelodysplas- graft-versus-host disease. J Clin Oncol. Said MS, Kong NC. Posterior reversible
tic syndrome. Antimicrob Resist Infect 2021;39:1888-1898. encephalopathy syndrome in systemic
Control. 2020;9:74. 131. Liu SN, Zhang XH, Xu LP, et al. Prognostic lupus erythematosus: pooled analysis of
119. Chen K, Wang Q, Pleasants RA, et al. factors and long- term follow- up of the literature reviews and report of six
Empiric treatment against invasive fungal basiliximab for steroid-refractory acute new cases. Lupus. 2013;22:492-496.
diseases in febrile neutropenic patients: graft-
versus-
host disease: updated ex-
144. Koulaouzidis G, Yung AE, Yung DE,
a systematic review and network meta- perience from a large-scale study. Am J et al. Conventional cardiac risk factors
analysis. BMC Infect Dis. 2017;17:159. Hematol. 2020;95:927-936. associated with trastuzumab- induced
120. Klastersky J, Paesmans M. The 132. Manikandan R, Kumar S, Dorairajan LN. cardiotoxicity in breast cancer: system-
Multinational Association for Supportive Hemorrhagic cystitis: a challenge to the atic review and meta-analysis. Curr Probl
Care in Cancer (MASCC) risk index urologist. Indian J Urol. 2010;26:159-166. Cancer. 2021;45:100723.
22 CA: A Cancer Journal for Clinicians
CA CANCER J CLIN 2022;0:1–24
145. Barish R, Gates E, Barac A. Trastuzumab- 159. Park JH, Riviere I, Gonen M, et al. Long- of dermatologic adverse events to agents
induced cardiomyopathy. Cardiol Clin. term follow-up of CD19 CAR therapy in targeting the PD-1 receptor. Eur J Cancer.
2019;37:407-418. acute lymphoblastic leukemia. N Engl J 2016;60:12-25.
146. Jerusalem G, Lancellotti P, Kim SB. HER2+ Med. 2018;378:449-459. 172. Rajha E, Chaftari P, Kamal M, Maamari
breast cancer treatment and cardiotoxic- 160. Maude SL, Laetsch TW, Buechner J, et al. J, Chaftari C, Yeung SJ. Gastrointestinal
ity: monitoring and management. Breast Tisagenlecleucel in children and young adverse events associated with im-
Cancer Res Treat. 2019;177:237-250. adults with B-cell lymphoblastic leuke- mune checkpoint inhibitor therapy.
147. Ricart AD. Antibody-drug conjugates of mia. N Engl J Med. 2018;378:439-448. Gastroenterol Rep (Oxf). 2020;8:25-30.
calicheamicin derivative: gemtuzumab 161. Neelapu SS, Locke FL, Bartlett NL, et al. 173. Dougan M, Wang Y, Rubio-Tapia A, Lim
ozogamicin and inotuzumab ozogami- Axicabtagene ciloleucel CAR T-cell ther- JK. AGA clinical practice update on di-
cin. Clin Cancer Res. 2011;17:6417-6427. apy in refractory large B-cell lymphoma. agnosis and management of immune
148. Sharma P, Allison JP. Dissecting the N Engl J Med. 2017;377:2531-2544. checkpoint inhibitor colitis and hepa-
mechanisms of immune checkpoint ther- 162. Newick K, O’Brien S, Moon E, Albelda titis: expert review. Gastroenterology.
apy. Nat Rev Immunol. 2020;20:75-76. SM. CAR T cell therapy for solid tumors. 2021;160:1384-1393.
149. Lipson EJ, Drake CG. Ipilimumab: an anti- Annu Rev Med. 2017;68:139-152. 174. Faje A. Immunotherapy and hypophysitis:
CTLA-4 antibody for metastatic melanoma.
163. Santomasso B, Bachier C, Westin J, clinical presentation, treatment, and bio-
Clin Cancer Res. 2011;17:6958-6962. Rezvani K, Shpall EJ. The other side of logic insights. Pituitary. 2016;19:82-92.
150. Lin X, Lu X, Luo G, Xiang H. Progress CAR T-cell therapy: cytokine release syn- 175. Wu J, Lacouture ME. Pruritus associ-
in PD-1/PD-L1 pathway inhibitors: from drome, neurologic toxicity, and financial ated with targeted anticancer therapies
biomacromolecules to small molecules. burden. Am Soc Clin Oncol Educ Book. and their management. Dermatol Clin.
Eur J Med Chem. 2020;186:111876. 2019;39:433-444. 2018;36:315-324.
151. Lipson EJ, Tawbi HA, Schadendorf D, 164. Tsimboukis S, Merikas I, Karapanagiotou
176. de Filette J, Jansen Y, Schreuer M,
et al. Relatlimab (RELA) plus nivolumab EM, Saif MW, Syrigos KN. Erlotinib- et al. Incidence of thyroid-related adverse
(NIVO) versus NIVO in first-line advanced induced skin rash in patients with non- events in melanoma patients treated
melanoma: primary phase III results from small-cell lung cancer: pathogenesis, with pembrolizumab. J Clin Endocrinol
RELATIVITY-047 (CA224-047) [abstract]. clinical significance, and management. Metab. 2016;101:4431-4439.
J Clin Oncol. 2021;39(15 suppl):9503. Clin Lung Cancer. 2009;10:106-111.
177. Maamari J, Yeung SJ, Chaftari PS.
152. Sullivan RJ, Weber JS. Immune- related 165. Chu CY, Choi J, Eaby-Sandy B, Langer Diabetic ketoacidosis induced by a sin-
toxicities of checkpoint inhibitors: mech- CJ, Lacouture ME. Osimertinib: a novel gle dose of pembrolizumab. Am J Emerg
anisms and mitigation strategies. Nat Rev dermatologic adverse event profile in Med. 2019;37:376.e371-376.e372.
Drug Discov. Published online July 27, patients with lung cancer. Oncologist. 178. Suresh K, Naidoo J, Lin CT, Danoff S.
2021. doi:10.1038/s41573-021-00259-5 2018;23:891-899. Immune checkpoint immunotherapy
153. Carlino MS, Larkin J, Long GV. Immune 166. Petrelli F, Borgonovo K, Barni S. The pre- for non-
small cell lung cancer: bene-
checkpoint inhibitors in melanoma. dictive role of skin rash with cetuximab fits and pulmonary toxicities. Chest.
Lancet. 2021;398:1002-1014. and panitumumab in colorectal cancer 2018;154:1416-1423.
patients: a systematic review and meta- 179. Steven NM, Fisher BA. Management of
154. Abdel-Wahab N, Shah M, Suarez-Almazor
analysis of published trials. Target Oncol. rheumatic complications of immune
ME. Adverse events associated with im-
2013;8:173-181. checkpoint inhibitor therapy— an on-
mune checkpoint blockade in patients
with cancer: a systematic review of case 167. Nikolaou V, Syrigos K, Saif MW. Incidence cological perspective. Rheumatology
reports. PLoS One. 2016;11:e0160221. and implications of chemotherapy re- (Oxford). 2019;58(suppl 7):vii29-vii39.
lated hand-foot syndrome. Expert Opin 180. Cortazar FB, Marrone KA, Troxell ML,
155. Hodi FS, Chiarion- Sileni V, Gonzalez
Drug Saf. 2016;15:1625-1633. et al. Clinicopathological features of
R, et al. Nivolumab plus ipilimumab
or nivolumab alone versus ipilimumab 168. Al Beihany A, Al Omar H, Sahovic E, acute kidney injury associated with im-
alone in advanced melanoma (CheckMate et al. Successful treatment of hepatic mune checkpoint inhibitors. Kidney Int.
067): 4-
year outcomes of a multicentre, veno-occlusive disease after myeloablative 2016;90:638-647.
randomised, phase 3 trial. Lancet Oncol. allogeneic hematopoietic stem cell trans- 181. Cunningham ET, Moorthy RS, Zierhut M.
2018;19:1480-1492. plantation by early administration of a Immune checkpoint inhibitor- induced
short course of methylprednisolone. Bone uveitis. Ocul Immunol Inflamm. 2020;28:
156. Brahmer JR, Lacchetti C, Schneider BJ,
Marrow Transplant. 2008;41:287-291. 847-849.
et al. Management of immune- related
adverse events in patients treated with 169. Ho VT, Revta C, Richardson PG. Hepatic 182. Escudier M, Cautela J, Malissen N, et al.
immune checkpoint inhibitor therapy: veno-occlusive disease after hemato- Clinical features, management, and out-
American Society of Clinical Oncology poietic stem cell transplantation: up- comes of immune checkpoint inhibitor-
Clinical Practice Guideline. J Clin Oncol. date on defibrotide and other current related cardiotoxicity. Circulation.
2018;36:1714-1768. investigational therapies. Bone Marrow 2017;136:2085-2087.
Transplant. 2008;41:229-237.
157. Schuster SJ, Bishop MR, Tam CS, et al.
183. Sadaat M, Jang S. Hemophagocytic
Tisagenlecleucel in adult relapsed or re- 170. Touyz RM, Herrmann SMS, Herrmann lymphohistiocytosis with immuno-
fractory diffuse large B-cell lymphoma. J. Vascular toxicities with VEGF inhib- therapy: brief review and case report.
N Engl J Med. 2019;380:45-56. itor therapies-focus on hypertension J Immunother Cancer. 2018;6:49.
and arterial thrombotic events. J Am Soc
158. Holstein SA, Lunning MA. CAR T- cell 184. Lee DW, Gardner R, Porter DL, et al.
Hypertens. 2018;12:409-425.
therapy in hematologic malignancies: a Current concepts in the diagnosis and
voyage in progress. Clin Pharmacol Ther.
171. Belum VR, Benhuri B, Postow MA, management of cytokine release syn-
2020;107:112-122. et al. Characterisation and management drome. Blood. 2014;124:188-195.
VOLUME 0 | NUMBER 0 | MONTH 2022 23
Oncologic emergencies and urgencies
185. Riegler LL, Jones GP, Lee DW. Current of constipation in advanced cancer: for outcomes and risks of treatments
approaches in the grading and manage- ESMO Clinical Practice Guidelines. Ann (SUPPORT). The SUPPORT Principal
ment of cytokine release syndrome after Oncol. 2018;29(suppl 4):iv111-iv125. Investigators. JAMA. 1995;274:1591-1598.
chimeric antigen receptor T-cell therapy. 196. Rao VL, Micic D, Davis AM. Medical 207. American College of Emergency
Ther Clin Risk Manag. 2019;15:323-335. management of opioid- induced consti- Physicians. Five Things Physicians and
186. Coyne CJ, Reyes-Gibby CC, Durham DD, pation. JAMA. 2019;322:2241-2242. Patients Should Question: 3. Don’t delay
et al. Cancer pain management in the engaging available palliative and hos-
197. Howlett C, Gonzalez R, Yerram P, Faley
emergency department: a multicenter pice care services in the emergency de-
B. Use of naloxone for reversal of life-
prospective observational trial of the partment for patients likely to benefit.
threatening opioid toxicity in cancer-
Comprehensive Oncologic Emergencies Choosing Wisely (an initiative of the
related pain. J Oncol Pharm Pract. 2016;22:
Research Network (CONCERN). Support American Board of Internal Medicine
114-120.
Care Cancer. 2021;29:4543-4553. [ABIM] Foundation). American College
198. Barreto SG, Saccone GT. Pancreatic
187. Glare PA, Davies PS, Finlay E, et al. of Emergency Physicians; 2013. Accessed
nociception— revisiting the physiology
Pain in cancer survivors. J Clin Oncol. November 16, 2021. acep.org/globalasse
and pathophysiology. Pancreatology.
2014;32:1739-1747. ts/uploads/uploaded-f iles/acep/membe
2012;12:104-112.
188. Patel PM, Goodman LF, Knepel SA, rship/chapters/grants/choosing-w isley-
199. Brewer JR, Morrison G, Dolan ME, Fleming 5-things-phys.pdf
et al. Evaluation of emergency depart-
GF. Chemotherapy- induced peripheral
ment management of opioid- tolerant 208. Kaplan M. SPIKES: a framework for
neuropathy: current status and progress.
cancer patients with acute pain. J Pain breaking bad news to patients with can-
Gynecol Oncol. 2016;140:176-183.
Symptom Manage. 2017;54:501-507. cer. Clin J Oncol Nurs. 2010;14:514-516.
200. McNicol ED, Midbari A, Eisenberg E.
189. Equianalgesic guide for adults and 209. Childers JW, Back AL, Tulsky JA, Arnold
Opioids for neuropathic pain. Cochrane
children with communication tool. In: RM. REMAP: a framework for goals
Database Syst Rev. 2013;8:CD006146.
Quill TE, Periyakoil V, Denney-Koelsch of care conversations. J Oncol Pract.
E, White P, Zhukovsky D. Primer 201. Sachdev AH, Gress FG. Celiac plexus block 2017;13:e844-e850.
of Palliative Care. 7th ed. American and neurolysis: a review. Gastrointest
210. George N, Bowman J, Aaronson E, Ouchi
Academy of Hospice and Palliative Care Endosc Clin N Am. 2018;28:579-586.
K. Past, present, and future of palliative
Medicine; 2019. 202. Temel JS, Greer JA, Muzikansky A, et care in emergency medicine in the USA.
190. Hagen NA, Elwood T, Ernst S. Cancer pain al. Early palliative care for patients with Acute Med Surg. 2020;7:e497.
emergencies: a protocol for management. metastatic non-small-cell lung cancer. N
211. Rege RM, Peyton K, Pajka SE, Grudzen
J Pain Symptom Manage. 1997;14:45-50. Engl J Med. 2010;363:733-742.
CR, Conroy MJ, Southerland LT.
191. Schneider G, Voltz R, Gaertner J. Cancer 203. Prigerson HG, Bao Y, Shah MA, et al. Arranging hospice care from the emer-
pain management and bone metastases: Chemotherapy use, performance sta- gency department: a single center retro-
an update for the clinician. Breast Care tus, and quality of life at the end of life. spective study. J Pain Symptom Manage.
(Basel). 2012;7:113-120. JAMA Oncol. 2015;1:778-784. 2022;63:e281-e286.
192. Jairam V, Yang DX, Yu JB, Park HS. 204. McDermott CL, Fedorenko C, 212. Schoeberl F, Tiedt S, Schmitt A, et al.
Emergency department visits for opioid Kreizenbeck K, et al. End-of-life services Neurofilament light chain serum levels
overdoses among patients with cancer. among patients with cancer: evidence correlate with the severity of neurotox-
J Natl Cancer Inst. 2020;112:938-943. from cancer registry records linked with icity after CAR T cell treatment. Blood
193. Droney J, Levy J, Quigley C. Prescribing commercial health insurance claims. Adv. Published online ahead of print
opioids in renal failure. J Opioid Manag. J Oncol Pract. 2017;13:e889-e899. January 18, 2022. doi:10.1182/blood
2007;3:309-316. 205. Weeks JC, Catalano PJ, Cronin A, et al. advances.2021006144
194. Soleimanpour H, Safari S, Shahsavari Nia Patients’ expectations about effects of 213. Wehrli M, Gallagher K, Chen YB, et al.
K, Sanaie S, Alavian SM. Opioid drugs in chemotherapy for advanced cancer. N Single-center experience using anakinra
patients with liver disease: a systematic Engl J Med. 2012;367:1616-1625. for steroid-refractory immune effector
review. Hepat Mon. 2016;16:e32636. 206. A controlled trial to improve care for seri- cell-
associated neurotoxicity syndrome
195. Larkin PJ, Cherny NI, La Carpia D, et al. ously ill hospitalized patients. The study (ICANS). J Immunother Cancer. 2022;10:
Diagnosis, assessment and management to understand prognoses and preferences e003847.
24 CA: A Cancer Journal for Clinicians
You might also like
- Understanding Non-Hodgkin Lymphoma. A Guide for Patients, Survivors, and Loved Ones. September 2015From EverandUnderstanding Non-Hodgkin Lymphoma. A Guide for Patients, Survivors, and Loved Ones. September 2015No ratings yet
- Management of Hereditary Colorectal Cancer: A Multidisciplinary ApproachFrom EverandManagement of Hereditary Colorectal Cancer: A Multidisciplinary ApproachJose G. GuillemNo ratings yet
- Oncologic Emergencies and Urgencies A Comprehensive ReviewDocument24 pagesOncologic Emergencies and Urgencies A Comprehensive ReviewJulio MineraNo ratings yet
- Oncological Emergencies From Pathophysiology and Diagnosis To Treatment: A Narrative ReviewDocument22 pagesOncological Emergencies From Pathophysiology and Diagnosis To Treatment: A Narrative ReviewDeni IrwandiNo ratings yet
- Emergencias OncológicasDocument33 pagesEmergencias OncológicasNathaly GallosoNo ratings yet
- NeutropeniaDocument17 pagesNeutropeniaassajadda lizikriNo ratings yet
- Distal Cholangiocarcinoma and Pancreas Adenocarcinoma Ethun2016Document8 pagesDistal Cholangiocarcinoma and Pancreas Adenocarcinoma Ethun2016DannyNo ratings yet
- JCO 2014 Ñamendys Silva 1169 70Document2 pagesJCO 2014 Ñamendys Silva 1169 70Eward Rod SalNo ratings yet
- AML 10 Palliative NursingDocument5 pagesAML 10 Palliative NursingutamiprakosoNo ratings yet
- Geriatric Syndromes in Elderly Patients Admitted To An Oncology-Acute Care For Elders UnitDocument6 pagesGeriatric Syndromes in Elderly Patients Admitted To An Oncology-Acute Care For Elders UnitYuliana Eka SintaNo ratings yet
- Medicine American Journal of Hospice and PalliativeDocument6 pagesMedicine American Journal of Hospice and Palliativem1k0eNo ratings yet
- Baugh Et Al-2017-Academic Emergency MedicineDocument9 pagesBaugh Et Al-2017-Academic Emergency MedicineRovanNo ratings yet
- Fertility Preservation in Pediatric Leukemia and LymphomaDocument11 pagesFertility Preservation in Pediatric Leukemia and LymphomaElianaNo ratings yet
- PBC 27293Document8 pagesPBC 27293RadenSiwi Bagus HadhiningratNo ratings yet
- Cam4 6 1861Document10 pagesCam4 6 1861Ćatke TkećaNo ratings yet
- Rapid Access Multidisciplinary Lymph Node Diagnostic Clinic: Analysis of 550 PatientsDocument8 pagesRapid Access Multidisciplinary Lymph Node Diagnostic Clinic: Analysis of 550 PatientsAna GómezNo ratings yet
- Challenges and Outcome of Wilms' Tumour Management in A Resource-Constrained SettingDocument3 pagesChallenges and Outcome of Wilms' Tumour Management in A Resource-Constrained Settingcallisto3487No ratings yet
- Hiperkalsemia MalignancyDocument7 pagesHiperkalsemia MalignancyM. Abdurrahman Al-HaraaniNo ratings yet
- MC m6 Cancer+ovario+precozDocument9 pagesMC m6 Cancer+ovario+precozGrecia Castro CNo ratings yet
- Objective: Breast Cancer Is The Most Common Type of Cancer Found in Women, in The United StatesDocument5 pagesObjective: Breast Cancer Is The Most Common Type of Cancer Found in Women, in The United StatesdwiNo ratings yet
- Dissertation LeukemiaDocument4 pagesDissertation LeukemiaCustomPapersOnlineSaltLakeCity100% (1)
- ST Gallen 2021 A OncologyDocument20 pagesST Gallen 2021 A OncologyJorge Apolo PinzaNo ratings yet
- Haematologic EmergenciesDocument33 pagesHaematologic Emergenciessalmamaged7619No ratings yet
- Guia para El MedicoDocument6 pagesGuia para El MedicoJuan Sebastian OrdoñezNo ratings yet
- Systemic Therapy For Advanced Appendiceal Adenocarcinoma: An Analysis From The NCCN Oncology Outcomes Database For Colorectal CancerDocument8 pagesSystemic Therapy For Advanced Appendiceal Adenocarcinoma: An Analysis From The NCCN Oncology Outcomes Database For Colorectal Canceralberto cabelloNo ratings yet
- Alok A. Khorana - Incidence and Predictors of Venous Thromboembolism (VTE) Among Ambulatory High-RiskDocument8 pagesAlok A. Khorana - Incidence and Predictors of Venous Thromboembolism (VTE) Among Ambulatory High-RiskFarid RakhmanNo ratings yet
- Ournal of Linical Ncology: PurposeDocument11 pagesOurnal of Linical Ncology: PurposeRicky Cornelius TariganNo ratings yet
- HF 1Document14 pagesHF 1Galuh EkaNo ratings yet
- Aldrink2018 DikonversiDocument31 pagesAldrink2018 DikonversiNadenka BellaNo ratings yet
- Dose-Adjusted Enoxaparin Thromboprophylaxis in Hospitalized CancerDocument7 pagesDose-Adjusted Enoxaparin Thromboprophylaxis in Hospitalized CancerAnonymous 9dVZCnTXSNo ratings yet
- Cancer Immunology IntroductionDocument8 pagesCancer Immunology IntroductionMariana NannettiNo ratings yet
- Leucemia Aguda en El Embarazo, 2021Document10 pagesLeucemia Aguda en El Embarazo, 2021AdrianNo ratings yet
- Asco GCSF 2015Document16 pagesAsco GCSF 2015Alvy SyukrieNo ratings yet
- Breast Cancer Guidelines OverviewDocument23 pagesBreast Cancer Guidelines OverviewRodney MatthewsNo ratings yet
- Guideline Implementation For Breast Healthcare in Low-Income and Middle-Income CountriesDocument23 pagesGuideline Implementation For Breast Healthcare in Low-Income and Middle-Income Countriesrubensosa16No ratings yet
- Cancer de PancreasDocument12 pagesCancer de PancreasRuben RoaNo ratings yet
- Cancer y Inmunosupresor en EtcDocument6 pagesCancer y Inmunosupresor en EtcANDONIS30No ratings yet
- Predictors For Single Agent Resistance in FIGO Score 5 or 6 Gestational Trophoblastic NeoplasiaDocument11 pagesPredictors For Single Agent Resistance in FIGO Score 5 or 6 Gestational Trophoblastic NeoplasiaKim RamirezNo ratings yet
- Adjuvant Chemotherapy Is Not Associated With A Survival Benefit ForDocument6 pagesAdjuvant Chemotherapy Is Not Associated With A Survival Benefit ForHerry SasukeNo ratings yet
- Primer: Hepatocellular CarcinomaDocument28 pagesPrimer: Hepatocellular CarcinomaAinun Aii NoorNo ratings yet
- Borderline Ovarian Cancer: Understanding Tumors of Low Malignant PotentialDocument8 pagesBorderline Ovarian Cancer: Understanding Tumors of Low Malignant Potentialamarendra WardhanaNo ratings yet
- 247 FullDocument10 pages247 FullMeidianty TandiNo ratings yet
- Adult Acute Lymphoblastic LeukemiaDocument22 pagesAdult Acute Lymphoblastic Leukemiamelki hadisasmitaNo ratings yet
- Pediatric Cancer in Perspective: Cure NOT: IS EnoughDocument5 pagesPediatric Cancer in Perspective: Cure NOT: IS EnoughKaren MacDonaldNo ratings yet
- Incidence and Risk Factors For Ventilator Associated Pneumon 2007 RespiratorDocument6 pagesIncidence and Risk Factors For Ventilator Associated Pneumon 2007 RespiratorTomasNo ratings yet
- 2020 Article 2138Document10 pages2020 Article 2138Andi Tiara S. AdamNo ratings yet
- Acute Myeloid Leukemia ThesisDocument5 pagesAcute Myeloid Leukemia ThesisBuyCheapEssayOmaha100% (2)
- Ricardo - Management of Lung Nodules and Lung Cancer Screening During COVIDDocument10 pagesRicardo - Management of Lung Nodules and Lung Cancer Screening During COVIDCIRUGIA CARDIOTORÁCICA MINIMAMENTE INVASIVANo ratings yet
- KeperawatanDocument8 pagesKeperawatanRyan FaisaldoNo ratings yet
- Understanding Non-Hodgkin Lymphoma. A Guide for Patients, Survivors, and Loved Ones. April 2021From EverandUnderstanding Non-Hodgkin Lymphoma. A Guide for Patients, Survivors, and Loved Ones. April 2021No ratings yet
- 0413 Massive Upper GI Bleeding PDFDocument12 pages0413 Massive Upper GI Bleeding PDFhectulNo ratings yet
- Journal Pone 0262151Document16 pagesJournal Pone 0262151pablo rubenNo ratings yet
- 775 FullDocument9 pages775 FullidaNo ratings yet
- OvarDocument52 pagesOvarAndrei BuruianăNo ratings yet
- Childhood Acute Lymphoblastic Leukemia Treatment (PDQ®) - National Cancer InstituteDocument135 pagesChildhood Acute Lymphoblastic Leukemia Treatment (PDQ®) - National Cancer Institutealejandro1122100% (1)
- 10 14338 - Ijpt-22-00021 1Document12 pages10 14338 - Ijpt-22-00021 1Raul Matute MartinNo ratings yet
- Ol 20 1 441 PDFDocument7 pagesOl 20 1 441 PDFeka satyani belinaNo ratings yet
- Cpho023 02 07Document9 pagesCpho023 02 07Kyung-Nam KohNo ratings yet
- Af13e6df 9c91 4284 A3ae Feb2bacbcba4Document7 pagesAf13e6df 9c91 4284 A3ae Feb2bacbcba4alberto cabelloNo ratings yet
- Clinical Presentation of Childhood Leukaemia: A Systematic Review and Meta-AnalysisDocument9 pagesClinical Presentation of Childhood Leukaemia: A Systematic Review and Meta-AnalysisPrima YosiNo ratings yet
- Evaluation of Acute Abdominal PainDocument4 pagesEvaluation of Acute Abdominal PainEdison Tan SantamariaNo ratings yet
- Acute Indigestion of The AbdomenDocument11 pagesAcute Indigestion of The AbdomenSyukrina Nur rahayuNo ratings yet
- 8319 - Akut Abdomen Pada AnakDocument20 pages8319 - Akut Abdomen Pada AnakAdi daradiNo ratings yet
- Abdominal AssessmentDocument44 pagesAbdominal Assessmentdbryant010191% (11)
- Soal Compile Gastrointestinal System 2014Document22 pagesSoal Compile Gastrointestinal System 2014Della Tamara RindasiwiNo ratings yet
- Common Illnesses: 1. Write The Correct Illness After Reading The Clues. Each Illness Has Two CluesDocument4 pagesCommon Illnesses: 1. Write The Correct Illness After Reading The Clues. Each Illness Has Two Cluesmcarmendgj74No ratings yet
- Are All Abdominal Pains the Same? Understanding Visceral Pain and the Role of AntispasmodicsDocument41 pagesAre All Abdominal Pains the Same? Understanding Visceral Pain and the Role of AntispasmodicsSamuel SilabanNo ratings yet
- A Gastro Tahun Lalu - Tahun IniDocument12 pagesA Gastro Tahun Lalu - Tahun IniDapot SianiparNo ratings yet
- Surgery II - Topical Past Papers (2007-2019)Document61 pagesSurgery II - Topical Past Papers (2007-2019)AnmahNo ratings yet
- Appendicitis Spring 20 Digestive ClassDocument74 pagesAppendicitis Spring 20 Digestive Classalice de los santosNo ratings yet
- DR. ANTONIO P. CABUGAO vs. PEOPLE - G.R. No. 163879 - July 30, 2014 - DIGEST PDFDocument2 pagesDR. ANTONIO P. CABUGAO vs. PEOPLE - G.R. No. 163879 - July 30, 2014 - DIGEST PDFAaron Ariston100% (1)
- Williams Gynecology PDFDriveDocument25 pagesWilliams Gynecology PDFDriveKawaii Rjen-chanNo ratings yet
- Pre-And Post-Book Study Test For The Shelf Exam: How To Use This ChapterDocument6 pagesPre-And Post-Book Study Test For The Shelf Exam: How To Use This ChapterMiguel CuevasNo ratings yet
- Small bowel obstructionDocument11 pagesSmall bowel obstructionRace MendezNo ratings yet
- 2023 Surgery Viva ReleaseDocument5 pages2023 Surgery Viva ReleaseduncanNo ratings yet
- Approach To Abdominal PainDocument22 pagesApproach To Abdominal PainOmar AbdillahiNo ratings yet
- Acute AbdomenDocument2 pagesAcute AbdomenTroy FengNo ratings yet
- Acute Abdominal Pain GuideDocument19 pagesAcute Abdominal Pain GuideAudricNo ratings yet
- AN APPROACH TO PAEDIATRIC ABDOMINAL PAINDocument32 pagesAN APPROACH TO PAEDIATRIC ABDOMINAL PAINdrsaleemNo ratings yet
- Abdominal Pain in Pregnancy: A Rational Approach To ManagementDocument10 pagesAbdominal Pain in Pregnancy: A Rational Approach To ManagementElena ZepedaNo ratings yet
- ExamPreview RN 111722Document148 pagesExamPreview RN 111722jhajj0% (3)
- Abdominal Visceral Pain: Clinical AspectDocument4 pagesAbdominal Visceral Pain: Clinical AspectMagdy GabrNo ratings yet
- Full Download Medical Surgical Nursing Critical Thinking For Collaborative Care PDF Full ChapterDocument36 pagesFull Download Medical Surgical Nursing Critical Thinking For Collaborative Care PDF Full Chapterjasonjohnsonfzcjibytag100% (15)
- A Colour Handbook of GastroenterologyDocument248 pagesA Colour Handbook of GastroenterologyAlina Gabriela FetoiuNo ratings yet
- Stomachache and Abdominal PainDocument3 pagesStomachache and Abdominal PainHarold Sgo Jimenez GNo ratings yet
- Lec04 - Assessing Mouth, Throat, Abdomen and RectumDocument23 pagesLec04 - Assessing Mouth, Throat, Abdomen and RectumIRISH MANIAGONo ratings yet
- Symptoms and Causes of ColitisDocument5 pagesSymptoms and Causes of ColitisChatrina TandiloloNo ratings yet
- General Surgery Board-Final Written Exam Blueprint v.1Document3 pagesGeneral Surgery Board-Final Written Exam Blueprint v.1Mohammed S. Al GhamdiNo ratings yet
- CHAPTER 12 Abdominal PainDocument2 pagesCHAPTER 12 Abdominal PainIvanka Lizbeth PrieteNo ratings yet
- Dif&dia&ped&gup&5 THDocument619 pagesDif&dia&ped&gup&5 THGokul Adarsh100% (1)