You might also like
- ACBT and Autogenic Drainage PDFDocument14 pagesACBT and Autogenic Drainage PDFSwati GuptaNo ratings yet
- Airway Clearance Therapy: Finding The Evidence: Teresa A Volsko MHHS RRT FAARCDocument10 pagesAirway Clearance Therapy: Finding The Evidence: Teresa A Volsko MHHS RRT FAARCRodolfo MoyaNo ratings yet
- Endotracheal Suctioning of Mechanically Ventilated Patients With Artificial Airways (June 2010)Document7 pagesEndotracheal Suctioning of Mechanically Ventilated Patients With Artificial Airways (June 2010)DCaeiroNo ratings yet
- Fonc 11 751396Document10 pagesFonc 11 751396Muhammad RifkiNo ratings yet
- Airway Clearance TechniquesDocument14 pagesAirway Clearance TechniquesKhushboo DurejaNo ratings yet
- When To Remove A Chest TubeDocument6 pagesWhen To Remove A Chest TubeAlan Espíndola CruzNo ratings yet
- Apical Vapor LockDocument21 pagesApical Vapor Locktito reddyNo ratings yet
- Decanulasi TrakeostomiDocument6 pagesDecanulasi TrakeostomiDhiel Muhammad FarreyraNo ratings yet
- Advances in Chest Drain Management in Thoracic DiseaseDocument10 pagesAdvances in Chest Drain Management in Thoracic DiseasetomeyttoNo ratings yet
- Jet VentilationDocument5 pagesJet Ventilationskumar bNo ratings yet
- Management of The Artificial AirwaDocument17 pagesManagement of The Artificial AirwaGuillermoAlphonsoVasquezGiglioNo ratings yet
- Nseir 2011Document11 pagesNseir 2011Dayana PalacioNo ratings yet
- EpiphoraDocument13 pagesEpiphoramanognaaaaNo ratings yet
- HidroceleDocument5 pagesHidrocelelochnezNo ratings yet
- Indications of JP DrainsDocument9 pagesIndications of JP DrainsDelbrynth MitchaoNo ratings yet
- Anesthesia For BronchosDocument11 pagesAnesthesia For Bronchosadink mochammadNo ratings yet
- Advanced Trauma and Life Support AtlsDocument64 pagesAdvanced Trauma and Life Support AtlsAnggita Tri YurisworoNo ratings yet
- LM 3 - Chest TubeDocument5 pagesLM 3 - Chest TubeMelrhean GraceNo ratings yet
- 1 s2.0 S0196070922003945 MainDocument8 pages1 s2.0 S0196070922003945 MainJose Miguel CastellonNo ratings yet
- 5309 Ra 1Document3 pages5309 Ra 176q88b4yrxNo ratings yet
- Airway Management and CO2 Laser Treatment of Subglottic and Tracheal Stenosis Using Flexible Bronchoscope and Laryngeal Mask Anesthesia, 2011Document4 pagesAirway Management and CO2 Laser Treatment of Subglottic and Tracheal Stenosis Using Flexible Bronchoscope and Laryngeal Mask Anesthesia, 2011Araceli BarreraNo ratings yet
- Wound Drain PlacementDocument7 pagesWound Drain PlacementVictor BeranNo ratings yet
- Critical Care SuctioningDocument5 pagesCritical Care SuctioningChinta Nabila 조롱 수없는No ratings yet
- Ett OkDocument8 pagesEtt OkOman HendiNo ratings yet
- Closed Vs Open SuctionDocument5 pagesClosed Vs Open SuctionKhushboo DurejaNo ratings yet
- Improvement After Surgical Closure of Secundum Atrial Septal Defects in Adults 2155 9880 1000493Document9 pagesImprovement After Surgical Closure of Secundum Atrial Septal Defects in Adults 2155 9880 1000493Riani NazilaNo ratings yet
- Surgical Management of Parapharyngeal AbscessDocument3 pagesSurgical Management of Parapharyngeal AbscessmeyNo ratings yet
- Alr22476 RevDocument13 pagesAlr22476 Revplz sub me whant moniNo ratings yet
- What's New in Reducing The Impact of Tracheostomy On Communication and Swallowing in The ICUDocument4 pagesWhat's New in Reducing The Impact of Tracheostomy On Communication and Swallowing in The ICUMarisol BecerraNo ratings yet
- Sdfa Sdfasdk JFLKSDF Asdfasdf Sdaf AsdfDocument19 pagesSdfa Sdfasdk JFLKSDF Asdfasdf Sdaf AsdfFaris BariqiNo ratings yet
- MikroaspirasiDocument6 pagesMikroaspirasiPamungkas HaryNo ratings yet
- Chest Drainage Medical ManagementDocument3 pagesChest Drainage Medical ManagementPaul John RutaquioNo ratings yet
- The Influence of Airflow Via High Flow Nasal Cannula On DurationDocument7 pagesThe Influence of Airflow Via High Flow Nasal Cannula On DurationMariana BarrosNo ratings yet
- Pompili 2017Document4 pagesPompili 2017Teja LaksanaNo ratings yet
- Jurnal MataDocument5 pagesJurnal MataArifah UsrahNo ratings yet
- Op900. Tracheostomy, ConiotomyDocument4 pagesOp900. Tracheostomy, ConiotomyGus LionsNo ratings yet
- 1 PBDocument4 pages1 PBrashmiNo ratings yet
- Care of Chest Drainage: Articles RationaleDocument7 pagesCare of Chest Drainage: Articles Rationalepreeti sharmaNo ratings yet
- Management Options of Acquired Punctal Stenosis: Review ArticleDocument8 pagesManagement Options of Acquired Punctal Stenosis: Review ArticleAhmed samyNo ratings yet
- Bladder Explosion During Transurethral Resection Surgery Case SeriesDocument21 pagesBladder Explosion During Transurethral Resection Surgery Case SeriesAthenaeum Scientific PublishersNo ratings yet
- Management of AirwaysDocument12 pagesManagement of AirwaysdyahNo ratings yet
- Airway Management During Upper GI Endoscopic Procedures2016Document9 pagesAirway Management During Upper GI Endoscopic Procedures2016jcarl_20063003No ratings yet
- Managing A Chest Tube and Drainage System: Rajaraman Durai, Happy Hoque, Tony W. DaviesDocument9 pagesManaging A Chest Tube and Drainage System: Rajaraman Durai, Happy Hoque, Tony W. DaviesBeni BolngNo ratings yet
- Endotracheal Tubes and Fluid Aspiration An in Vitro Evaluation of New Cuff TechnologiesDocument9 pagesEndotracheal Tubes and Fluid Aspiration An in Vitro Evaluation of New Cuff TechnologiesTintin TagupaNo ratings yet
- Rocco 2017Document6 pagesRocco 2017Ricardo Uzcategui ArreguiNo ratings yet
- Perbedaan Close Suction Dan Open SuctionDocument13 pagesPerbedaan Close Suction Dan Open Suctionriri fitrisariNo ratings yet
- 241 TracheostomyDocument12 pages241 Tracheostomyalbert hutagalungNo ratings yet
- Evidence-Based Management of Patients With Chest Tube Drainage System To Reduce Complications in Cardiothoracic Vascular Surgery WardsDocument8 pagesEvidence-Based Management of Patients With Chest Tube Drainage System To Reduce Complications in Cardiothoracic Vascular Surgery WardsJumia AndawaNo ratings yet
- Plasma Extraction by Centrifugo-PneumatiDocument6 pagesPlasma Extraction by Centrifugo-PneumatihanieNo ratings yet
- Pulmonary: Treatment ofDocument5 pagesPulmonary: Treatment ofYantoNo ratings yet
- Principles and Practice of Lacrimal SurgeryFrom EverandPrinciples and Practice of Lacrimal SurgeryMohammad Javed AliNo ratings yet
- Dbouk, Talib & Drikakis, Dimitris - On Respiratory Droplets and Face Masks (2020) - Physics of Fluids 32, 063303 - 5.0015044Document12 pagesDbouk, Talib & Drikakis, Dimitris - On Respiratory Droplets and Face Masks (2020) - Physics of Fluids 32, 063303 - 5.0015044cbtext1sNo ratings yet
- LaparoscopeDocument9 pagesLaparoscopedharmaNo ratings yet
- 1 s2.0 S0007091217425281 MainDocument5 pages1 s2.0 S0007091217425281 Mainmanolo.mendozavNo ratings yet
- Surgic Al Ma Na Gement Oftheseptal Per Forat Ion: Deborah Watson,, Gregory BarkdullDocument11 pagesSurgic Al Ma Na Gement Oftheseptal Per Forat Ion: Deborah Watson,, Gregory BarkdullVinoth LakshmikanthNo ratings yet
- Surgical Vacuum DrainDocument9 pagesSurgical Vacuum DrainZulfadli Salleh100% (1)
- Clinical Evaluation Swallowing Disorders As A Predictor of Unsuccessful Extubation: ADocument8 pagesClinical Evaluation Swallowing Disorders As A Predictor of Unsuccessful Extubation: ARodrigo Navia ValenzuelaNo ratings yet
- TOPIC 10 - 1019031146 UbaidillahDocument8 pagesTOPIC 10 - 1019031146 UbaidillahUbay SegaNo ratings yet
- Recombiplastin 2G - 0020002950 (8 ML) : Al For Identification and Resolution of Out-Of-Control SituationsDocument5 pagesRecombiplastin 2G - 0020002950 (8 ML) : Al For Identification and Resolution of Out-Of-Control SituationsSteffyPérezPioNo ratings yet
- ATLAS OF INTERVENTIONAL PAIN MANAGEMENT, 4ed PDFDocument1,164 pagesATLAS OF INTERVENTIONAL PAIN MANAGEMENT, 4ed PDFjesussalvadorsuazaNo ratings yet
- Chapter 7 - Dimension of Development - First Aid EducationDocument10 pagesChapter 7 - Dimension of Development - First Aid EducationAsh MooreNo ratings yet
- Hubungan Pengetahuan Dan Sikap Dengan Peran Perawat Pasca Pemberian Terapi RtpaDocument6 pagesHubungan Pengetahuan Dan Sikap Dengan Peran Perawat Pasca Pemberian Terapi RtpafatmawatiNo ratings yet
- Catatan Pediatri Raphaela-20190613122003Document68 pagesCatatan Pediatri Raphaela-20190613122003Kevin Kusuman100% (1)
- Nonextraction Treatment With Begg TechniqueDocument14 pagesNonextraction Treatment With Begg TechniqueSyed Mohammad Osama AhsanNo ratings yet
- Brazil Anvisa RDC 37 2015 Labeling Rubber Latex enDocument1 pageBrazil Anvisa RDC 37 2015 Labeling Rubber Latex enElaine NascimentoNo ratings yet
- Physical Stability and Activity of Cream W/O Etanolik Fruit EXTRACT MAHKOTA DEWA (Phaleria Macrocarph (Scheff.) Boerl,) AS A SunscreenDocument9 pagesPhysical Stability and Activity of Cream W/O Etanolik Fruit EXTRACT MAHKOTA DEWA (Phaleria Macrocarph (Scheff.) Boerl,) AS A SunscreenNur RohmahNo ratings yet
- Covid 19 PCR Test Results - JTH LAB - 2021.10.28 - For THJaffnaDocument2 pagesCovid 19 PCR Test Results - JTH LAB - 2021.10.28 - For THJaffnaArshathNo ratings yet
- Npi-Family Case StudyDocument12 pagesNpi-Family Case StudyGayLah MomblancoNo ratings yet
- Hiro System Procedure PDFDocument8 pagesHiro System Procedure PDFsnehaNo ratings yet
- Rekap Kalibrasi - Rumah Sakit Umum Daerah JombangDocument30 pagesRekap Kalibrasi - Rumah Sakit Umum Daerah JombangSeliyuli AntinaNo ratings yet
- ShopeepayDocument18 pagesShopeepayelvina utamaNo ratings yet
- HybaseDocument6 pagesHybaseSreejith SwaminathanNo ratings yet
- List of Nursing OrganizationsDocument3 pagesList of Nursing OrganizationsShehada Marcos BondadNo ratings yet
- Vikram Covid Vaccine Certificate1666801329239Document1 pageVikram Covid Vaccine Certificate1666801329239DR nagar gamerNo ratings yet
- Dentist FormDocument2 pagesDentist FormkianmiguelNo ratings yet
- Updated PPT Surgical Hand WashingDocument13 pagesUpdated PPT Surgical Hand WashingInsatiable CleeNo ratings yet
- Template Form EEA Evidence of Internship DC0017 PDF 3798454Document2 pagesTemplate Form EEA Evidence of Internship DC0017 PDF 3798454Anonymous YqCxXQ6wF5No ratings yet
- Webster 2019Document13 pagesWebster 2019sebakinesico-1No ratings yet
- Rekapan Diah Ayu-UHAMKA-DM Tipe 2Document185 pagesRekapan Diah Ayu-UHAMKA-DM Tipe 2DevinaNo ratings yet
- Praktek DR Juwanto SP PD Pekanbaru - Google Search PDFDocument1 pagePraktek DR Juwanto SP PD Pekanbaru - Google Search PDFayu nanizaNo ratings yet
- 10 OBAT TERBANYAK YANG DIGUNAKAN November 21Document5 pages10 OBAT TERBANYAK YANG DIGUNAKAN November 21MutemjNo ratings yet
- Functionality of Barangay Anti-Drug Abuse Council: Its Roles and Responsibilities Under Dilg Memorandum Circular No. 2015-66Document21 pagesFunctionality of Barangay Anti-Drug Abuse Council: Its Roles and Responsibilities Under Dilg Memorandum Circular No. 2015-66Angelie Regie J EstorqueNo ratings yet
- HP Commonwealth (Bartolome, Kendrick)Document1 pageHP Commonwealth (Bartolome, Kendrick)maryjoyloma04No ratings yet
- Pharma Company in EgyptDocument2 pagesPharma Company in EgyptMohamed Elsayed Farouk MostafaNo ratings yet
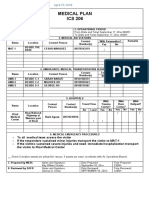
- Ics 206Document1 pageIcs 206Ldrrmo RamonNo ratings yet
- History of HospitalsDocument20 pagesHistory of HospitalsanushakanchiNo ratings yet
- African CultureDocument10 pagesAfrican CultureChelsy Allaine Dela CruzNo ratings yet