You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Types of Volcanoes - ShapeDocument2 pagesTypes of Volcanoes - ShapejeffersonNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Haal E Safar Az Farsh Ta Arsh or Read OnlineDocument174 pagesHaal E Safar Az Farsh Ta Arsh or Read OnlineHaal e Safar100% (4)
- Power of Love-Huey Lewis CRDDocument2 pagesPower of Love-Huey Lewis CRDmoon_19690% (1)
- History of Madre de DiosDocument3 pagesHistory of Madre de DiosMisterJanNo ratings yet
- Incidence of Alveoloplasty PDFDocument4 pagesIncidence of Alveoloplasty PDFaleeza sanaNo ratings yet
- Arts - 9 - Quarter 3 Module 1Document4 pagesArts - 9 - Quarter 3 Module 1John Mark Prestoza100% (3)
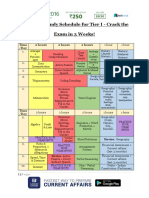
- SSC CHSL Study Schedule For Tier I - Crack The Exam in 3 Weeks!Document3 pagesSSC CHSL Study Schedule For Tier I - Crack The Exam in 3 Weeks!Tushita80% (15)
- Color Symbolism and CultureDocument7 pagesColor Symbolism and CultureWAQAS SHARIFNo ratings yet
- Islamiyat O-Level Paper-1 Notes PDFDocument126 pagesIslamiyat O-Level Paper-1 Notes PDFddd80% (5)
- Molecular Mechanisms of Synergistic Induction of Apoptosis by The Combination Therapy With Hyperthermia and Cisplatin in Prostate Cancer CellsDocument19 pagesMolecular Mechanisms of Synergistic Induction of Apoptosis by The Combination Therapy With Hyperthermia and Cisplatin in Prostate Cancer Cellsnam 11No ratings yet
- Autophagy-Active Beclin-1 Correlates With Favourable Clinical Outcome in Non-Hodgkin LymphomasDocument14 pagesAutophagy-Active Beclin-1 Correlates With Favourable Clinical Outcome in Non-Hodgkin Lymphomasnam 11No ratings yet
- Cell Cycle Responses To HyperthermiaDocument15 pagesCell Cycle Responses To Hyperthermianam 11No ratings yet
- Correlation Between Cell Killing Effect and Cell Membrane Potential After Heat Treatment Analysis Using Fluorescent Dye and Flow CytometryDocument9 pagesCorrelation Between Cell Killing Effect and Cell Membrane Potential After Heat Treatment Analysis Using Fluorescent Dye and Flow Cytometrynam 11No ratings yet
- Cancer Treatment With HyperthermiaDocument21 pagesCancer Treatment With Hyperthermianam 11No ratings yet
- Short 428C Heat Shock Induces Phosphorylation and Degradation of Cdc25A Which Depends On p38MAPK, Chk2 and 14 3 3Document11 pagesShort 428C Heat Shock Induces Phosphorylation and Degradation of Cdc25A Which Depends On p38MAPK, Chk2 and 14 3 3nam 11No ratings yet
- Parkin, PINK1, and DJ-1 Form A Ubiquitin E3 Ligase Complex Promoting Unfolded Protein DegradationDocument12 pagesParkin, PINK1, and DJ-1 Form A Ubiquitin E3 Ligase Complex Promoting Unfolded Protein Degradationnam 11No ratings yet
- Task Performance EuthenicsDocument3 pagesTask Performance EuthenicsKimberly MarquezNo ratings yet
- Genmath Q2 Week4Document36 pagesGenmath Q2 Week4ShennieNo ratings yet
- Lguvisitation-Municipality of CaintaDocument23 pagesLguvisitation-Municipality of CaintaDaniel BulanNo ratings yet
- An Introduction To Uhde Oil & Gas: Thyssenkrupp Uhde - Engineering With IdeasDocument40 pagesAn Introduction To Uhde Oil & Gas: Thyssenkrupp Uhde - Engineering With IdeasHany FathyNo ratings yet
- Gehman Mennonite Church: Let's Walk With Jesus Personally, Locally, and GloballyDocument1 pageGehman Mennonite Church: Let's Walk With Jesus Personally, Locally, and GloballyGehman Mennonite ChurchNo ratings yet
- Capto: 3 Good Reasons To Use The Capto For Handling Heavy FabricsDocument2 pagesCapto: 3 Good Reasons To Use The Capto For Handling Heavy FabricsgustirizkiawanNo ratings yet
- Catalogue2019 PDFDocument12 pagesCatalogue2019 PDFlakavath arthiNo ratings yet
- CW-80 ManualDocument12 pagesCW-80 ManualBrian YostNo ratings yet
- Cape Police Report - Unattended BodyDocument2 pagesCape Police Report - Unattended BodyNews-PressNo ratings yet
- FRC Team 2637, Phatnom Catz, Techbinder 2023 - 2024 CrescendoDocument17 pagesFRC Team 2637, Phatnom Catz, Techbinder 2023 - 2024 CrescendoShrey Agarwal (Drago Gaming)No ratings yet
- Wimod Ic iC880A: DatasheetDocument26 pagesWimod Ic iC880A: DatasheetJulian CamiloNo ratings yet
- Magic Porridge Pot-story+BilderDocument4 pagesMagic Porridge Pot-story+BilderSylvester PhilipNo ratings yet
- GoKReport1819Final 23091uDocument28 pagesGoKReport1819Final 23091uGurukrupa DasNo ratings yet
- Pengembangan Transferable Skills Dalam PembelajaraDocument12 pagesPengembangan Transferable Skills Dalam PembelajaraKesat RiyanNo ratings yet
- Business Communication - IIDocument3 pagesBusiness Communication - IIprachi100% (1)
- Identify The Choice That Best Completes The Statement or Answers The QuestionDocument9 pagesIdentify The Choice That Best Completes The Statement or Answers The QuestionDaniella mae ElipNo ratings yet
- Chapter 1 and 2Document75 pagesChapter 1 and 2Balamurali SureshNo ratings yet
- Workplace Health Promotion at Eska Rafinerska (Oil Refinery) 1. Organisations Involved 2. Description of The CaseDocument2 pagesWorkplace Health Promotion at Eska Rafinerska (Oil Refinery) 1. Organisations Involved 2. Description of The CaseDiana Vanessa GuerreroNo ratings yet
- Candi MerakDocument2 pagesCandi MerakEdi YantoNo ratings yet
- Jeselo O. Gorme, RN, MNDocument109 pagesJeselo O. Gorme, RN, MNcoosa liquorsNo ratings yet
- Askehave and Nielsen - Digital Genres PDFDocument22 pagesAskehave and Nielsen - Digital Genres PDFChristopher SmithNo ratings yet