You might also like
- Leaky Gut Syndrome for Beginners - The Self-Help Book - How to Correctly Interpret the Symptoms of a Leaky Gut, Identify the Causes and Heal Your Gut Step by StepFrom EverandLeaky Gut Syndrome for Beginners - The Self-Help Book - How to Correctly Interpret the Symptoms of a Leaky Gut, Identify the Causes and Heal Your Gut Step by StepNo ratings yet
- By: Abduljabbar Hamid Jabbar: University of Baghdad-College of Medicine M. B. Ch. BDocument14 pagesBy: Abduljabbar Hamid Jabbar: University of Baghdad-College of Medicine M. B. Ch. BXena XenaNo ratings yet
- Anatomy and Physiology of the Stomach and DuodenumDocument47 pagesAnatomy and Physiology of the Stomach and DuodenumMahmood SalahNo ratings yet
- Digestion Is The Breaking Down of Chemicals in The Body, Into A Form That Can Be Absorbed. It IsDocument10 pagesDigestion Is The Breaking Down of Chemicals in The Body, Into A Form That Can Be Absorbed. It IsSean McleanNo ratings yet
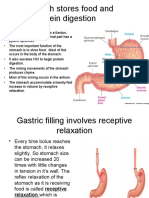
- Gastric/Stomach Physiology: 1. Gastric Filling Involves Receptive RelaxationDocument8 pagesGastric/Stomach Physiology: 1. Gastric Filling Involves Receptive RelaxationAnton KerenzNo ratings yet
- Git Lec 3,4Document14 pagesGit Lec 3,4Kim Sa-buNo ratings yet
- 13 Human Physiology Gastrointestinal PhysiologyDocument82 pages13 Human Physiology Gastrointestinal PhysiologysuNo ratings yet
- The Digestive System A Level NotesDocument7 pagesThe Digestive System A Level Noteselendria100% (1)
- Lecture 10: Gastric Secretion & Its Regulation: Functions of StomachDocument8 pagesLecture 10: Gastric Secretion & Its Regulation: Functions of StomachBoody KhalilNo ratings yet
- GIT Chapter ReviewDocument11 pagesGIT Chapter ReviewPersonne AnonymeNo ratings yet
- Digestive System - 2: Learning ObjectivesDocument5 pagesDigestive System - 2: Learning ObjectivesMaggieLockeNo ratings yet
- Gastric Secretions MineDocument27 pagesGastric Secretions MinesasamaterasuNo ratings yet
- PSG 252 Lecture 3 The StomachDocument5 pagesPSG 252 Lecture 3 The StomachMichael TobilobaNo ratings yet
- Fom 4.1Document8 pagesFom 4.1yelloweverglowNo ratings yet
- Case Presentation (NCM 102)Document26 pagesCase Presentation (NCM 102)Ibs LimNo ratings yet
- Large Intestine.: © L N - A & P II (A. I) D P1 8Document8 pagesLarge Intestine.: © L N - A & P II (A. I) D P1 8Naveen EldoseNo ratings yet
- Digestive/Endocrine Answer KeyDocument10 pagesDigestive/Endocrine Answer KeykmulqsNo ratings yet
- GIT Lect A2Document43 pagesGIT Lect A2Ayurveda PgNo ratings yet
- Digestive System (Unit X)Document44 pagesDigestive System (Unit X)zahraNo ratings yet
- Nur Syahirah Binti Mohd Yusri A170291: Nama Dan No. MatrikDocument9 pagesNur Syahirah Binti Mohd Yusri A170291: Nama Dan No. MatrikSyahirah YusriNo ratings yet
- Physiology: Bile Secretion by The LiverDocument8 pagesPhysiology: Bile Secretion by The Liverزين العابدين محمد عويشNo ratings yet
- Biopharmaceutics-01 AssignmentDocument14 pagesBiopharmaceutics-01 AssignmentRA TanvirNo ratings yet
- Physiology of GIT NursingDocument87 pagesPhysiology of GIT NursingraphatoelNo ratings yet
- The Digestion ProcessDocument7 pagesThe Digestion ProcessKim Szydney RachoNo ratings yet
- Mechanism of Gastric SecretionDocument11 pagesMechanism of Gastric Secretionmulya ningsihNo ratings yet
- All About GIT PhysiologyDocument79 pagesAll About GIT PhysiologyHarshavardhan AmancherlaNo ratings yet
- PencernaanDocument39 pagesPencernaanVina Zavira NizarNo ratings yet
- The Anatomy of The StomachDocument33 pagesThe Anatomy of The StomachVictor OmoloNo ratings yet
- Digestive System Chapter 23 Practice ExamDocument5 pagesDigestive System Chapter 23 Practice Examkimber brownNo ratings yet
- CBI503 Digestive System Physiology GuideDocument7 pagesCBI503 Digestive System Physiology GuideMaggieLockeNo ratings yet
- Digestive SystemDocument12 pagesDigestive Systemapi-269652707No ratings yet
- Research On Digestion in The StomachDocument3 pagesResearch On Digestion in The StomachNaomi NwaniNo ratings yet
- Anatomy and Physiology of The StomachDocument7 pagesAnatomy and Physiology of The StomachEmmi Maliza HutagaolNo ratings yet
- Stomach: Curvature. The Convex Lateral Border Is Called The Greater CurvatureDocument4 pagesStomach: Curvature. The Convex Lateral Border Is Called The Greater CurvaturezuzuzazaziziNo ratings yet
- Anatomy and Physiology of the Gastrointestinal SystemDocument117 pagesAnatomy and Physiology of the Gastrointestinal SystemKBDNo ratings yet
- Gastric SecretionDocument36 pagesGastric SecretionammuNo ratings yet
- Nutrition and DigestionDocument8 pagesNutrition and DigestionjeffchegzodNo ratings yet
- Git Lec 3Document33 pagesGit Lec 3Kim Sa-buNo ratings yet
- Anatomy and Physiology of the Gastrointestinal System - Functions, Organs and Digestion ProcessDocument117 pagesAnatomy and Physiology of the Gastrointestinal System - Functions, Organs and Digestion ProcessJohnMichaelDominguezNo ratings yet
- Anatomy and Physiology of Human Digestive System: The Mouth and PharynxDocument9 pagesAnatomy and Physiology of Human Digestive System: The Mouth and Pharynxitachi278No ratings yet
- Digestive System 2022-23Document28 pagesDigestive System 2022-23Fady Fady100% (1)
- 1 IntroductionDocument22 pages1 IntroductionirfanNo ratings yet
- M1 Lesson 2Document6 pagesM1 Lesson 2Catherine Sinen ObinqueNo ratings yet
- Digestive System and Bioenergetics NotesDocument9 pagesDigestive System and Bioenergetics NotesDestinee LegendsNo ratings yet
- ANATOMY & PHY OF THE GIDocument8 pagesANATOMY & PHY OF THE GIElsy MayjoNo ratings yet
- Pig Digestive System-Digestive System of The PigDocument4 pagesPig Digestive System-Digestive System of The PiglsvcsbNo ratings yet
- Stomach and Small IntestenDocument49 pagesStomach and Small IntestenNyakie MotlalaneNo ratings yet
- 4-The Digestive System PDocument29 pages4-The Digestive System PferasshaaNo ratings yet
- Stomach Anatomy, Functions and SecretionsDocument29 pagesStomach Anatomy, Functions and SecretionsSaad Zafar AwanNo ratings yet
- Digestive System ReviewDocument2 pagesDigestive System ReviewSherriena LeangNo ratings yet
- Physiology, Lecture 8, GIT 2 (Stomach) (Slides)Document24 pagesPhysiology, Lecture 8, GIT 2 (Stomach) (Slides)Ali Al-Qudsi100% (2)
- Alimentary TractDocument122 pagesAlimentary TractMosa MosaNo ratings yet
- THE DIGESTIVE SYSTEM EXPLAINEDDocument44 pagesTHE DIGESTIVE SYSTEM EXPLAINEDJoy NatividadNo ratings yet
- Digestive Physiology ExplainedDocument14 pagesDigestive Physiology ExplainedJãçk SparrowNo ratings yet
- H92C 35 Self Assessment Digestion AnswersDocument4 pagesH92C 35 Self Assessment Digestion AnswersdoaaNo ratings yet
- Digestive System A&p BookletDocument11 pagesDigestive System A&p Bookletnurse1990No ratings yet
- Physio. D. NOOR. L4.GITDocument8 pagesPhysio. D. NOOR. L4.GITزين العابدين محمد عويشNo ratings yet
- Digestive System Deglutition PhasesDocument9 pagesDigestive System Deglutition PhasesLekhana BankiNo ratings yet
- Gross Anatomy: RugaeDocument5 pagesGross Anatomy: RugaeKryza Dale Bunado BaticanNo ratings yet
- Digestive System Finalppt LectureDocument30 pagesDigestive System Finalppt LectureFrancene YepesNo ratings yet
- By: Abduljabbar Hamid Jabbar: University of Baghdad-College of Medicine M. B. Ch. BDocument97 pagesBy: Abduljabbar Hamid Jabbar: University of Baghdad-College of Medicine M. B. Ch. BXena XenaNo ratings yet
- Understanding the Stages of Swallowing (DeglutitionDocument16 pagesUnderstanding the Stages of Swallowing (DeglutitionXena XenaNo ratings yet
- Physio 6. Digestive System 6Document21 pagesPhysio 6. Digestive System 6Xena XenaNo ratings yet
- Understanding the Stages of Swallowing (DeglutitionDocument16 pagesUnderstanding the Stages of Swallowing (DeglutitionXena XenaNo ratings yet
- By: Abduljabbar Hamid Jabbar: University of Baghdad-College of Medicine M. B. Ch. BDocument97 pagesBy: Abduljabbar Hamid Jabbar: University of Baghdad-College of Medicine M. B. Ch. BXena XenaNo ratings yet
- Hypersensitivity Reaction TypesDocument1 pageHypersensitivity Reaction TypesTom MallinsonNo ratings yet
- 11 Marker-Assisted Selection in Plant BreedingDocument22 pages11 Marker-Assisted Selection in Plant BreedingrosanaNo ratings yet
- NCPDocument3 pagesNCPErl DrizNo ratings yet
- Scleroderma PathophysiologyDocument3 pagesScleroderma PathophysiologyampalNo ratings yet
- MCQS-Ch-5-Variety of Life-Part-Sol-1Document2 pagesMCQS-Ch-5-Variety of Life-Part-Sol-1All kinds of information on channelNo ratings yet
- Antibacterial Activity of Aqueous Extract of CalotDocument5 pagesAntibacterial Activity of Aqueous Extract of CalotVishnu PriyaNo ratings yet
- BIOINFORMATICS LAB ReportDocument14 pagesBIOINFORMATICS LAB ReportKaleemUllah SulimankhailNo ratings yet
- Biology GWD Projects 2022Document2 pagesBiology GWD Projects 2022LizzyNo ratings yet
- TTH Edition 2nd EditionDocument62 pagesTTH Edition 2nd EditionfrankcubeNo ratings yet
- Bioplastic A Bettter Alternative For Sustanable FutureDocument72 pagesBioplastic A Bettter Alternative For Sustanable FutureShanaiah Charice GanasNo ratings yet
- Periodontology 2000 - 2021 - Hajishengallis - Polymicrobial Communities in Periodontal Disease Their Quasi OrganismalDocument21 pagesPeriodontology 2000 - 2021 - Hajishengallis - Polymicrobial Communities in Periodontal Disease Their Quasi Organismalalan.da.s.aguirreNo ratings yet
- June 2016 (v3) QP - Paper 2 CIE Biology A-LevelDocument12 pagesJune 2016 (v3) QP - Paper 2 CIE Biology A-LevelSalman Farsi TaharatNo ratings yet
- MLS214 Merged Files-Final LabDocument66 pagesMLS214 Merged Files-Final LabGhada BucheeriNo ratings yet
- CSF SamplesDocument14 pagesCSF SamplesEPHANTUS WAINAINANo ratings yet
- 2017 Residancy Exam JUHDocument8 pages2017 Residancy Exam JUHMohammadSAL-RawashdehNo ratings yet
- R. L. M. Pierik (Auth.) - in Vitro Culture of Higher Plants-Springer Netherlands (1987) PDFDocument345 pagesR. L. M. Pierik (Auth.) - in Vitro Culture of Higher Plants-Springer Netherlands (1987) PDFPablo GutierrezNo ratings yet
- Glorious PR FinalDocument188 pagesGlorious PR FinalJulie Silvenia100% (1)
- Molecular Characterization and Antibiotic Resistance of Staphylococcus Spp. Isolated From Cheese Processing PlantsDocument9 pagesMolecular Characterization and Antibiotic Resistance of Staphylococcus Spp. Isolated From Cheese Processing PlantsAbdul Wahab Assya RoniNo ratings yet
- Pathology of Female Reproductive SystemDocument33 pagesPathology of Female Reproductive SystemDio Reynaldi SusantoNo ratings yet
- Focus On Myeloproliferative Diseases and Myelodysplastic SyndromesDocument6 pagesFocus On Myeloproliferative Diseases and Myelodysplastic SyndromesBopiyudha bopiyudhaNo ratings yet
- Cell Organelles Worksheet: Structure/Function Cell PartDocument2 pagesCell Organelles Worksheet: Structure/Function Cell PartKimora BrooksNo ratings yet
- Gene LibrariesDocument14 pagesGene Librariessharmamaddy32No ratings yet
- PLANT PATHOLOGY OBJECTIVE QUESTIONSDocument65 pagesPLANT PATHOLOGY OBJECTIVE QUESTIONSJIBIN JOSE100% (1)
- Structure of HemoglobinDocument3 pagesStructure of HemoglobinAyesha SheikhNo ratings yet
- Ebola Health Education CHNDocument23 pagesEbola Health Education CHNBrijesh YadavNo ratings yet
- Microbiology ExperimentDocument9 pagesMicrobiology Experiment门门No ratings yet
- Microbiology PDFDocument146 pagesMicrobiology PDFsadaf javeriaNo ratings yet
- Neuro CH 14 Study GuideDocument9 pagesNeuro CH 14 Study GuideMichael J MillerNo ratings yet
- Channel Catfish Virus DiseaseDocument4 pagesChannel Catfish Virus Diseaseapi-3737467No ratings yet
- Science8 Q4 M3Document16 pagesScience8 Q4 M3Vine100% (1)