You might also like
- Perio-Prosthodontic Pontic Site Management, Part I: Pontic Designs and Their Current ApplicationsDocument12 pagesPerio-Prosthodontic Pontic Site Management, Part I: Pontic Designs and Their Current ApplicationsFelipe Castro100% (4)
- 06 Silverman 1953 The Speaking Method in Measuring Vertical DimensionDocument7 pages06 Silverman 1953 The Speaking Method in Measuring Vertical DimensionCoRal Partida BenitezNo ratings yet
- Horizontal Alveolar Ridge Augmentation in Implant Dentistry: A Surgical ManualFrom EverandHorizontal Alveolar Ridge Augmentation in Implant Dentistry: A Surgical ManualRating: 4.5 out of 5 stars4.5/5 (2)
- A Restrospective Periodontal Assessment of 137 Teeth After Featheredge Preparation and GingittageDocument11 pagesA Restrospective Periodontal Assessment of 137 Teeth After Featheredge Preparation and GingittageBelen AntoniaNo ratings yet
- A Review of Esthetic Pontic Design OptionsDocument12 pagesA Review of Esthetic Pontic Design OptionsCristhiane Rodrigues MaryNo ratings yet
- Let S Be Your Guide-PoundDocument8 pagesLet S Be Your Guide-PoundFaheemuddin MuhammadNo ratings yet
- Fixed Orthodontic Appliances: A Practical GuideFrom EverandFixed Orthodontic Appliances: A Practical GuideRating: 1 out of 5 stars1/5 (1)
- What Is The Evidence Base For The Efficacies of Different Complete Denture Impression Procedures? A Critical ReviewDocument16 pagesWhat Is The Evidence Base For The Efficacies of Different Complete Denture Impression Procedures? A Critical ReviewVishal ReddyNo ratings yet
- Digital Planning and Custom Orthodontic TreatmentFrom EverandDigital Planning and Custom Orthodontic TreatmentK. Hero BreuningNo ratings yet
- Implant Thread Designs: An Overview: July 2017Document10 pagesImplant Thread Designs: An Overview: July 2017Seno FauziNo ratings yet
- Understanding Masticatory Function in Unilateral CrossbitesFrom EverandUnderstanding Masticatory Function in Unilateral CrossbitesNo ratings yet
- A New Veneer Technique With Prefabricated Composite Denture Teeth Combined With The "Biologically Oriented Preparation Technique" (BOPT) - A Case Report PDFDocument14 pagesA New Veneer Technique With Prefabricated Composite Denture Teeth Combined With The "Biologically Oriented Preparation Technique" (BOPT) - A Case Report PDFLinda Garcia PNo ratings yet
- Anterior Teeth and Smile Design FactorsDocument11 pagesAnterior Teeth and Smile Design FactorsSahana Rangarajan100% (1)
- Lingualized Occlusion in RDPDocument37 pagesLingualized Occlusion in RDPmujtaba100% (1)
- Provisional MaterialsDocument4 pagesProvisional Materialsveloso.rossana100% (1)
- An Interview With Chris ChangDocument5 pagesAn Interview With Chris ChangDominikaSkórkaNo ratings yet
- Full Mouth Rehabilitation Using Hobo Twin-Stage TechniqueDocument5 pagesFull Mouth Rehabilitation Using Hobo Twin-Stage TechniqueswagataNo ratings yet
- Incisal Guidance & Anterior Occlusion TypesDocument14 pagesIncisal Guidance & Anterior Occlusion TypesAmar BhochhibhoyaNo ratings yet
- Aull. A Study of The Transverse Axis. (1963)Document11 pagesAull. A Study of The Transverse Axis. (1963)Jose Enrique AvilaNo ratings yet
- Hobos PhilosophyDocument189 pagesHobos PhilosophysapnaNo ratings yet
- Vertical Dimension-Literature ReviewDocument6 pagesVertical Dimension-Literature ReviewAvina BanariNo ratings yet
- Densah Bur Surgical Technique ManualDocument44 pagesDensah Bur Surgical Technique ManualLuis Felipe50% (2)
- Rehabilitation of Hemimandibulectomy PatientDocument3 pagesRehabilitation of Hemimandibulectomy PatientAB MISHRANo ratings yet
- A Modification of The Altered Cast TechniqueDocument2 pagesA Modification of The Altered Cast TechniqueChirag Gorasiya100% (1)
- Model Guided Soft Tissue AugmentationDocument10 pagesModel Guided Soft Tissue AugmentationPedro Amaral100% (2)
- Academy of Prosthodontics - Principles Concepts and Practices in Prosthodontics PDFDocument22 pagesAcademy of Prosthodontics - Principles Concepts and Practices in Prosthodontics PDFValonia IreneNo ratings yet
- Twin Stage Procedure for Precise DisocclusionDocument108 pagesTwin Stage Procedure for Precise Disocclusionindra_jeet2009No ratings yet
- Lip Tooth Ridge ClassificationDocument8 pagesLip Tooth Ridge ClassificationNehas HassanNo ratings yet
- SD-V9N1 Bosshart CompleteDocument7 pagesSD-V9N1 Bosshart CompleteAnonymous gjrAZMXB3No ratings yet
- Preparation and restoration of extensively damaged vital teethDocument13 pagesPreparation and restoration of extensively damaged vital teethShu Nser100% (2)
- Aesthetics in Complete Denture - A REVIEWDocument2 pagesAesthetics in Complete Denture - A REVIEWInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Clinical Management of Aquired Defects of MaxillaDocument81 pagesClinical Management of Aquired Defects of Maxillarayavarapu sunilNo ratings yet
- Esthetic Analysis Checklist: 8 Steps For Systematic Treatment PlanningDocument1 pageEsthetic Analysis Checklist: 8 Steps For Systematic Treatment PlanningMarcus EskilssonNo ratings yet
- Esthetics and Implant DentistryDocument18 pagesEsthetics and Implant DentistryVikas Aggarwal0% (1)
- Full Mouth Adhesive Rehabilitation. The Three Stpe Techinique Part 2Document30 pagesFull Mouth Adhesive Rehabilitation. The Three Stpe Techinique Part 2Diego CesarNo ratings yet
- Complete Denture Occlusion PDFDocument25 pagesComplete Denture Occlusion PDFÄpriolia SuNo ratings yet
- Article 009Document9 pagesArticle 009MedstudNo ratings yet
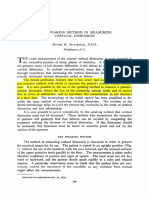
- CLASSIC ARTICLE Clinical Measurement and EvaluationDocument5 pagesCLASSIC ARTICLE Clinical Measurement and EvaluationJesusCordoba100% (2)
- Planning Fixed Partial Dentures For Severely Misaligned AbutmentsDocument7 pagesPlanning Fixed Partial Dentures For Severely Misaligned AbutmentsAntonny VasquezNo ratings yet
- 10867-0 Neoss Anatomical Healing Abutment Manual Hi Res 2009-05-19Document4 pages10867-0 Neoss Anatomical Healing Abutment Manual Hi Res 2009-05-19Nate TaylorNo ratings yet
- Prosthodontic Diagnostic Index (PDI) Classification SystemDocument1 pageProsthodontic Diagnostic Index (PDI) Classification SystemevvallartaNo ratings yet
- The Kinetics of Anterior Tooth DisplayDocument3 pagesThe Kinetics of Anterior Tooth DisplayKristel CruzNo ratings yet
- Full Mouth Rehabilitation: A Smooth Pathway For Complex JourneyDocument8 pagesFull Mouth Rehabilitation: A Smooth Pathway For Complex JourneySkAliHassanNo ratings yet
- Emax CAD Step Cerec-E - 627931Document2 pagesEmax CAD Step Cerec-E - 627931Leo JamesNo ratings yet
- Art Perfil de Emergencia Implantes PDFDocument7 pagesArt Perfil de Emergencia Implantes PDFdiego alenadro trujilloNo ratings yet
- Basic Principles of Obturator Design For Partially Edentulous Patients. Part I: ClassificationDocument69 pagesBasic Principles of Obturator Design For Partially Edentulous Patients. Part I: ClassificationDrFarha NazNo ratings yet
- 9Document23 pages9Rodrigo AngelesNo ratings yet
- Full-Mouth Rehabilitation of A Severe Tooth Wear Case: A Digital, Esthetic and Functional ApproachDocument22 pagesFull-Mouth Rehabilitation of A Severe Tooth Wear Case: A Digital, Esthetic and Functional Approachjose figueroaNo ratings yet
- Journal Club 5Document74 pagesJournal Club 5Naveen Kumar100% (1)
- Full Mouth Rehabilitation in A Case of Severely at PDFDocument6 pagesFull Mouth Rehabilitation in A Case of Severely at PDFMayank MalraNo ratings yet
- Pacquet2022 - Therapeutic Strategy For Cracked TeethDocument17 pagesPacquet2022 - Therapeutic Strategy For Cracked TeethJosé Ramón CuetoNo ratings yet
- Recent Advances in Procthodontics - LD (AMAR)Document102 pagesRecent Advances in Procthodontics - LD (AMAR)Archana PanwarNo ratings yet
- The Neutral Zone in Complete DenturesDocument8 pagesThe Neutral Zone in Complete DenturesToDownload81No ratings yet
- The Rule of the 5 Triangles for Immediate ImplantsDocument12 pagesThe Rule of the 5 Triangles for Immediate ImplantsVikas Aggarwal100% (3)
- Digital Face Bow Transfer Technique Using The Dentofacial Analyzer For Dental Esthetics and 2 D 3 D Smile Design A Clinical ReportDocument9 pagesDigital Face Bow Transfer Technique Using The Dentofacial Analyzer For Dental Esthetics and 2 D 3 D Smile Design A Clinical ReportPaula DiazNo ratings yet
- Denture Sequelae: Common Side Effects of Wearing Complete DenturesDocument58 pagesDenture Sequelae: Common Side Effects of Wearing Complete Denturesaayush100% (2)
- Intern Survival Guide: Department of Internal MedicineDocument35 pagesIntern Survival Guide: Department of Internal MedicineSuvetha TamilarasanNo ratings yet
- Continuum of Care. Simplified Workflow.: Introducing Trilogy EV300Document3 pagesContinuum of Care. Simplified Workflow.: Introducing Trilogy EV300Shubhobrata BhattacherjeeNo ratings yet
- Rosa 2014Document6 pagesRosa 2014Michal PerkowskiNo ratings yet
- MS2 - Neurologic Disorder My ReportDocument30 pagesMS2 - Neurologic Disorder My ReportNeil Lansang BallobanNo ratings yet
- HydramniosDocument31 pagesHydramniosSpandana DepuruNo ratings yet
- Covid TestDocument1 pageCovid TestConcur ConsultancyNo ratings yet
- Using the WHO Surgical Safety Checklist to Improve OutcomesDocument5 pagesUsing the WHO Surgical Safety Checklist to Improve OutcomesKeshava NagalkarNo ratings yet
- 836033cc84 MCQDocument142 pages836033cc84 MCQAnup Lal RajbahakNo ratings yet
- Caso 1 Six SigmaDocument9 pagesCaso 1 Six SigmaNayibe Tatiana Sanchez AlvarezNo ratings yet
- Renal Anatomy EmbryologyDocument31 pagesRenal Anatomy EmbryologySnehal JayaramNo ratings yet
- Complete Ophtho VM555 CoursepackDocument189 pagesComplete Ophtho VM555 Coursepacknandhus2227No ratings yet
- 310-Article Text-582-1-10-20210312-1Document13 pages310-Article Text-582-1-10-20210312-1Ni Putu SwastyNo ratings yet
- Nature of Drug AbuseDocument2 pagesNature of Drug AbuseColin GosbertNo ratings yet
- LabCorp provides age-specific pediatric reference rangesDocument14 pagesLabCorp provides age-specific pediatric reference rangesshoratanNo ratings yet
- Respiratory Distress SyndromeDocument4 pagesRespiratory Distress SyndromeRommar RomeroNo ratings yet
- Detoxification and Chelation Protocols GuideDocument213 pagesDetoxification and Chelation Protocols Guidedoggydog100% (3)
- Emergency Care Emt 13th Edition Ebook PDFDocument61 pagesEmergency Care Emt 13th Edition Ebook PDFadolfo.milliken17896% (47)
- Concept of Garbhashayagata Arbuda With Special Reference To Uterine Fibroid - A Review ArticleDocument8 pagesConcept of Garbhashayagata Arbuda With Special Reference To Uterine Fibroid - A Review Article200202209003No ratings yet
- An International Commentary On Dysphagia and Dysphonia During The COVID 19 PandemicDocument26 pagesAn International Commentary On Dysphagia and Dysphonia During The COVID 19 PandemicRomian ValenciaNo ratings yet
- Menopause - Digital ProgramDocument7 pagesMenopause - Digital ProgramU of T MedicineNo ratings yet
- Pedia History Taking (Oct9)Document5 pagesPedia History Taking (Oct9)fall autumnNo ratings yet
- Bag technique nursing careDocument2 pagesBag technique nursing careDanz KieNo ratings yet
- Aquagenic Palmoplantar Keratoderma With Dorsal Hand Involvement in An Adolescent FemaleDocument2 pagesAquagenic Palmoplantar Keratoderma With Dorsal Hand Involvement in An Adolescent FemaleTher RayNo ratings yet
- LS2 Scientific - Critical Thinking JUNIOR HIGH SCHOOL PDFDocument91 pagesLS2 Scientific - Critical Thinking JUNIOR HIGH SCHOOL PDFNaomae Lagrada VasalloNo ratings yet
- EAU Guidelines On Urological Infections 2021Document74 pagesEAU Guidelines On Urological Infections 2021ioana teodorescuNo ratings yet
- Bedside Hemodynamic MonitoringDocument26 pagesBedside Hemodynamic MonitoringBrad F LeeNo ratings yet
- 9 Steam InhalationDocument2 pages9 Steam InhalationKen Morales Alcantara100% (1)
- A Student Manual of Clinical Skills 13 7 8Document194 pagesA Student Manual of Clinical Skills 13 7 8mofath100% (5)
- Home Care For Your Kids TeethDocument2 pagesHome Care For Your Kids TeethDr. Kristin ElliotNo ratings yet
- Acute & Critical 2Document167 pagesAcute & Critical 2Kissy BesarioNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (14)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Daniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisFrom EverandDaniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisRating: 3.5 out of 5 stars3.5/5 (130)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)