You might also like
- Maternal and Child Health Nursing PDFDocument40 pagesMaternal and Child Health Nursing PDFTina Talmadge100% (5)
- MDS Oral Medicine Question Papers 2002Document5 pagesMDS Oral Medicine Question Papers 2002Niyas UmmerNo ratings yet
- IvfDocument24 pagesIvftariqul13017No ratings yet
- InfertilityDocument10 pagesInfertilityHarish Labana100% (1)
- Recent Advancements in Infertility Techniques AloneDocument111 pagesRecent Advancements in Infertility Techniques AlonesanthanalakshmiNo ratings yet
- Biology Investigatory Reproductive HealthDocument12 pagesBiology Investigatory Reproductive HealthVIKRAMVIKKYOFFICIAL83% (41)
- What Is in Vitro Fertilization (IVF) and Its ProcessDocument4 pagesWhat Is in Vitro Fertilization (IVF) and Its ProcessPlanet womenNo ratings yet
- Infertility - Definition, Causes, Diagnostic Procedures AND CouncellingDocument37 pagesInfertility - Definition, Causes, Diagnostic Procedures AND CouncellingvincentsharonNo ratings yet
- Notes-Maternal Health NursingDocument22 pagesNotes-Maternal Health NursingRachael Crossgrove100% (4)
- Activity DesignDocument2 pagesActivity DesignRhu New Lucena90% (20)
- Breast Cancer 1Document194 pagesBreast Cancer 1Connie SianiparNo ratings yet
- Procedure: in Vitro Fertilization (Ivf)Document7 pagesProcedure: in Vitro Fertilization (Ivf)Lovely SarangiNo ratings yet
- Maternal and Child Health NursingDocument39 pagesMaternal and Child Health NursingRena VilNo ratings yet
- Recent Advancement in Infertility Management and Adoption ProcessDocument160 pagesRecent Advancement in Infertility Management and Adoption ProcessBhawna JoshiNo ratings yet
- INFERTILITY Obg SeminarDocument19 pagesINFERTILITY Obg SeminarDelphy Varghese100% (2)
- MCHN Reviewer 1Document24 pagesMCHN Reviewer 1Steam LcNo ratings yet
- INFERTILITY Obg SeminarDocument19 pagesINFERTILITY Obg SeminarDelphy VargheseNo ratings yet
- Orthodontic Management in Children With Special NeedsDocument5 pagesOrthodontic Management in Children With Special NeedsAnonymous LnWIBo1GNo ratings yet
- Contraception and SterilizationDocument4 pagesContraception and SterilizationLouie Kem Anthony BabaranNo ratings yet
- SUBFERTILITYDocument46 pagesSUBFERTILITYLalisaM Activity100% (1)
- Infertility AssignmentDocument26 pagesInfertility Assignmentbrilliantraajpoot86% (7)
- NCM 109 Resource UnitDocument51 pagesNCM 109 Resource UnitDaryl Adrian RecaidoNo ratings yet
- Getting Pregnant Naturally: Healthy Choices To Boost Your Chances Of Conceiving Without Fertility DrugsFrom EverandGetting Pregnant Naturally: Healthy Choices To Boost Your Chances Of Conceiving Without Fertility DrugsRating: 3.5 out of 5 stars3.5/5 (8)
- InfertilityDocument24 pagesInfertilityDeepa ThomasNo ratings yet
- Semi Finals CHAPTER IVDocument5 pagesSemi Finals CHAPTER IVjacobprince0016No ratings yet
- INFERTILITYDocument6 pagesINFERTILITYIGA ABRAHAMNo ratings yet
- Surrogate Embryo TransferDocument4 pagesSurrogate Embryo TransferJanah PagayNo ratings yet
- SDL 3 MCN 1Document3 pagesSDL 3 MCN 1Milagros Florita100% (1)
- Day 2 - NCM 109 Lec - Infertile CoupleDocument101 pagesDay 2 - NCM 109 Lec - Infertile CoupleMiguel TolentinoNo ratings yet
- NCM 109 Semi Final CHAPTER IVDocument6 pagesNCM 109 Semi Final CHAPTER IV37. Vanesa mae ReyesNo ratings yet
- How Is Male Infertility Treated?Document9 pagesHow Is Male Infertility Treated?Rio DanteNo ratings yet
- Unit 3 Maternal Health Care Edited 2015Document43 pagesUnit 3 Maternal Health Care Edited 2015Londera BainNo ratings yet
- Group1 OB Ward-Case StudyDocument10 pagesGroup1 OB Ward-Case StudyAnthony Seth AguilandoNo ratings yet
- In Vitro FertilizationDocument4 pagesIn Vitro FertilizationFrances Kaye Sta. CruzNo ratings yet
- MaternalDocument41 pagesMaternalUc_tweenNo ratings yet
- Infertility and Climacteric CrisisDocument4 pagesInfertility and Climacteric Crisisgeorgeloto12No ratings yet
- MCN2 Prelim-NotesDocument4 pagesMCN2 Prelim-NotesChris AnnNo ratings yet
- Infertility 2023Document5 pagesInfertility 2023Charlette GuadalupeNo ratings yet
- Upd. MEANING OF INFERTILITYDocument9 pagesUpd. MEANING OF INFERTILITYCharles DebrahNo ratings yet
- (Text) Maternal and Child Health NursingDocument40 pages(Text) Maternal and Child Health NursingVia H.No ratings yet
- Nursing-Interventions MCN For Infertility MenDocument2 pagesNursing-Interventions MCN For Infertility MenRio DanteNo ratings yet
- The Undescended Testis: A.E. MackinnonDocument4 pagesThe Undescended Testis: A.E. MackinnonAin GhazaliNo ratings yet
- Notes On Subfertility AssessmentDocument5 pagesNotes On Subfertility AssessmentHassen ZabalaNo ratings yet
- InfertilityDocument46 pagesInfertilityمحمد عماد عليNo ratings yet
- Oyelowo 2007Document9 pagesOyelowo 2007Sinarsih DaczhyyNo ratings yet
- NCM 107Document83 pagesNCM 107Jan Rae Barnatia AtienzaNo ratings yet
- 4 Nursing Care For The Family in Need of Reproductive Life PlanningDocument5 pages4 Nursing Care For The Family in Need of Reproductive Life PlanningHarry Venzon JaboliNo ratings yet
- SOCIO 102-Lesson 5: The Process of ReproductionDocument33 pagesSOCIO 102-Lesson 5: The Process of ReproductionRessaNo ratings yet
- Chapter 8: Nursing Care of The Subfertile CoupleDocument10 pagesChapter 8: Nursing Care of The Subfertile CoupleAlyssaGrandeMontimorNo ratings yet
- PseudopregnancyDocument21 pagesPseudopregnancyShanmathiNo ratings yet
- Infertility 230411173332 Cc62ed95Document50 pagesInfertility 230411173332 Cc62ed95Kapil YadavNo ratings yet
- Complications of Labor and DeveryDocument7 pagesComplications of Labor and DeveryMon Russel FriasNo ratings yet
- Obstetirc NursingDocument36 pagesObstetirc NursingGlenn Daryll SantosNo ratings yet
- In Vitro FertilizationDocument10 pagesIn Vitro Fertilizationbethelhemalemu126No ratings yet
- 1 Infertility 2022Document138 pages1 Infertility 2022CAÑADA, JOHANNELYN M.No ratings yet
- ARTDocument36 pagesARTTtyyfff Fyyu89-No ratings yet
- Family Planning: Prepared By: Kieth C. Seresula, RM, BSMDocument109 pagesFamily Planning: Prepared By: Kieth C. Seresula, RM, BSMKieth SeresulaNo ratings yet
- Case StudyDocument9 pagesCase StudyChristian San Jose TanNo ratings yet
- (L7) - Reproductive Health - Aug 23, 2019 - FridayDocument49 pages(L7) - Reproductive Health - Aug 23, 2019 - Fridaysarthak kedariNo ratings yet
- Problems in ReproductionDocument23 pagesProblems in ReproductionRoccabeth VillanuevaNo ratings yet
- Mid 101 Assignments Module 1-8Document7 pagesMid 101 Assignments Module 1-8Nicole DeusNo ratings yet
- INFERTILITYDocument30 pagesINFERTILITYShagun TyagiNo ratings yet
- Module 7 High Risk Newborn 2023Document46 pagesModule 7 High Risk Newborn 2023DemokGraganzaJrNo ratings yet
- Care of Mother and Child at Risk or With Problems (Acute and Chronic)Document2 pagesCare of Mother and Child at Risk or With Problems (Acute and Chronic)DemokGraganzaJrNo ratings yet
- Module 10 Endocrine Disorders 2023Document27 pagesModule 10 Endocrine Disorders 2023DemokGraganzaJrNo ratings yet
- Drug Study FormatDocument1 pageDrug Study FormatDemokGraganzaJrNo ratings yet
- Activity 4-Creative ArtsDocument3 pagesActivity 4-Creative Artsapi-568507733No ratings yet
- Cirugías de La Glándula Mamaria en El BovinoDocument20 pagesCirugías de La Glándula Mamaria en El BovinoJavier HernandezNo ratings yet
- Backgrounder Pearl Gamblers Experience at Misericordia Community Hospital in EdmontonDocument2 pagesBackgrounder Pearl Gamblers Experience at Misericordia Community Hospital in EdmontonCityNewsTorontoNo ratings yet
- Breech Presentation: - by Drtejaswini K.RDocument41 pagesBreech Presentation: - by Drtejaswini K.Rjssamc prasootitantraNo ratings yet
- Congenital Anomalies 2Document59 pagesCongenital Anomalies 2Hamss AhmedNo ratings yet
- Public Health Neurological Disorder 2019Document232 pagesPublic Health Neurological Disorder 2019Klinik FiraraNo ratings yet
- Get The Facts About COVID-19 Vaccines - Mayo ClinicDocument10 pagesGet The Facts About COVID-19 Vaccines - Mayo ClinicLuna BellatrixNo ratings yet
- Hair Loss AnswersDocument241 pagesHair Loss AnswersRobert HarmathNo ratings yet
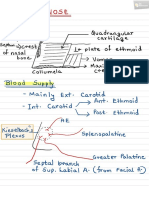
- Nose PDFDocument6 pagesNose PDFNiranjanPandeyNo ratings yet
- WHO 2011 Typhoid FeverDocument39 pagesWHO 2011 Typhoid FeverVizzi Alvi Fitrah NasutionNo ratings yet
- Final Research ProposalDocument37 pagesFinal Research ProposalAhmed AbdoNo ratings yet
- Emergency Oxygen Therapy in The Dental Practice: Administration and ManagementDocument4 pagesEmergency Oxygen Therapy in The Dental Practice: Administration and ManagementAndi Suchy Qumala SarieNo ratings yet
- Management of Ocular Chemical InjuriesDocument82 pagesManagement of Ocular Chemical InjuriesAfiqah FaizalNo ratings yet
- Clinical Handbook of Infectious Diseases in Farm AnimalsDocument146 pagesClinical Handbook of Infectious Diseases in Farm Animalsigorgalopp100% (1)
- 02 Chain of SurvivalDocument1 page02 Chain of SurvivalHatem FaroukNo ratings yet
- Adrenal Gland Disease in Ferrets: Elisabeth Simone-Freilicher, DVM, DABVP-AvianDocument13 pagesAdrenal Gland Disease in Ferrets: Elisabeth Simone-Freilicher, DVM, DABVP-AvianGabriel MendesNo ratings yet
- 5 Cover Letter Samples For Your Scientific ManuscriptDocument11 pages5 Cover Letter Samples For Your Scientific ManuscriptAlejandra J. Troncoso100% (2)
- Men and Chlamydia ScreeningDocument28 pagesMen and Chlamydia ScreeningMen's Health ForumNo ratings yet
- Management of Portal Hypertension in Children: Ahmed Mahmoud El-Tawil, MSC, MRCS, PHDDocument9 pagesManagement of Portal Hypertension in Children: Ahmed Mahmoud El-Tawil, MSC, MRCS, PHDNulul Ci LoolyNo ratings yet
- Joker LineDocument10 pagesJoker LineVivekanand ChandrashekarNo ratings yet
- Pain Management, The Veterinary Technicians PerspectyveDocument14 pagesPain Management, The Veterinary Technicians PerspectyveClínica Veterinaria TODOVETNo ratings yet
- IvpDocument18 pagesIvpFranz SalazarNo ratings yet
- Do Vaccinations Cause Autism?Document3 pagesDo Vaccinations Cause Autism?Josh BarberaNo ratings yet
- Acute GlomerulonephritisDocument1 pageAcute GlomerulonephritisAyrheen FornolesNo ratings yet
- Kelsey Nash ResumeDocument2 pagesKelsey Nash Resumeapi-349578979No ratings yet
- Assessment of Antibacterial Ointment of Carabao GrassDocument20 pagesAssessment of Antibacterial Ointment of Carabao GrassMiah Grace QuimpoNo ratings yet