You might also like
- InfertilityDocument10 pagesInfertilityHarish Labana100% (1)
- Infertility CausesDocument45 pagesInfertility CausesDemokGraganzaJrNo ratings yet
- INFERTILITY Obg SeminarDocument19 pagesINFERTILITY Obg SeminarDelphy Varghese100% (2)
- INFERTILITY Obg SeminarDocument19 pagesINFERTILITY Obg SeminarDelphy VargheseNo ratings yet
- Infertility 230411173332 Cc62ed95Document50 pagesInfertility 230411173332 Cc62ed95Kapil YadavNo ratings yet
- Zoology FyDocument12 pagesZoology FyByomakeshNo ratings yet
- University of Energy and Natural Resources infertility fact sheetDocument9 pagesUniversity of Energy and Natural Resources infertility fact sheetCharles DebrahNo ratings yet
- Getting Pregnant Naturally: Healthy Choices To Boost Your Chances Of Conceiving Without Fertility DrugsFrom EverandGetting Pregnant Naturally: Healthy Choices To Boost Your Chances Of Conceiving Without Fertility DrugsRating: 3.5 out of 5 stars3.5/5 (8)
- Notes On Subfertility AssessmentDocument5 pagesNotes On Subfertility AssessmentHassen ZabalaNo ratings yet
- The Male Biological Clock: The Startling News About Aging, Sexuality, and Fertility in MenFrom EverandThe Male Biological Clock: The Startling News About Aging, Sexuality, and Fertility in MenRating: 3 out of 5 stars3/5 (1)
- What Is InfertilityDocument10 pagesWhat Is InfertilityTemitopeNo ratings yet
- Male InfertilityDocument1 pageMale InfertilityemanNo ratings yet
- Nursing-Interventions MCN For Infertility MenDocument2 pagesNursing-Interventions MCN For Infertility MenRio DanteNo ratings yet
- Infertility and Climacteric CrisisDocument4 pagesInfertility and Climacteric Crisisgeorgeloto12No ratings yet
- Causes and Diagnosis of InfertilityDocument16 pagesCauses and Diagnosis of InfertilityJyoti Amit TiwariNo ratings yet
- Day 2 - NCM 109 Lec - Infertile CoupleDocument101 pagesDay 2 - NCM 109 Lec - Infertile CoupleMiguel TolentinoNo ratings yet
- ئاما ده یا سه ركرده یاDocument12 pagesئاما ده یا سه ركرده یاbirhatgulli79No ratings yet
- PCOS No More: Take Control of PCOS Symptoms & Treatments - A Holistic System of Lifestyle Changes, Diet, & Exercises to Beat Polycystic Ovary Syndrome Naturally & Permanently. PCOS Recipes Included.From EverandPCOS No More: Take Control of PCOS Symptoms & Treatments - A Holistic System of Lifestyle Changes, Diet, & Exercises to Beat Polycystic Ovary Syndrome Naturally & Permanently. PCOS Recipes Included.Rating: 4 out of 5 stars4/5 (3)
- InfertilityDocument46 pagesInfertilityOmg ,No ratings yet
- Infertility: SymptomsDocument9 pagesInfertility: SymptomsVyshak KrishnanNo ratings yet
- InfertilityDocument23 pagesInfertilityoforiamponsahdaniel970No ratings yet
- Male Factor InfertilityDocument18 pagesMale Factor InfertilityKenan OmurtagNo ratings yet
- INFERTILITY CAUSES AND TREATMENTDocument14 pagesINFERTILITY CAUSES AND TREATMENTNishaThakuri0% (1)
- INFERTILITYDocument30 pagesINFERTILITYShagun TyagiNo ratings yet
- InfertilityDocument30 pagesInfertilityPatience Yakubu PaulNo ratings yet
- Male Infertility 12-1-13 UserTemp-5 PDFDocument4 pagesMale Infertility 12-1-13 UserTemp-5 PDFGhulam MustafaNo ratings yet
- Subfertility: Definition and ClassificationsDocument18 pagesSubfertility: Definition and ClassificationsAnonymous 0C4OZmRNo ratings yet
- THE PHYSICAL AND SEXUAL SELFDocument20 pagesTHE PHYSICAL AND SEXUAL SELFsigma rusNo ratings yet
- InfertilityDocument23 pagesInfertilityDelphy Varghese100% (4)
- Nadia LBM 1 KBDocument25 pagesNadia LBM 1 KBNadia Dwi NurhalizaNo ratings yet
- Understanding the Physical and Sexual SelfDocument9 pagesUnderstanding the Physical and Sexual SelfKrishna Faith P. DelaraNo ratings yet
- What Is InfertilityDocument11 pagesWhat Is InfertilityReyansh gargNo ratings yet
- INFERTILITY Purnima SeminarDocument9 pagesINFERTILITY Purnima SeminarBhanesh SahuNo ratings yet
- IMPOTENCE AND STERILITY: CAUSES, EXAMINATION AND MEDICOLEGAL ASPECTSDocument28 pagesIMPOTENCE AND STERILITY: CAUSES, EXAMINATION AND MEDICOLEGAL ASPECTSSachin SinghNo ratings yet
- Puberty, fertility and menopause issues exploredDocument7 pagesPuberty, fertility and menopause issues exploredElias VouzounisNo ratings yet
- Infertility AssignmentDocument26 pagesInfertility Assignmentbrilliantraajpoot86% (7)
- Recent Advancements in Infertility TreatmentsDocument71 pagesRecent Advancements in Infertility TreatmentsNimi SimonNo ratings yet
- Infertilityseminarppt 190718134710Document77 pagesInfertilityseminarppt 190718134710subiNo ratings yet
- Infertility Diagnosis and ManagementDocument9 pagesInfertility Diagnosis and ManagementSinarsih DaczhyyNo ratings yet
- Menstrual Disorders in Adolescents: The Internet Journal of Gynecology and ObstetricsDocument34 pagesMenstrual Disorders in Adolescents: The Internet Journal of Gynecology and ObstetricsNayla Adira04No ratings yet
- Notes Infertility Delayed PubertyDocument9 pagesNotes Infertility Delayed PubertyTONY GO AWAYNo ratings yet
- Week 6 Nursing Care of The Family With Reproductive DisordersDocument27 pagesWeek 6 Nursing Care of The Family With Reproductive DisordersStefhanie Mae LazaroNo ratings yet
- Infertility GuideDocument24 pagesInfertility GuideDeepa ThomasNo ratings yet
- Nursing Administration ManualDocument6 pagesNursing Administration ManualKenee SamboNo ratings yet
- What Is InfertilityDocument19 pagesWhat Is InfertilityArlene Agnawa SapaoNo ratings yet
- InfertilityDocument5 pagesInfertilityRupert BautistaNo ratings yet
- Chapter-2-Unpacking-the-Self-The-Sexual-SelfDocument3 pagesChapter-2-Unpacking-the-Self-The-Sexual-SelfcondrillondenmarjohnNo ratings yet
- You Are What You Secrete: A Practical Guide to Common, Hormone-Related DiseasesFrom EverandYou Are What You Secrete: A Practical Guide to Common, Hormone-Related DiseasesNo ratings yet
- Adolescent Gynecologic Care QUESTIONS 1, 2, 3Document7 pagesAdolescent Gynecologic Care QUESTIONS 1, 2, 3patelkn_2005No ratings yet
- Physical and Sexual SelfDocument41 pagesPhysical and Sexual SelfFlorilyn Dela CruzNo ratings yet
- CUA Guideline on Work-Up and Management of Azoospermic MalesDocument11 pagesCUA Guideline on Work-Up and Management of Azoospermic Malesandi hamatajNo ratings yet
- InfertilityDocument30 pagesInfertilityEka KurniatiNo ratings yet
- The Physical and Sexual SelfDocument30 pagesThe Physical and Sexual SelfLorna Edeza EvangelistaNo ratings yet
- Assesment of Amen or RheaDocument49 pagesAssesment of Amen or Rheakhadzx100% (2)
- Group 1 Research Ethcs FinalDocument23 pagesGroup 1 Research Ethcs FinalIGA ABRAHAMNo ratings yet
- Ethical Issues in ResearchDocument8 pagesEthical Issues in ResearchIGA ABRAHAMNo ratings yet
- Felester Research, 2022Document31 pagesFelester Research, 2022IGA ABRAHAMNo ratings yet
- Rhabdoviruses by KennedyDocument36 pagesRhabdoviruses by KennedyIGA ABRAHAMNo ratings yet
- Concept Paper FinalDocument6 pagesConcept Paper FinalIGA ABRAHAMNo ratings yet
- BALTIMOREDocument3 pagesBALTIMOREIGA ABRAHAMNo ratings yet
- Late Antenatal Care Booking FactorsDocument6 pagesLate Antenatal Care Booking FactorsIGA ABRAHAMNo ratings yet
- Group 1 Validity FinalDocument30 pagesGroup 1 Validity FinalIGA ABRAHAMNo ratings yet
- 5a-Oncogenic and Retroviruses 2017Document77 pages5a-Oncogenic and Retroviruses 2017IGA ABRAHAMNo ratings yet
- Concept Paper by Mauchi TimothyDocument5 pagesConcept Paper by Mauchi TimothyIGA ABRAHAMNo ratings yet
- Baltimore To Add in ThereDocument2 pagesBaltimore To Add in ThereIGA ABRAHAMNo ratings yet
- Organisation StructureDocument7 pagesOrganisation StructureIGA ABRAHAMNo ratings yet
- Papovavirus Family Characteristics and DiseasesDocument25 pagesPapovavirus Family Characteristics and DiseasesIGA ABRAHAMNo ratings yet
- Data Collection Methods and ToolsDocument32 pagesData Collection Methods and ToolsIGA ABRAHAMNo ratings yet
- Appleton & Lange Review of Anatomy PDFDocument157 pagesAppleton & Lange Review of Anatomy PDFherry2sw100% (2)
- Anatomy Short Answer Questions Bank Lower LimbDocument4 pagesAnatomy Short Answer Questions Bank Lower LimbIGA ABRAHAMNo ratings yet
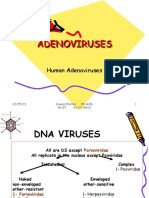
- 1 AdenovirusesDocument36 pages1 AdenovirusesIGA ABRAHAMNo ratings yet
- CVS, GIT and Respiratory ChangesDocument17 pagesCVS, GIT and Respiratory ChangesIGA ABRAHAMNo ratings yet
- Curriculum Vitire COSSY NAMALEDocument4 pagesCurriculum Vitire COSSY NAMALEIGA ABRAHAMNo ratings yet
- OrganizingDocument18 pagesOrganizingIGA ABRAHAMNo ratings yet
- Aine RSRCHDocument59 pagesAine RSRCHIGA ABRAHAMNo ratings yet
- NURSING MANAGEMENT AND ADMINISTRATION-feb2022Document42 pagesNURSING MANAGEMENT AND ADMINISTRATION-feb2022IGA ABRAHAM100% (1)
- Akatukunda Precious Final Research ProposalDocument46 pagesAkatukunda Precious Final Research ProposalIGA ABRAHAMNo ratings yet
- ReportDocument2 pagesReportIGA ABRAHAMNo ratings yet
- OrganizingDocument18 pagesOrganizingIGA ABRAHAMNo ratings yet
- Pay Ugx. 2,670,000 to Kabale University with Zeepay Ref 2230006301685Document1 pagePay Ugx. 2,670,000 to Kabale University with Zeepay Ref 2230006301685IGA ABRAHAMNo ratings yet
- Reproductive System Cancers by EasterDocument19 pagesReproductive System Cancers by EasterIGA ABRAHAM100% (1)
- Pelvic Inflammatory DiseaseDocument4 pagesPelvic Inflammatory DiseaseIGA ABRAHAMNo ratings yet
- 2023 Diary Planner Template Excel 15Document24 pages2023 Diary Planner Template Excel 15Viviane CoraNo ratings yet
- Vaginal Discharge by EasterDocument4 pagesVaginal Discharge by EasterIGA ABRAHAMNo ratings yet
- Taking Obstetrical HistoryDocument20 pagesTaking Obstetrical Historymawada abdallaNo ratings yet
- Wa0002.Document21 pagesWa0002.Deepak E deepakNo ratings yet
- Drugs in Sport EssayDocument5 pagesDrugs in Sport Essaysbbftinbf100% (2)
- Group 6 Sexual SelfDocument44 pagesGroup 6 Sexual SelfFelipe GuadizNo ratings yet
- Abortion Law and Medical Ethics AnalysisDocument4 pagesAbortion Law and Medical Ethics AnalysislvohNo ratings yet
- Ectopic PregnancyDocument26 pagesEctopic PregnancyMalek.Fakher1900No ratings yet
- Biology Investigatory FileDocument13 pagesBiology Investigatory FileSidra khan100% (2)
- Puberty & AdolescenceDocument15 pagesPuberty & Adolescencejean greyNo ratings yet
- OB PEDIA Practice Questions (100 Items)Document8 pagesOB PEDIA Practice Questions (100 Items)kara.adolacion-19No ratings yet
- Body System: Reproductive - FemaleDocument2 pagesBody System: Reproductive - FemaleKakah MoNo ratings yet
- Endometritis: Cabangon Saagundo Abejar Granzon Mayowa TabañagDocument14 pagesEndometritis: Cabangon Saagundo Abejar Granzon Mayowa TabañagChresia Schae MondejarNo ratings yet
- Sci 5 PPT q2 WK 1 Day 1-5 (Autosaved)Document93 pagesSci 5 PPT q2 WK 1 Day 1-5 (Autosaved)renato.minaNo ratings yet
- The Three Perspectives on Abortion in the PhilippinesDocument4 pagesThe Three Perspectives on Abortion in the PhilippinesLamour Manlapaz100% (1)
- Jurnal Bhs Inggris FixDocument8 pagesJurnal Bhs Inggris FixKurniawan ramadhanaNo ratings yet
- UnwantedDocument1 pageUnwantedTerence SalamatNo ratings yet
- Menstrual Cycle QuizDocument3 pagesMenstrual Cycle QuizCyril CauilanNo ratings yet
- Emergency Contaception by James TrussellDocument37 pagesEmergency Contaception by James TrussellAdityaWijayaNo ratings yet
- Ibnu Sina Hospital, Tuesday, April 19th, 2022 (Period April 10th - 17th, 2022)Document4 pagesIbnu Sina Hospital, Tuesday, April 19th, 2022 (Period April 10th - 17th, 2022)MirahAvishaNo ratings yet
- THE DOWNSIDE OF SURROGACY IN THE PHILIPPINESDocument13 pagesTHE DOWNSIDE OF SURROGACY IN THE PHILIPPINESvina lorraine marasiganNo ratings yet
- ARSHDocument1 pageARSHSaurav SamadhiyaNo ratings yet
- Unit 4 Maternal ConceptsDocument8 pagesUnit 4 Maternal ConceptsEunice TrinidadNo ratings yet
- #12 - NCM 109 (Rle) - TransesDocument4 pages#12 - NCM 109 (Rle) - TransesJaimie BanaagNo ratings yet
- Orca Share Media1496246332671Document5 pagesOrca Share Media1496246332671HCX dghhqNo ratings yet
- Factors Leading to Low Family Planning in CagayanDocument57 pagesFactors Leading to Low Family Planning in Cagayanmarie judimor gomezNo ratings yet
- Case Study 114: InstructionsDocument3 pagesCase Study 114: InstructionsCheska PalomaNo ratings yet
- Cot First QuarterDocument15 pagesCot First QuarterRowena Torres DahiligNo ratings yet
- Infertility NotesDocument41 pagesInfertility NotesPrasadNo ratings yet
- Modern Contraceptive Utilization and Associated Factors Among Women of Reproductive Age at Fort Portal Regional Referral Hospital, Uganda.Document19 pagesModern Contraceptive Utilization and Associated Factors Among Women of Reproductive Age at Fort Portal Regional Referral Hospital, Uganda.KIU PUBLICATION AND EXTENSIONNo ratings yet
- The Parts of The Human Reproductive System and Their FunctionsDocument13 pagesThe Parts of The Human Reproductive System and Their FunctionsRhodora Rendon OrizonteNo ratings yet
- Obstectric and Gynaecology 3 Year 6 Batch: MCQ (Obe - One Best Answer)Document5 pagesObstectric and Gynaecology 3 Year 6 Batch: MCQ (Obe - One Best Answer)Zeke EdgeNo ratings yet