You might also like
- NP3Document12 pagesNP3Lyca BerinNo ratings yet
- Activation Vs Experiential Avoidance As A Transdia PDFDocument12 pagesActivation Vs Experiential Avoidance As A Transdia PDFpsicologia ejartNo ratings yet
- Psikodinamika Tenrikeefe2014Document60 pagesPsikodinamika Tenrikeefe2014AzisahhNo ratings yet
- Recover From AdversityDocument20 pagesRecover From AdversityA. AlejandroNo ratings yet
- A Multi-Method Assessment of Attentional Processes in Chronic, Treatment-Resistant Depression Mira Cladder-Micus A, E, - , Janna N. VrijsDocument9 pagesA Multi-Method Assessment of Attentional Processes in Chronic, Treatment-Resistant Depression Mira Cladder-Micus A, E, - , Janna N. VrijsIsabelaValeria Idrovo-LuqueNo ratings yet
- 2019 EspenDocument10 pages2019 Espennermal93No ratings yet
- Resilience and Mental Health NursingDocument15 pagesResilience and Mental Health NursingDWNo ratings yet
- Cusack Et Al. (2016)Document54 pagesCusack Et Al. (2016)jehonol883No ratings yet
- Hakamata 2013Document7 pagesHakamata 2013bordian georgeNo ratings yet
- Asmundson, 2019Document15 pagesAsmundson, 2019Sérgio FonsecaNo ratings yet
- Validation Study of A Portuguese Version of The Hospital Anxiety and Depression ScaleDocument14 pagesValidation Study of A Portuguese Version of The Hospital Anxiety and Depression ScaleBruno Miguel MagalhãesNo ratings yet
- The Effectiveness of Interpersonal Psychotherapy For Posttraumatic Stress Disorder (PTSD)Document10 pagesThe Effectiveness of Interpersonal Psychotherapy For Posttraumatic Stress Disorder (PTSD)IJAR JOURNALNo ratings yet
- Saracutu2017 PDFDocument40 pagesSaracutu2017 PDFDiana SchlittlerNo ratings yet
- 10 3389@fneur 2020 00230Document12 pages10 3389@fneur 2020 00230nanikNo ratings yet
- Research Paper On Post Traumatic Stress DisorderDocument8 pagesResearch Paper On Post Traumatic Stress Disorderegvhzwcd100% (1)
- Work Stress and Resident Burnout, Before and During The COVID-19 Pandemia: An Up-DateDocument11 pagesWork Stress and Resident Burnout, Before and During The COVID-19 Pandemia: An Up-DateLUIS EDUARDO MEDINA MUÑANTENo ratings yet
- J Neubiorev 2018 01 012Document33 pagesJ Neubiorev 2018 01 012Adriana NegrescuNo ratings yet
- 10.1016/j.nedt.2016.02.003: Nurse Education TodayDocument32 pages10.1016/j.nedt.2016.02.003: Nurse Education TodayAri YuanNo ratings yet
- Interventions For Common Mental Health Problems Among University Students-with-cover-page-V2Document11 pagesInterventions For Common Mental Health Problems Among University Students-with-cover-page-V2Ana Luiza Ferreira PsiNo ratings yet
- Association Between Illness Representation and Psychological Distress in Stroke PatientsDocument9 pagesAssociation Between Illness Representation and Psychological Distress in Stroke PatientsFahim Abrar KhanNo ratings yet
- Accepted Manuscript: 10.1016/j.ijosm.2016.05.003Document25 pagesAccepted Manuscript: 10.1016/j.ijosm.2016.05.003yoverNo ratings yet
- BrueraDocument21 pagesBrueraThatiana GimenesNo ratings yet
- Psikodinamika2015 PDFDocument48 pagesPsikodinamika2015 PDFAzisahhNo ratings yet
- Clinical Psychology Review: 10.1016/j.cpr.2015.07.004Document48 pagesClinical Psychology Review: 10.1016/j.cpr.2015.07.004AzisahhNo ratings yet
- Paper 5Document13 pagesPaper 5isilecarosvialNo ratings yet
- Abdominal Acupuncture For DepressionDocument35 pagesAbdominal Acupuncture For DepressionAGNESE YOLOTZIN OLIVERA TORO REYESNo ratings yet
- Effectiveness of Psychoeducation Intervention On Post-Traumatic StressDocument11 pagesEffectiveness of Psychoeducation Intervention On Post-Traumatic StressIin InaraNo ratings yet
- Gratitude JournalingDocument5 pagesGratitude JournalingPreeti ChouhanNo ratings yet
- Resilience in Cancer PatientsDocument35 pagesResilience in Cancer PatientsFlory23ibc23No ratings yet
- Torres-Reading On PTSDDocument15 pagesTorres-Reading On PTSDbabiNo ratings yet
- Articol 1 SPVDocument8 pagesArticol 1 SPVStroe EmmaNo ratings yet
- Final Report On Stress ManagementDocument23 pagesFinal Report On Stress ManagementAbhinab DasNo ratings yet
- 10 1016@j CTCP 2018 06 011 PDFDocument42 pages10 1016@j CTCP 2018 06 011 PDFBelenFlyawayNo ratings yet
- Emotional Intelligence and Personality in Major Depression: Trait Versus State EffectsDocument6 pagesEmotional Intelligence and Personality in Major Depression: Trait Versus State EffectsLaura AlfaroNo ratings yet
- Artikel InternasionalDocument15 pagesArtikel InternasionalFitriatul MunawarohNo ratings yet
- Attachment and Posttraumatic Stress Disorder in Multiple Trauma SamplesDocument9 pagesAttachment and Posttraumatic Stress Disorder in Multiple Trauma SamplesRaudhiatul AzzahraNo ratings yet
- Cortisol Response To Stress - The Role of Expectancy and Anticipatory Stress RegulationDocument10 pagesCortisol Response To Stress - The Role of Expectancy and Anticipatory Stress RegulationDra. María José CastilloNo ratings yet
- Impact of Post-Traumatic Stress Disorder and Job-RelatedDocument5 pagesImpact of Post-Traumatic Stress Disorder and Job-RelatedFlorentina SisuNo ratings yet
- Accepted Manuscript: Une Adrian J. BradleyDocument63 pagesAccepted Manuscript: Une Adrian J. BradleyJuliana MejiaNo ratings yet
- Clinical Psychology Review: Michelle L. Moulds, Madelyne A. Bisby, Jennifer Wild, Richard A. Bryant TDocument16 pagesClinical Psychology Review: Michelle L. Moulds, Madelyne A. Bisby, Jennifer Wild, Richard A. Bryant TLAURA CRISTINA TORRES CATANONo ratings yet
- Self-Determination FEP AssociationsDocument15 pagesSelf-Determination FEP Associationssaurav.das2030No ratings yet
- The Role of Positive Emotion and Contributions of Positive Psychology inDocument17 pagesThe Role of Positive Emotion and Contributions of Positive Psychology ine orlando mocaNo ratings yet
- J Jcbs 2019 02 005Document36 pagesJ Jcbs 2019 02 005kenth yuNo ratings yet
- HammenDocument18 pagesHammenAndreia AlmeidaNo ratings yet
- 1 s2.0 S2212144719301206 Main PDFDocument7 pages1 s2.0 S2212144719301206 Main PDFgalatimeNo ratings yet
- Ambulatory Assessment For Precision Psychiatry - Foundations, Current Developments and Future AvenuesDocument13 pagesAmbulatory Assessment For Precision Psychiatry - Foundations, Current Developments and Future AvenuesSGUNo ratings yet
- Classen Et Al. (2020) A Pilot RCT of A Body-Oriented Group Therapy For Complex Trauma SurvivorsDocument18 pagesClassen Et Al. (2020) A Pilot RCT of A Body-Oriented Group Therapy For Complex Trauma SurvivorsPerisson DantasNo ratings yet
- Impact of Mindfulness and Self-Compassion On Anxiety and Depression: The Mediating Role of ResilienceDocument10 pagesImpact of Mindfulness and Self-Compassion On Anxiety and Depression: The Mediating Role of ResilienceKevin RomeroNo ratings yet
- Post-Traumatic Stress Disorder: A Guide for Primary Care Clinicians and TherapistsFrom EverandPost-Traumatic Stress Disorder: A Guide for Primary Care Clinicians and TherapistsNo ratings yet
- J CPR 2018 03 004Document64 pagesJ CPR 2018 03 004ayça firatNo ratings yet
- Daftar PustakaDocument37 pagesDaftar PustakaRiska Aulyanti ArisNo ratings yet
- Paliativ Care, IKD3Document9 pagesPaliativ Care, IKD3Agatha NindaNo ratings yet
- Accepted Manuscript: Psychiatry ResearchDocument41 pagesAccepted Manuscript: Psychiatry ResearchEmiNo ratings yet
- Anna Vogel Rita Rosner: Electronic Supplementary MaterialDocument31 pagesAnna Vogel Rita Rosner: Electronic Supplementary MaterialNerea F GNo ratings yet
- Research 1 3.Document31 pagesResearch 1 3.Christine Mae Viñas RemoNo ratings yet
- Eklund Et Al., 2023Document9 pagesEklund Et Al., 2023Administrador ContaNo ratings yet
- Social Anxiety and Fear of Causing Discomfort To Others Diagnostic Specificity Symptom Correlates and CBT Treatment OutcomeDocument19 pagesSocial Anxiety and Fear of Causing Discomfort To Others Diagnostic Specificity Symptom Correlates and CBT Treatment OutcomeAdrián Mantero OjedaNo ratings yet
- Research 1-3Document28 pagesResearch 1-3Christine Mae Viñas RemoNo ratings yet
- Neuroscience and Psychodynamic PsychologyDocument4 pagesNeuroscience and Psychodynamic PsychologyImani ImaniNo ratings yet
- Schizophrenia Research: Rebecca Rodrigues, Kelly K. AndersonDocument10 pagesSchizophrenia Research: Rebecca Rodrigues, Kelly K. Andersonsamira6alvarado6zebaNo ratings yet
- Varios (2019) Sensory Processing Sensitivity in The Context of Environmental Sensitivity - A Critical Review and Development of Research AgendaDocument19 pagesVarios (2019) Sensory Processing Sensitivity in The Context of Environmental Sensitivity - A Critical Review and Development of Research AgendaSusana Plaza-NavasNo ratings yet
- Esketamine For Treatment Resistant Depression: Expert Review of NeurotherapeuticsDocument30 pagesEsketamine For Treatment Resistant Depression: Expert Review of NeurotherapeuticsMahir MutluNo ratings yet
- Bullying As An Expression of Intolerant Schemas: Original ArticleDocument6 pagesBullying As An Expression of Intolerant Schemas: Original ArticleMahir MutluNo ratings yet
- Jom 0b013e3182619038Document9 pagesJom 0b013e3182619038Mahir MutluNo ratings yet
- Gebelerin Algılanan Stres, Hayat Memnuniyeti, PsikolojikDocument40 pagesGebelerin Algılanan Stres, Hayat Memnuniyeti, PsikolojikMahir MutluNo ratings yet
- Child Abuse & Neglect: Juan Faura-Garcia, Izaskun Orue, Esther CalveteDocument11 pagesChild Abuse & Neglect: Juan Faura-Garcia, Izaskun Orue, Esther CalveteMahir MutluNo ratings yet
- Sex Matters: Stress Perception and The Relevance of Resilience and Perceived Social Support in Emerging AdultsDocument9 pagesSex Matters: Stress Perception and The Relevance of Resilience and Perceived Social Support in Emerging AdultsMahir MutluNo ratings yet
- J Jpsychores 2005 12 007Document7 pagesJ Jpsychores 2005 12 007Mahir MutluNo ratings yet
- Seyma BalciDocument90 pagesSeyma BalciMahir MutluNo ratings yet
- Üni̇versi̇te Öğrenci̇leri̇nde Çocukluk ÇağiDocument113 pagesÜni̇versi̇te Öğrenci̇leri̇nde Çocukluk ÇağiMahir MutluNo ratings yet
- Geleneksel Veya Siber Zorbalığa Maruz Kalmanın Okula Yabancılaşmaya İlişkin EtkileriDocument17 pagesGeleneksel Veya Siber Zorbalığa Maruz Kalmanın Okula Yabancılaşmaya İlişkin EtkileriMahir MutluNo ratings yet
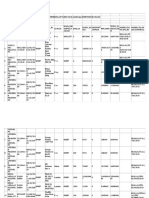
- Implan Dan BMHP NonekatalogDocument284 pagesImplan Dan BMHP NonekatalogmyfaisNo ratings yet
- DR - Masang Sitepu SPM Fak - Kedokteran UhkbpnDocument161 pagesDR - Masang Sitepu SPM Fak - Kedokteran UhkbpnSisca FeronikaNo ratings yet
- BI Miniproject Report (Diabetes)Document18 pagesBI Miniproject Report (Diabetes)Soap MacTavishNo ratings yet
- Prenatal Substance Dependence AbuseDocument13 pagesPrenatal Substance Dependence Abusenursereview100% (2)
- Quick Reference Guide April 2019 PDFDocument2 pagesQuick Reference Guide April 2019 PDFAaron ShokarNo ratings yet
- PE 1 - Module 2 LessonDocument9 pagesPE 1 - Module 2 LessonEllen Joyce P. CarnajeNo ratings yet
- Health Promotion and Health Education - Nursing Students - Perspect PDFDocument120 pagesHealth Promotion and Health Education - Nursing Students - Perspect PDFAlex Olivar100% (1)
- COPDX V2 59 Aug 2019 FINAL2 PDFDocument237 pagesCOPDX V2 59 Aug 2019 FINAL2 PDFjames ryerNo ratings yet
- Infection Control - NclexDocument4 pagesInfection Control - NclexTashaNo ratings yet
- MS4 Midterm NCLEX BurnsDocument5 pagesMS4 Midterm NCLEX BurnsDebbie Dela Cruz100% (5)
- Current Status and Risk Factors of Canine ParvovirusDocument7 pagesCurrent Status and Risk Factors of Canine Parvovirustomas whaterzonNo ratings yet
- Anesthesia Side EffectsDocument10 pagesAnesthesia Side EffectsPADAYON MEDISINANo ratings yet
- Newer Oral Anticoagulants: Dabigatran Etexilate Is An Inactive Pro-DrugDocument5 pagesNewer Oral Anticoagulants: Dabigatran Etexilate Is An Inactive Pro-DrugLouiseNo ratings yet
- Hypoglycemia Guidelines - AAP Vs PES (2172)Document12 pagesHypoglycemia Guidelines - AAP Vs PES (2172)Lina DiazNo ratings yet
- Antibiotic Guidelines For BONE AND JOINT INFECTIONSDocument3 pagesAntibiotic Guidelines For BONE AND JOINT INFECTIONSKhurram NadeemNo ratings yet
- Ouma Winny Attachment ReportDocument35 pagesOuma Winny Attachment ReportFelister John100% (1)
- Esodeviation الحول الإنسيDocument33 pagesEsodeviation الحول الإنسيYaman MuhaisenNo ratings yet
- Microsporum CanisDocument2 pagesMicrosporum CanisMiguel C. DolotNo ratings yet
- IATF Resolution No. 90Document3 pagesIATF Resolution No. 90Steph GNo ratings yet
- Test 6 PharmacologyDocument25 pagesTest 6 Pharmacologysophiebureau102No ratings yet
- Self Assessment ToolDocument25 pagesSelf Assessment ToolJoylyn Mendez LlenaNo ratings yet
- Mindfulness: Presented by Joshua Green, M.S. Doctoral Intern at Umaine Counseling CenterDocument12 pagesMindfulness: Presented by Joshua Green, M.S. Doctoral Intern at Umaine Counseling CenterLawrence MbahNo ratings yet
- Recommendations CardiovascularRenal 07.09.2022Document6 pagesRecommendations CardiovascularRenal 07.09.2022Harisankarthekkethil 26No ratings yet
- Code Team Training and Assessment Best Practices From The Floor UCM - 486059Document34 pagesCode Team Training and Assessment Best Practices From The Floor UCM - 486059JoaoNo ratings yet
- Cerj Sarigumba - Nurse's Progress Notes Fdar TemplateDocument2 pagesCerj Sarigumba - Nurse's Progress Notes Fdar TemplateCerj SarigumbaNo ratings yet
- Assessment of Quality of Movement During A Lateral Step-Down Test Narrative ReviewDocument9 pagesAssessment of Quality of Movement During A Lateral Step-Down Test Narrative ReviewCamila GuevaraNo ratings yet
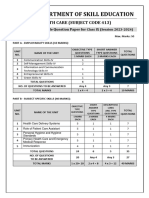
- 413 Health Care SQPDocument7 pages413 Health Care SQPAnil SarohaNo ratings yet
- LupusQol Pour Evaluation de La Qualite de Vie Devilliers 2012 PDFDocument10 pagesLupusQol Pour Evaluation de La Qualite de Vie Devilliers 2012 PDFBamba DiawNo ratings yet
- DMLT I IiDocument11 pagesDMLT I IisyedzahidshabirNo ratings yet