You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- William Bridges Transitions OverviewDocument2 pagesWilliam Bridges Transitions OverviewReveln Consults67% (3)
- M - Medications: Discharge PlanningDocument4 pagesM - Medications: Discharge Planningalynnavictoria100% (4)
- Cystic Tumors of The Pancreas - Diagnosis and TreatmentDocument188 pagesCystic Tumors of The Pancreas - Diagnosis and TreatmentNawzad Sulayvani100% (1)
- XX - 2016-11 - Small Amounts of Tissue Preserve Pancreatic Function - Long-Term Follow-Up Study of Middle-Segment Preserving PancreatectomyDocument8 pagesXX - 2016-11 - Small Amounts of Tissue Preserve Pancreatic Function - Long-Term Follow-Up Study of Middle-Segment Preserving PancreatectomyNawzad SulayvaniNo ratings yet
- Z - 2021-05 - Hemorrhagic Pancreatic Pseudocyst - A Rare ComplicationDocument2 pagesZ - 2021-05 - Hemorrhagic Pancreatic Pseudocyst - A Rare ComplicationNawzad SulayvaniNo ratings yet
- ZZ - 2006-07 - Pancreatic Pseudocyst Bleeding Associated With Massive Intraperitoneal HemorrhageDocument2 pagesZZ - 2006-07 - Pancreatic Pseudocyst Bleeding Associated With Massive Intraperitoneal HemorrhageNawzad SulayvaniNo ratings yet
- 2023-05 - C-Reactive Protein-to-Albumin Ratio Pred - 231002 - 132433Document7 pages2023-05 - C-Reactive Protein-to-Albumin Ratio Pred - 231002 - 132433Nawzad SulayvaniNo ratings yet
- 2020-01 - Endoscopic Retrograde Cholangiopancreatography in Recurrent Acute Pancreatitis - Determining The Optimal Subgroup of Patients in Whom The Procedure Is BeneficialDocument2 pages2020-01 - Endoscopic Retrograde Cholangiopancreatography in Recurrent Acute Pancreatitis - Determining The Optimal Subgroup of Patients in Whom The Procedure Is BeneficialNawzad SulayvaniNo ratings yet
- 2018-10 - Ischemic Cholangiopathy 11 Years After Liver Transplantation From Asymptomatic Chronic Hepatic Artery ThrombosisDocument3 pages2018-10 - Ischemic Cholangiopathy 11 Years After Liver Transplantation From Asymptomatic Chronic Hepatic Artery ThrombosisNawzad SulayvaniNo ratings yet
- 2020-09 - Ischemic Cholangiopathy - An UpdateDocument5 pages2020-09 - Ischemic Cholangiopathy - An UpdateNawzad SulayvaniNo ratings yet
- LP8 With Attached Worksheets - Elements and Compounds Present in Product Labels - FoodDocument11 pagesLP8 With Attached Worksheets - Elements and Compounds Present in Product Labels - FoodAbigail JasminNo ratings yet
- Forcetriad Value Analysis Brief - ValleyLabDocument10 pagesForcetriad Value Analysis Brief - ValleyLabmelquisedecNo ratings yet
- Methodological Issues and Strategies in Clinical RDocument2 pagesMethodological Issues and Strategies in Clinical RAndres CajamarcaNo ratings yet
- Case Presentation Knee Pain PDFDocument16 pagesCase Presentation Knee Pain PDFIchmatul Hidayah OktaveniNo ratings yet
- The Measurement of Emotional Intelligence Using Caliper TraitsDocument4 pagesThe Measurement of Emotional Intelligence Using Caliper TraitsAhmed KamelNo ratings yet
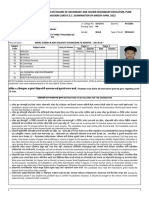
- Maharashtra State Board of Secondary and Higher Secondary Education, Pune Admission Card H.S.C. Examination of March-April 2022Document3 pagesMaharashtra State Board of Secondary and Higher Secondary Education, Pune Admission Card H.S.C. Examination of March-April 2022PANKAJ WANDHARENo ratings yet
- PQS E08-E013 Manufacturer Guide1.4Document23 pagesPQS E08-E013 Manufacturer Guide1.4saberNo ratings yet
- Lesson 2-Technology As A Way of RevealingDocument2 pagesLesson 2-Technology As A Way of RevealingJemalyn Hinggo100% (1)
- Dela Rosa 2A MCN-Module 04Document4 pagesDela Rosa 2A MCN-Module 04Atsu MiyaNo ratings yet
- Thyroid-Stimulating Hormone (TSH) - TSH Levels TestDocument3 pagesThyroid-Stimulating Hormone (TSH) - TSH Levels TestSANDHYASINI NAYAKNo ratings yet
- Benefits of HijamaDocument3 pagesBenefits of HijamaBateria MeaNo ratings yet
- Concept Map Mental HealthDocument2 pagesConcept Map Mental HealthRhina FutrellNo ratings yet
- Kids Screen AdictionDocument3 pagesKids Screen AdictionNisal RukshanNo ratings yet
- 1319 Case StudyDocument7 pages1319 Case StudyElizabeth SamudioNo ratings yet
- ENS 101 Syllabus Fall 2021Document6 pagesENS 101 Syllabus Fall 2021Ho Jin OhNo ratings yet
- Mental Health Problems in College FreshmenDocument28 pagesMental Health Problems in College FreshmenPhillip MendozaNo ratings yet
- Deped Organizational Structure UpdatedDocument30 pagesDeped Organizational Structure UpdatedJoshua Zenox RuizNo ratings yet
- The Ordinance Route Is Bad, Repromulgation Worse: EditorialDocument2 pagesThe Ordinance Route Is Bad, Repromulgation Worse: EditorialVaibhav DafaleNo ratings yet
- Helen Rose Cepeda - Activity 1Document2 pagesHelen Rose Cepeda - Activity 1Helen Rose CepedaNo ratings yet
- Health and Remedies Information Gap Activities - 141815Document6 pagesHealth and Remedies Information Gap Activities - 141815Andrés DíazNo ratings yet
- SafeStayGuidelinesV11 0803022 0Document11 pagesSafeStayGuidelinesV11 0803022 0Bibin RajNo ratings yet
- Types of Ovarian CancerDocument5 pagesTypes of Ovarian Cancerوسام وميض عبدالله CNo ratings yet
- 15 Female: Individual Sports Assignment 1.1 Fitness Assessment, Analysis, & GoalsDocument3 pages15 Female: Individual Sports Assignment 1.1 Fitness Assessment, Analysis, & GoalsClara GreenNo ratings yet
- 1389 FullDocument5 pages1389 FullLuluk hasanahNo ratings yet
- Concept Map f21 FinishedDocument5 pagesConcept Map f21 Finishedapi-601070065No ratings yet
- Massager Pro: User ManualDocument8 pagesMassager Pro: User ManualdiegomattaNo ratings yet
- Family Health Nursing Output: Family Assessment W/ Family Care Plan (With RUBRICS)Document8 pagesFamily Health Nursing Output: Family Assessment W/ Family Care Plan (With RUBRICS)Gia Espinosa Ocbeña100% (1)
- Jacques Lacan - The Mirror Stage As Formative of The I SummaryDocument3 pagesJacques Lacan - The Mirror Stage As Formative of The I SummaryScientist SakthivelNo ratings yet