You might also like
- Female Urinary Tract Infections in Clinical PracticeFrom EverandFemale Urinary Tract Infections in Clinical PracticeBob YangNo ratings yet
- Title An Audit of Microbiological Tests in A Primary Care ClinicDocument20 pagesTitle An Audit of Microbiological Tests in A Primary Care ClinicHam FGNo ratings yet
- Urinary GuidelinesDocument9 pagesUrinary GuidelinesCabinet VeterinarNo ratings yet
- Small Animal - Nephrology and UrologyDocument3 pagesSmall Animal - Nephrology and UrologyNana juniartiNo ratings yet
- New and Developing Diagnostic Technologies For Urinary Tract Infections - PMCDocument25 pagesNew and Developing Diagnostic Technologies For Urinary Tract Infections - PMCPuran pataNo ratings yet
- Antimicrobial Susceptibility Testing PDFDocument19 pagesAntimicrobial Susceptibility Testing PDFdatitoxNo ratings yet
- MICROBIOLOGY LABORATORY COLONY COUNTS AND ANTIMICROBIAL SUSCEPTIBILITYDocument16 pagesMICROBIOLOGY LABORATORY COLONY COUNTS AND ANTIMICROBIAL SUSCEPTIBILITYKaren Urbien Del Valle - CabilloNo ratings yet
- Infeksi Saluran KemihDocument6 pagesInfeksi Saluran KemihGabreilla HanochNo ratings yet
- Antibioticos en Cultivos de OrinaDocument4 pagesAntibioticos en Cultivos de OrinaSofia Huillca GuevaraNo ratings yet
- Laboratory Diagnosis of Urinary Tract Infections in Adult PatientsDocument9 pagesLaboratory Diagnosis of Urinary Tract Infections in Adult PatientsTony ZhangNo ratings yet
- Title: Culture and Sensitivity Pattern of Urinary Tract Infection Among Women of Reproductive Age GroupDocument4 pagesTitle: Culture and Sensitivity Pattern of Urinary Tract Infection Among Women of Reproductive Age GroupFatima MNo ratings yet
- Lab UtiDocument9 pagesLab UtiAni RahayuNo ratings yet
- ATB Gyne PDFDocument10 pagesATB Gyne PDFNATTAPAT SANGKAKULNo ratings yet
- Bacteriuria in Individuals Who Become Delirious: CommentaryDocument3 pagesBacteriuria in Individuals Who Become Delirious: CommentaryGabreilla HanochNo ratings yet
- Antibiotic Susceptibility TestDocument2 pagesAntibiotic Susceptibility TestMaryam SarNo ratings yet
- Atlantic Coast Veterinary Conference 2001 - VINDocument5 pagesAtlantic Coast Veterinary Conference 2001 - VINYahya ElemmawyNo ratings yet
- UTIDocument17 pagesUTIBongkotchakorn Mind PhonchaiNo ratings yet
- 39 BF 07 FB 9 Ef 58 FDFDocument6 pages39 BF 07 FB 9 Ef 58 FDFMazin AlmaziniNo ratings yet
- Laboratory Diagnosis of Urinary Tract InfectionsDocument9 pagesLaboratory Diagnosis of Urinary Tract InfectionsArturo OrtúñezNo ratings yet
- Culture - Urine: BackgroundDocument4 pagesCulture - Urine: BackgroundYeyen SaputriNo ratings yet
- Prevention of Urinary Tract Infection in Six Spinal Cord Injured Pregnant Women Who Gave Birth To Seven Children Under A Weekly Oral Cyclic Antibiotic Program PDFDocument4 pagesPrevention of Urinary Tract Infection in Six Spinal Cord Injured Pregnant Women Who Gave Birth To Seven Children Under A Weekly Oral Cyclic Antibiotic Program PDFMaría Alejandra López AriasNo ratings yet
- Uti 2011Document7 pagesUti 2011Kamolporn JongchanapongNo ratings yet
- Laboratory Diagnosis of Urinary Tract Infections in Adult PatientsDocument9 pagesLaboratory Diagnosis of Urinary Tract Infections in Adult PatientsAngga Krisna ArthaNo ratings yet
- Management of Urinary Tract Infection in Women A Practical Approach For Everyday PracticeDocument23 pagesManagement of Urinary Tract Infection in Women A Practical Approach For Everyday PracticeKeysha AbigailNo ratings yet
- Urinalysis (Ua) and The Diagnosis of UtisDocument5 pagesUrinalysis (Ua) and The Diagnosis of UtisErawati ArmayaniNo ratings yet
- 43 Pukar EtalDocument3 pages43 Pukar EtaleditorijmrhsNo ratings yet
- Document 4Document9 pagesDocument 4นันทสิทธิ์ ศิริวิชญ์ไมตรีNo ratings yet
- Prevalence and Antimicrobial Resistance Profile of Pathogens Isolated From Patients With Urine Tract Infections Admitted To A University Hospital in A Medium-Sized Brazilian CityDocument11 pagesPrevalence and Antimicrobial Resistance Profile of Pathogens Isolated From Patients With Urine Tract Infections Admitted To A University Hospital in A Medium-Sized Brazilian CityAna LemesNo ratings yet
- Clin Infect Dis.-2010-Fishbain-79-84Document6 pagesClin Infect Dis.-2010-Fishbain-79-84Edson MarquesNo ratings yet
- ATB ProfilaxisDocument10 pagesATB Profilaxiscristopher_ahcNo ratings yet
- Principles of Bacterial Infections and Anti-Infectives: Cause, Pathogenicity, and VirulenceDocument29 pagesPrinciples of Bacterial Infections and Anti-Infectives: Cause, Pathogenicity, and Virulencejheannie02100% (1)
- Name: Kiran Bhatti University: Liaquat University of Medical and Health Sciences. Pharm-D StudentDocument9 pagesName: Kiran Bhatti University: Liaquat University of Medical and Health Sciences. Pharm-D StudentPharmanic By Ruttaba FatimaNo ratings yet
- Lower Urinary Tract Infection GuideDocument4 pagesLower Urinary Tract Infection GuideReen ChavezNo ratings yet
- qfrUTI EditDocument9 pagesqfrUTI EditMylz MendozaNo ratings yet
- qfrUTI EditDocument9 pagesqfrUTI EditMylz MendozaNo ratings yet
- AUP Medical Lab Science Dept Case Study Analysis BacteriologyDocument1 pageAUP Medical Lab Science Dept Case Study Analysis BacteriologyEDDREI PAULLYNNE DESOASIDONo ratings yet
- Antibiotic Resistance Thesis StatementDocument6 pagesAntibiotic Resistance Thesis Statementkatelogebellevue100% (2)
- Nonantibiotic Prevention andDocument27 pagesNonantibiotic Prevention andGheorghe SecuNo ratings yet
- Updated Guideline On Diagnosis and TreatmentDocument5 pagesUpdated Guideline On Diagnosis and TreatmentRidho WahyutomoNo ratings yet
- Iaat 12 I 9 P 187Document8 pagesIaat 12 I 9 P 187Maniak LuckNo ratings yet
- Iaat12i5p615 PDFDocument6 pagesIaat12i5p615 PDFsuresh kumar bakhtianiNo ratings yet
- JM 002169Document4 pagesJM 002169edisonballaNo ratings yet
- Rational Use and Prevention of Antibiotic ResistanceDocument22 pagesRational Use and Prevention of Antibiotic ResistanceMD ASIFNo ratings yet
- Principles of Antibiotic TherapyDocument26 pagesPrinciples of Antibiotic TherapyHaroun drissNo ratings yet
- Treatment and Future of Bacterial Urinary Tract InfectionsDocument10 pagesTreatment and Future of Bacterial Urinary Tract InfectionsAgrippina KatarinaNo ratings yet
- Treatment of Bacterial Urinary Tract InfDocument10 pagesTreatment of Bacterial Urinary Tract InfAnugrah TrianandaNo ratings yet
- Isolation, Identification and Characterization of Urinary Tract Infectious Bacteria and The Effect of Different AntibioticsDocument10 pagesIsolation, Identification and Characterization of Urinary Tract Infectious Bacteria and The Effect of Different AntibioticsAlexander DeckerNo ratings yet
- International Journal of Pharmacy and Pharmaceutical SciencesDocument6 pagesInternational Journal of Pharmacy and Pharmaceutical SciencesNurainiManda-MinozNo ratings yet
- Clinical Therapy of UTI in Children Under The Age of Five Varies WidelyDocument21 pagesClinical Therapy of UTI in Children Under The Age of Five Varies WidelyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Guide To Clinical Audit Antibiotic Use in Urinary Tract InfectionDocument10 pagesGuide To Clinical Audit Antibiotic Use in Urinary Tract Infectionihtisham1No ratings yet
- Treatment of Bacterial Urinary Tract Inf20160406 20379 J6wa49 With Cover Page v2Document11 pagesTreatment of Bacterial Urinary Tract Inf20160406 20379 J6wa49 With Cover Page v2Babita AgrawalNo ratings yet
- Diagnosing Inflammation and Infection in The Urinary System Via ProteomicsDocument14 pagesDiagnosing Inflammation and Infection in The Urinary System Via ProteomicsYUSHANo ratings yet
- Bacteriological Profile of Blood Stream Infections at A Rural Tertiary Care Teaching Hospital of Western Uttar PradeshDocument9 pagesBacteriological Profile of Blood Stream Infections at A Rural Tertiary Care Teaching Hospital of Western Uttar PradeshHArdik NegiNo ratings yet
- Rational Use of AntibioticsDocument39 pagesRational Use of Antibioticsjun sianNo ratings yet
- I. Urinary Tract Infections Overview: A. Acute Uncomplicated UTI in WomenDocument13 pagesI. Urinary Tract Infections Overview: A. Acute Uncomplicated UTI in WomenDominique VioletaNo ratings yet
- 878Wag2015MS Urosepsis OverviewDocument20 pages878Wag2015MS Urosepsis OverviewMuhammad Imam NoorNo ratings yet
- 11 - Recurrent UTI TOG 2020Document7 pages11 - Recurrent UTI TOG 2020Anna JuniedNo ratings yet
- Guideline Antibiotic RationalDocument35 pagesGuideline Antibiotic RationalIstianah EsNo ratings yet
- Key definitions and antibiotic choices for UTIs in pregnancyDocument6 pagesKey definitions and antibiotic choices for UTIs in pregnancyVijetaNo ratings yet
- UTI and Asymptomatic Bacteriuria TEACHING SLIDESDocument43 pagesUTI and Asymptomatic Bacteriuria TEACHING SLIDESJana DbaibouNo ratings yet
- Actinocyclusnormanii 1990Document14 pagesActinocyclusnormanii 1990Cris FischerNo ratings yet
- 1 s2.0 S0264817213002675 MainDocument21 pages1 s2.0 S0264817213002675 MainCris FischerNo ratings yet
- Lima 2013Document12 pagesLima 2013Cris FischerNo ratings yet
- 1 s2.0 S0031018219302640 MainDocument17 pages1 s2.0 S0031018219302640 MainCris FischerNo ratings yet
- 1 s2.0 S0034425710003469 MainDocument9 pages1 s2.0 S0034425710003469 MainCris FischerNo ratings yet
- 1 s2.0 S0037073820301974 MainDocument11 pages1 s2.0 S0037073820301974 MainCris FischerNo ratings yet
- 10 1016@j Earscirev 2019 103000Document63 pages10 1016@j Earscirev 2019 103000Cris FischerNo ratings yet
- Hassan2018 Cyclotella MeneghinianaDocument16 pagesHassan2018 Cyclotella MeneghinianaCris FischerNo ratings yet
- 1552 FullDocument1 page1552 FullCris FischerNo ratings yet
- Journal Pre-Proof: Clinical Microbiology and InfectionDocument25 pagesJournal Pre-Proof: Clinical Microbiology and InfectionCris FischerNo ratings yet
- Effect of Light and Sediment Grain Size On The Vertical Migration of Benthic DiatomsDocument8 pagesEffect of Light and Sediment Grain Size On The Vertical Migration of Benthic DiatomsCris FischerNo ratings yet
- Yahaf 2021Document4 pagesYahaf 2021Cris FischerNo ratings yet
- Cretaceous DiatomsDocument27 pagesCretaceous DiatomsCris FischerNo ratings yet
- Toledo MIS SOUTH ATLANTICDocument13 pagesToledo MIS SOUTH ATLANTICCris FischerNo ratings yet
- Himanshu Rai, Roshni Khare, Dalip Kumar Upreti (auth.), Himanshu Rai, Dalip K. Upreti (eds.) - Terricolous Lichens in India_ Volume 1_ Diversity Patterns and Distribution Ecology (2014, Springer-Verlag New York) -Document104 pagesHimanshu Rai, Roshni Khare, Dalip Kumar Upreti (auth.), Himanshu Rai, Dalip K. Upreti (eds.) - Terricolous Lichens in India_ Volume 1_ Diversity Patterns and Distribution Ecology (2014, Springer-Verlag New York) -Cris FischerNo ratings yet
- Biodeterioration of Stone SurfacesDocument299 pagesBiodeterioration of Stone SurfacesCris FischerNo ratings yet
- Particle Size Measurement of Diatoms With Inference of Their Properties: Comparison of Three TechniquesDocument11 pagesParticle Size Measurement of Diatoms With Inference of Their Properties: Comparison of Three TechniquesCris FischerNo ratings yet
- Trevor Goward - The Lichens of British Columbia, Illustrated Keys, Part 2 - Fruticose Species (1999, BC Ministry of Forests)Document326 pagesTrevor Goward - The Lichens of British Columbia, Illustrated Keys, Part 2 - Fruticose Species (1999, BC Ministry of Forests)Cris FischerNo ratings yet
- Marine Isotope Stage 3 (MIS 3) and Continental Beds From Northern Uruguay (Sopas Formation) : Paleontology, Chronology, and ClimateDocument23 pagesMarine Isotope Stage 3 (MIS 3) and Continental Beds From Northern Uruguay (Sopas Formation) : Paleontology, Chronology, and ClimateCris FischerNo ratings yet
- Rosaetal 2017Document26 pagesRosaetal 2017Cris FischerNo ratings yet
- Mahi QuesDocument10 pagesMahi QuesCris FischerNo ratings yet
- Medeanicetal 2009Document11 pagesMedeanicetal 2009Cris FischerNo ratings yet
- Campbell Et Al Manuscript EscholarDocument37 pagesCampbell Et Al Manuscript EscholarCris FischerNo ratings yet
- Structure and Diversity of Intertidal Benthic Diatom Assemblages in Contrasting Shores: A Case Study From The Tagus EstuaryDocument13 pagesStructure and Diversity of Intertidal Benthic Diatom Assemblages in Contrasting Shores: A Case Study From The Tagus EstuaryCris FischerNo ratings yet
- 238655Document1 page238655Cris FischerNo ratings yet
- Wang 2019Document35 pagesWang 2019Cris FischerNo ratings yet
- Drainage Manual: State of Florida Department of TransportationDocument78 pagesDrainage Manual: State of Florida Department of TransportationghoyarbideNo ratings yet
- (Leon 2021) Pengaruh Financial Distress, Laverage Terhadap Konservatisme Akuntansi Pada Perusahaan Manfaktur Sektor Konsumsi 2016-2019Document24 pages(Leon 2021) Pengaruh Financial Distress, Laverage Terhadap Konservatisme Akuntansi Pada Perusahaan Manfaktur Sektor Konsumsi 2016-2019PUTRI AYU HASTUTINo ratings yet
- Floor CraneDocument6 pagesFloor CranejillianixNo ratings yet
- Science, Technology, Engineering and Mathematics (Stem) Grade 11 Grade 12 First Semester Second Semester First Semester Second SemesterDocument1 pageScience, Technology, Engineering and Mathematics (Stem) Grade 11 Grade 12 First Semester Second Semester First Semester Second SemesterJhondriel Lim71% (7)
- Ms. Rochelle P. Sulitas – Grade 7 SCIENCE Earth and Space Learning PlanDocument4 pagesMs. Rochelle P. Sulitas – Grade 7 SCIENCE Earth and Space Learning PlanEmelynNo ratings yet
- Tem 2final PDFDocument9 pagesTem 2final PDFSkuukzky baeNo ratings yet
- Epoxy HRDocument5 pagesEpoxy HRMuthuKumarNo ratings yet
- NasaDocument26 pagesNasaMatei BuneaNo ratings yet
- Book Notes - The Life Changing Magic of Tidying Up PDFDocument6 pagesBook Notes - The Life Changing Magic of Tidying Up PDFAilyn Bagares AñanoNo ratings yet
- Workbook. Unit 3. Exercises 5 To 9. RESPUESTASDocument3 pagesWorkbook. Unit 3. Exercises 5 To 9. RESPUESTASRosani GeraldoNo ratings yet
- 2024 Yoga Vidya Training FormDocument8 pages2024 Yoga Vidya Training FormJohnNo ratings yet
- Samsung (UH5003-SEA) BN68-06750E-01ENG-0812Document2 pagesSamsung (UH5003-SEA) BN68-06750E-01ENG-0812asohas77No ratings yet
- TaxonomyDocument56 pagesTaxonomyKrezia Mae SolomonNo ratings yet
- Robotics: Let's Talk About Robots!Document5 pagesRobotics: Let's Talk About Robots!Elizaveta KononovaNo ratings yet
- Enzyme KineticsDocument13 pagesEnzyme KineticsMohib100% (1)
- SDRRM Earthquake Drill TemplateDocument3 pagesSDRRM Earthquake Drill TemplateChristian Bonne MarimlaNo ratings yet
- Portable USB ChargerDocument13 pagesPortable USB ChargerParmar KundanNo ratings yet
- ASTM D5895 - 2020 Tiempo SecadoDocument4 pagesASTM D5895 - 2020 Tiempo SecadoPablo OrtegaNo ratings yet
- GC 1999 03 Minas BrethilDocument5 pagesGC 1999 03 Minas BrethilErszebethNo ratings yet
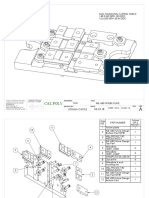
- Fixture Design ProjectDocument4 pagesFixture Design ProjectJosh CastleNo ratings yet
- DriveDebug User ManualDocument80 pagesDriveDebug User ManualFan CharlesNo ratings yet
- Teaching English as a Second Language in Four PhasesDocument18 pagesTeaching English as a Second Language in Four PhasesVia Johnson100% (1)
- CENELEC RA STANDARDS CATALOGUEDocument17 pagesCENELEC RA STANDARDS CATALOGUEHamed AhmadnejadNo ratings yet
- Cse 3003: Computer Networks: Dr. Sanket Mishra ScopeDocument56 pagesCse 3003: Computer Networks: Dr. Sanket Mishra ScopePOTNURU RAM SAINo ratings yet
- Concrete Mixer Truck SinotrukDocument2 pagesConcrete Mixer Truck SinotrukTiago AlvesNo ratings yet
- Decision Flow Chart: For Suspicious PackagesDocument2 pagesDecision Flow Chart: For Suspicious PackagesHervian LanangNo ratings yet
- All About Bearing and Lubrication A Complete GuideDocument20 pagesAll About Bearing and Lubrication A Complete GuideJitu JenaNo ratings yet
- IEEE802.11b/g High Power Wireless AP/Bridge Quick Start GuideDocument59 pagesIEEE802.11b/g High Power Wireless AP/Bridge Quick Start GuideonehotminuteNo ratings yet
- Automation & Artificial Intelligence: Robots and Their ApplicationsDocument93 pagesAutomation & Artificial Intelligence: Robots and Their ApplicationsManal AndhereNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (14)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Daniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisFrom EverandDaniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisRating: 3.5 out of 5 stars3.5/5 (130)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)