You might also like
- Is Frenotomy Effective in ImprovingDocument8 pagesIs Frenotomy Effective in ImprovingIkaDian PuspitanzaNo ratings yet
- Benefits of Frenulotomy in Infants With AnkyloglossiaDocument4 pagesBenefits of Frenulotomy in Infants With Ankyloglossiaadrian bouzasNo ratings yet
- Labial Frenotomy For Symptomatic Isolated Upper Lip TieDocument5 pagesLabial Frenotomy For Symptomatic Isolated Upper Lip Tiepj.czarneckaNo ratings yet
- International Journal of Pediatric Otorhinolaryngology: Mark W. Steehler, Matthew K. Steehler, Earl H. HarleyDocument5 pagesInternational Journal of Pediatric Otorhinolaryngology: Mark W. Steehler, Matthew K. Steehler, Earl H. HarleyJohan Sebastian Perea PalaciosNo ratings yet
- A Case Series of Anterior and Posterior Tongue TiesDocument4 pagesA Case Series of Anterior and Posterior Tongue TiesTrung Sơn LêNo ratings yet
- DownloadDocument11 pagesDownloadhasan nazzalNo ratings yet
- Abdominal Wall Defects Exomphalos (Omphalocele)Document5 pagesAbdominal Wall Defects Exomphalos (Omphalocele)Ahmad Ulil AlbabNo ratings yet
- Tongue Tie 2016Document6 pagesTongue Tie 2016drchiNo ratings yet
- Neonatal Research PaperDocument5 pagesNeonatal Research Paperkrqovxbnd100% (1)
- Nursing Research PaperDocument14 pagesNursing Research Paperapi-735739064No ratings yet
- Neonatal Brachial Plexus PalsyFrom EverandNeonatal Brachial Plexus PalsyRating: 5 out of 5 stars5/5 (1)
- Ankyloglossia: Assessment, Incidence, and Effect of Frenuloplasty On The Breastfeeding DyadDocument8 pagesAnkyloglossia: Assessment, Incidence, and Effect of Frenuloplasty On The Breastfeeding DyadBárbara ArancibiaNo ratings yet
- Nursing Care of Preterm InfantsDocument13 pagesNursing Care of Preterm Infants3B NOVIDA, ALEYA G.No ratings yet
- Educational Topic 14: Lactation: U 2: O S A: N ODocument3 pagesEducational Topic 14: Lactation: U 2: O S A: N Ofasdf asdaNo ratings yet
- Breastfeeding Improvement Following Tonguetie and Liptie Release A Prospective Cohort StudyDocument7 pagesBreastfeeding Improvement Following Tonguetie and Liptie Release A Prospective Cohort Studywegrimel ariegaraNo ratings yet
- Ectopic Pregnancy Research PapersDocument6 pagesEctopic Pregnancy Research Papersafedthktn100% (1)
- Obgyn Clerkship Guide To SuccessDocument6 pagesObgyn Clerkship Guide To SuccessprabhatNo ratings yet
- Tongue Tieassessandmanage2020 PDFDocument8 pagesTongue Tieassessandmanage2020 PDFTwinamasiko DanielNo ratings yet
- Fetal Neural Tube 2021 12 LMBR PDFDocument24 pagesFetal Neural Tube 2021 12 LMBR PDFwayansiagaNo ratings yet
- Cleft Lip and Cleft PalateDocument11 pagesCleft Lip and Cleft PalateErnie AlixNo ratings yet
- Clinical Review: Prevalence, Diagnosis, and Treatment of AnkyloglossiaDocument7 pagesClinical Review: Prevalence, Diagnosis, and Treatment of AnkyloglossiaisnaftyaNo ratings yet
- Di Article ReviewDocument10 pagesDi Article Reviewapi-238540303No ratings yet
- History of Present IllnessDocument30 pagesHistory of Present IllnessTrixia Joy R NachorNo ratings yet
- Endocrinología pediátrica práctica en poblaciones con recursos limitadosFrom EverandEndocrinología pediátrica práctica en poblaciones con recursos limitadosNo ratings yet
- Research Paper On Pregnancy and ChildbirthDocument8 pagesResearch Paper On Pregnancy and Childbirthnywxluvkg100% (1)
- Literature Review On Pregnancy Labour and PuerperiumDocument4 pagesLiterature Review On Pregnancy Labour and Puerperiumfihynakalej2No ratings yet
- HospitalizationDocument5 pagesHospitalizationDaniela Aguirre GonzálezNo ratings yet
- BGD Tutorial 2015 - Applied Embryology and TeratologyDocument10 pagesBGD Tutorial 2015 - Applied Embryology and TeratologyRendy YogaNo ratings yet
- 15.3 Cleft Lip and PalateDocument41 pages15.3 Cleft Lip and PalateChristina YounasNo ratings yet
- Management of Posterior Ankyloglossia and Upper Lip Ties in A Tertiary Otolaryngology Outpatient ClinicDocument4 pagesManagement of Posterior Ankyloglossia and Upper Lip Ties in A Tertiary Otolaryngology Outpatient Clinicadrian bouzasNo ratings yet
- POLYMELIADocument17 pagesPOLYMELIAJanani SelvakumarNo ratings yet
- Literature Review On Knowledge and Practice of Exclusive BreastfeedingDocument5 pagesLiterature Review On Knowledge and Practice of Exclusive Breastfeedingc5rh6ras100% (1)
- Care of the Well NewbornDocument10 pagesCare of the Well NewbornAntonio ValleNo ratings yet
- v13 p74 EthicalDocument7 pagesv13 p74 EthicalVincent FloraNo ratings yet
- Breastfeeding Dissertation TopicsDocument8 pagesBreastfeeding Dissertation TopicsBuyACollegePaperOnlineMilwaukee100% (1)
- Clinical Approach of Ankyloglossia in Babies: Report of Two CasesDocument6 pagesClinical Approach of Ankyloglossia in Babies: Report of Two CasesEstaf EmkeyzNo ratings yet
- 05 N310 16324Document14 pages05 N310 16324Wanda WoodNo ratings yet
- Guidelines for managing abnormally invasive placentaDocument16 pagesGuidelines for managing abnormally invasive placentaErika GuerreroNo ratings yet
- Breech Presentation Literature ReviewDocument6 pagesBreech Presentation Literature Reviewfrvkuhrif100% (1)
- Pediatrics in Review 2006 Sugar 213 23Document13 pagesPediatrics in Review 2006 Sugar 213 23Berry BancinNo ratings yet
- Literature Review On Knowledge of Exclusive BreastfeedingDocument7 pagesLiterature Review On Knowledge of Exclusive BreastfeedingaflruomdeNo ratings yet
- Developmental Care For Promoting Development and Preventing Morbidity in Preterm Infants (Review)Document51 pagesDevelopmental Care For Promoting Development and Preventing Morbidity in Preterm Infants (Review)Dwi Suci AsrianiNo ratings yet
- Apoyo A Diada - Guia para SLPDocument11 pagesApoyo A Diada - Guia para SLPPaula Belén Rojas CunazzaNo ratings yet
- Relevant Obstetric Factors Associated With Fetal Heart Rate Monitoring For Cerebral Palsy in Pregnant Women With Hypertensive Disorder of PregnancyDocument8 pagesRelevant Obstetric Factors Associated With Fetal Heart Rate Monitoring For Cerebral Palsy in Pregnant Women With Hypertensive Disorder of PregnancyDwi PurwantiNo ratings yet
- HO 4 Essential Intrapartum Care 6may2013Document12 pagesHO 4 Essential Intrapartum Care 6may2013Maedine Urbano-Briones100% (1)
- Ebj JalesDocument3 pagesEbj JalesNEIL GUTIERREZNo ratings yet
- Breastfeeding Awareness and Practices in AbakalikiDocument14 pagesBreastfeeding Awareness and Practices in AbakalikiBusiness ProposalNo ratings yet
- Malnutrition During Pregnancy Among Child BearingDocument6 pagesMalnutrition During Pregnancy Among Child BearingR&T FamilyNo ratings yet
- Research Paper Neonatal NursingDocument4 pagesResearch Paper Neonatal Nursinggz8xbnex100% (1)
- Thesis On BreastfeedingDocument4 pagesThesis On Breastfeedingppxohvhkd100% (2)
- Research Paper On Exclusive BreastfeedingDocument8 pagesResearch Paper On Exclusive Breastfeedingmadywedykul2100% (1)
- Human Milk: Composition, Clinical Benefits and Future Opportunities: 90th Nestlé Nutrition Institute Workshop, Lausanne, October-November 2017From EverandHuman Milk: Composition, Clinical Benefits and Future Opportunities: 90th Nestlé Nutrition Institute Workshop, Lausanne, October-November 2017No ratings yet
- Multiple Gestation PPTDocument22 pagesMultiple Gestation PPTIrish Ivy VibethNo ratings yet
- Multiple GestationDocument22 pagesMultiple GestationIrish Ivy VibethNo ratings yet
- Running Head: FRENECTOMIES 1Document9 pagesRunning Head: FRENECTOMIES 1api-522555065No ratings yet
- GER-GERD - To D or Not To D Lightdale WebinarDocument81 pagesGER-GERD - To D or Not To D Lightdale WebinarIna PoianaNo ratings yet
- Research Paper On Ob GynDocument6 pagesResearch Paper On Ob Gynmwjhkmrif100% (1)
- Solutio Plasenta JournalDocument7 pagesSolutio Plasenta JournalAndi NatalonnaNo ratings yet
- Infant Feeding Beliefs and Day-to-Day Feeding Practices of NICU NursesDocument8 pagesInfant Feeding Beliefs and Day-to-Day Feeding Practices of NICU NursesFarah PramestyNo ratings yet
- Tongue-Tie: Incidence and Outcomes in Breastfeeding After Lingual Frenotomy in 2333 NewbornsDocument7 pagesTongue-Tie: Incidence and Outcomes in Breastfeeding After Lingual Frenotomy in 2333 NewbornsMarco Saavedra BurgosNo ratings yet
- Lesson 16Document20 pagesLesson 16Twinamasiko DanielNo ratings yet
- Histopathology of Dentinal Caries PresentationDocument31 pagesHistopathology of Dentinal Caries PresentationTwinamasiko DanielNo ratings yet
- Tongue Tieassessandmanage2020 PDFDocument8 pagesTongue Tieassessandmanage2020 PDFTwinamasiko DanielNo ratings yet
- Dental CariesDocument5 pagesDental CariesTwinamasiko DanielNo ratings yet
- Dental Caries Classification PDFDocument5 pagesDental Caries Classification PDFTwinamasiko DanielNo ratings yet
- General Tonic Monograph and Pharmacology Shi Quan Da Bu WanDocument8 pagesGeneral Tonic Monograph and Pharmacology Shi Quan Da Bu WanrikiNo ratings yet
- River BlindnessDocument3 pagesRiver BlindnessIlma Latansa100% (1)
- JAJ TestimoniesDocument2 pagesJAJ TestimoniesErdem Ğ. ÇalışkanNo ratings yet
- Acute Myeloid LeukemiaDocument14 pagesAcute Myeloid Leukemiaapi-247402827No ratings yet
- Nephrolithiasis - Drug StudyDocument5 pagesNephrolithiasis - Drug StudyAia JavierNo ratings yet
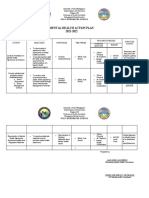
- Mental Health Action PlanDocument2 pagesMental Health Action PlanKenny Ann Grace Batiancila100% (9)
- GRADE 8 Teaching Guide Catchup Bullying and Its Impact On Mental Health Health 8Document6 pagesGRADE 8 Teaching Guide Catchup Bullying and Its Impact On Mental Health Health 8iamtherealjuandelacruzNo ratings yet
- Occupational Health and Safety Issues of Traffic EnforcersDocument16 pagesOccupational Health and Safety Issues of Traffic EnforcersRhobin Mhark GabitoNo ratings yet
- Maternal Child NursingDocument31 pagesMaternal Child Nursingmatrixtrinity88% (24)
- The FGM Initiative Final Report 2013Document61 pagesThe FGM Initiative Final Report 2013TinaStiffNo ratings yet
- NCLEX-RN Test Plan 2010Document10 pagesNCLEX-RN Test Plan 2010PhilippineNursingDirectory.com100% (1)
- Books by Robie H. HarrisDocument2 pagesBooks by Robie H. HarrisCandlewick PressNo ratings yet
- Examination Performance Report Spring 2018 Part 1Document3 pagesExamination Performance Report Spring 2018 Part 1Syed Danish AliNo ratings yet
- P2C Syllabus v6Document18 pagesP2C Syllabus v6Sabin CoteliciNo ratings yet
- EJMHR Ezunu Et Al V1Document10 pagesEJMHR Ezunu Et Al V1ngoziestherezunu74No ratings yet
- Flowchart For Drug Surrender: Pnp/PdeaDocument2 pagesFlowchart For Drug Surrender: Pnp/PdeaLuppo PcaduNo ratings yet
- Reading Test (4) - Part (C) - Text (1) - Smart OEDocument1 pageReading Test (4) - Part (C) - Text (1) - Smart OEdrnilarwinNo ratings yet
- Reading Unit 3Document2 pagesReading Unit 3estefania aranda jimenezNo ratings yet
- Victoria DePonceau SPD ResumeDocument1 pageVictoria DePonceau SPD ResumeVictoria Leigh DePonceauNo ratings yet
- How Environment Affects Our HealthDocument4 pagesHow Environment Affects Our HealthMajo PerezNo ratings yet
- New Harbinger Self-Help Workbook the Mindfulness and Acceptance Workbook for Social Anxiety and Shyness_ Using Acceptance and Commitment Therapy to Free Yourself From Fear and Reclaim Your Life [1st Ed.Document132 pagesNew Harbinger Self-Help Workbook the Mindfulness and Acceptance Workbook for Social Anxiety and Shyness_ Using Acceptance and Commitment Therapy to Free Yourself From Fear and Reclaim Your Life [1st Ed.Wesley Ramalho100% (1)
- NYCOSH Letter To DOB Re: OSHA Card Arrests 10262015Document2 pagesNYCOSH Letter To DOB Re: OSHA Card Arrests 10262015Monica NovoaNo ratings yet
- Mapeh 6 Test Questions From Q1-Q4Document8 pagesMapeh 6 Test Questions From Q1-Q4Tino SalabsabNo ratings yet
- Bactomin Product MonographDocument43 pagesBactomin Product MonographVivek AlaiNo ratings yet
- Nephrotic SyndromeDocument23 pagesNephrotic SyndromeDivina Francia JovenNo ratings yet
- Stress Management Strategies: Individual Approaches Organizational ApproachesDocument13 pagesStress Management Strategies: Individual Approaches Organizational ApproachesYakshit GoelNo ratings yet
- BS BuzzDocument9 pagesBS BuzzBS Central, Inc. "The Buzz"No ratings yet
- CV Template2Document3 pagesCV Template2rosemaryNo ratings yet
- Complication of Hemodialysis and Their ManagementDocument52 pagesComplication of Hemodialysis and Their ManagementRetno SumaraNo ratings yet
- CPG Gestational Trophoblastic DiseasesDocument31 pagesCPG Gestational Trophoblastic DiseasesSMR50% (2)