You might also like
- Current Therapy in EndodonticsFrom EverandCurrent Therapy in EndodonticsPriyanka JainNo ratings yet
- Von Wilmowsky2020 Use of CAD-based Pre-Bent Implants Reduces Theatre Time in Orbital Floor ReconstructionDocument6 pagesVon Wilmowsky2020 Use of CAD-based Pre-Bent Implants Reduces Theatre Time in Orbital Floor ReconstructionquetmauhamNo ratings yet
- Rahim Ov 2011Document11 pagesRahim Ov 2011Muslikah IkaNo ratings yet
- Clinical Application of 3D Pre-Bent Titanium Implants For Orbital Floor FracturesDocument6 pagesClinical Application of 3D Pre-Bent Titanium Implants For Orbital Floor Fractureslowjy119411No ratings yet
- Precision and Accuracy of A Digital Impression Scanner in Full-Arch Implant RehabilitationDocument5 pagesPrecision and Accuracy of A Digital Impression Scanner in Full-Arch Implant Rehabilitationgeorgios031No ratings yet
- Cloi 2022 GehrkeDocument15 pagesCloi 2022 GehrkeMarioNo ratings yet
- Prosthetic Management of An Existing Transmandibular Implant: A Clinical ReportDocument5 pagesProsthetic Management of An Existing Transmandibular Implant: A Clinical ReportDragos CiongaruNo ratings yet
- A Literature Review: CBCT Applications in Dental PracticeDocument6 pagesA Literature Review: CBCT Applications in Dental PracticeMohanad BraziNo ratings yet
- The Evolution of The CEREC SystemDocument7 pagesThe Evolution of The CEREC Systemjinny1_0No ratings yet
- Fatigue Resistance of Ultrathin CAD:CAM Complete Crowns With A Simplified Cementation Process.Document6 pagesFatigue Resistance of Ultrathin CAD:CAM Complete Crowns With A Simplified Cementation Process.Ali QawasNo ratings yet
- 2011 FIRMIN Autologous Ear ReconstructionDocument8 pages2011 FIRMIN Autologous Ear ReconstructionDimitris RodriguezNo ratings yet
- Dimensional Accuracy of Impression Tec-Hniques For The Endosteal Implants (An in Vitro Study) : Part IDocument12 pagesDimensional Accuracy of Impression Tec-Hniques For The Endosteal Implants (An in Vitro Study) : Part IAnonymous l0nej5M5sLNo ratings yet
- The 3d-Printed Prototype A New Protocol For The Evaluation and Potential Adaptation of Monolithic All-Ceramic Restorations Before FinalizationDocument8 pagesThe 3d-Printed Prototype A New Protocol For The Evaluation and Potential Adaptation of Monolithic All-Ceramic Restorations Before Finalizationfloressam2000No ratings yet
- Neves 2012Document7 pagesNeves 2012Manuel Humberto Rojas ArcaNo ratings yet
- Ing. Serag M. A Comparative Study of The Accuracy of Dies Made From Digital IntraDocument6 pagesIng. Serag M. A Comparative Study of The Accuracy of Dies Made From Digital IntraBavilonia K PaolaNo ratings yet
- 10 1016@j Prosdent 2020 04 025Document5 pages10 1016@j Prosdent 2020 04 025praveen rajNo ratings yet
- Journal of Dental Problems and SolutionsDocument4 pagesJournal of Dental Problems and SolutionsPeertechz Publications Inc.No ratings yet
- Acetabular Impaction Grafting in Total Hip Replacement 2011Document11 pagesAcetabular Impaction Grafting in Total Hip Replacement 2011abass elananiNo ratings yet
- 1 s2.0 S0022391323007655 MainDocument6 pages1 s2.0 S0022391323007655 MainDANTE DELEGUERYNo ratings yet
- RSGDocument5 pagesRSGHugoMoralesTecnicoDentalNo ratings yet
- Theuseofpatient-Specific Implantsinoraland MaxillofacialsurgeryDocument8 pagesTheuseofpatient-Specific Implantsinoraland MaxillofacialsurgeryUmer HussainNo ratings yet
- Art 2Document6 pagesArt 2ROSVITA EUFEMIA SANCHEZ VALENZUELANo ratings yet
- Evaluation of Marginal and Internal Fit of Ceramic and Metallic Crown Copings Using X-Ray Microtomography TechnologyDocument6 pagesEvaluation of Marginal and Internal Fit of Ceramic and Metallic Crown Copings Using X-Ray Microtomography TechnologyMayra Ortiz HerreraNo ratings yet
- In Situ Fibre Fracture Measurement in Carbon-Epoxy Laminates Using HighDocument7 pagesIn Situ Fibre Fracture Measurement in Carbon-Epoxy Laminates Using Highjianqi199808No ratings yet
- 10 1016@j Prosdent 2016 08 036Document7 pages10 1016@j Prosdent 2016 08 036José Carlos Herrera IbarraNo ratings yet
- Digital Transfer of The Subgingival Contour and Emergence Profile of The Provisional Restoration To The Final Bone-Anchored Fixed RestorationDocument5 pagesDigital Transfer of The Subgingival Contour and Emergence Profile of The Provisional Restoration To The Final Bone-Anchored Fixed RestorationAngelia PratiwiNo ratings yet
- Characterization of Retrieved OrthodonticDocument7 pagesCharacterization of Retrieved OrthodonticMaria SilvaNo ratings yet
- 3D-Finite Element Analysis of Molars Restored WithDocument9 pages3D-Finite Element Analysis of Molars Restored Withabhilashanand3No ratings yet
- Comparison of Microtomography and Optical Coherence Tomography On Apical Endodontic Filling AnalysisDocument6 pagesComparison of Microtomography and Optical Coherence Tomography On Apical Endodontic Filling AnalysisLeticia RiveraNo ratings yet
- 6 - Fabrication of An Implant-Supported Overdenture Using CAD-CAM Technology A Clinical ReportDocument8 pages6 - Fabrication of An Implant-Supported Overdenture Using CAD-CAM Technology A Clinical ReportkochikaghochiNo ratings yet
- US4403961 ProsteticsDocument7 pagesUS4403961 ProsteticsSchuster StephanNo ratings yet
- CAD-CAM Milled Dentures: The Geneva Protocols For Digital DenturesDocument11 pagesCAD-CAM Milled Dentures: The Geneva Protocols For Digital DenturesJames LinNo ratings yet
- 3D Reinforcement of Stiffener-To-Skin T-Joints by Z-Pinning and TuftingDocument9 pages3D Reinforcement of Stiffener-To-Skin T-Joints by Z-Pinning and TuftingLouis GrouNo ratings yet
- Biologic and Esthetic Outcome of CAD/CAM Custom Ceramic Implant Abutment: A Clinical ReportDocument4 pagesBiologic and Esthetic Outcome of CAD/CAM Custom Ceramic Implant Abutment: A Clinical ReportMohanad BraziNo ratings yet
- Aboutara 2011Document4 pagesAboutara 2011Alejandra LorancaNo ratings yet
- Construction of An Implant-Retained Auricular Prosthesis With The Aid of Contemporary Digital Technologies: A Clinical ReportDocument5 pagesConstruction of An Implant-Retained Auricular Prosthesis With The Aid of Contemporary Digital Technologies: A Clinical ReportnoranNo ratings yet
- T. Thygesen, C. Slots, M.B. Jensen, N. Ditzel, M. Kassem, L. Langhorn, M.Ø. AndersenDocument7 pagesT. Thygesen, C. Slots, M.B. Jensen, N. Ditzel, M. Kassem, L. Langhorn, M.Ø. AndersenAnca TomaNo ratings yet
- 1 s2.0 S2212440312000442 MainDocument6 pages1 s2.0 S2212440312000442 MainMarinaNo ratings yet
- Impresiones 3DDocument9 pagesImpresiones 3DDeyvi Emerson Rivas ZarateNo ratings yet
- Gil Santos2018Document6 pagesGil Santos2018Lando GriffinNo ratings yet
- Jaw Relationship Assessment For Removable Complete Dentures Using The T-Scan Computerised System - A Case ReportDocument6 pagesJaw Relationship Assessment For Removable Complete Dentures Using The T-Scan Computerised System - A Case ReportananthNo ratings yet
- Border MoldingDocument6 pagesBorder MoldingArun PrasadNo ratings yet
- Barnes 1978Document15 pagesBarnes 1978ismail.bliamsiNo ratings yet
- Hardness Measurement and Eval Uation of Thin Film On Material Surf AceDocument7 pagesHardness Measurement and Eval Uation of Thin Film On Material Surf Acearm coreNo ratings yet
- Lang 1995Document14 pagesLang 1995noufabdulaziz00No ratings yet
- CB-McCormack96 000Document6 pagesCB-McCormack96 000steigmannNo ratings yet
- Conservative and Endodontics MCQsDocument9 pagesConservative and Endodontics MCQshussamNo ratings yet
- Tfie International Journal of Periodontics & Restorative DentistryDocument9 pagesTfie International Journal of Periodontics & Restorative DentistryVICTOR FERNANDO LAMAS LARANo ratings yet
- Casas-Murillo2021 Article 3D-printedAnatomicalModelsOfThDocument8 pagesCasas-Murillo2021 Article 3D-printedAnatomicalModelsOfThVicente Bruno GuimaraesNo ratings yet
- Management of Complex Orbital Fractures: Article in PressDocument5 pagesManagement of Complex Orbital Fractures: Article in Pressstoia_sebiNo ratings yet
- A Comparison of Two Arthroscopic Techniques For Interpositional Polytetrafluoroethylene Patch Repair For Massive Irreparable Rotator Cuff Tears - Speed and BiomechanicsDocument6 pagesA Comparison of Two Arthroscopic Techniques For Interpositional Polytetrafluoroethylene Patch Repair For Massive Irreparable Rotator Cuff Tears - Speed and BiomechanicsDiego Rivas-VazquezNo ratings yet
- BSSODocument6 pagesBSSOPaula RusuNo ratings yet
- Content ServerDocument8 pagesContent ServerJuan Carlos MeloNo ratings yet
- Evaluation of Adaptation of Ceramic Inlays Using Optical Coherence 2019Document10 pagesEvaluation of Adaptation of Ceramic Inlays Using Optical Coherence 2019Valentin SerbanNo ratings yet
- Reabsorção 3 2023Document3 pagesReabsorção 3 2023Vinicíus PavaniNo ratings yet
- Comparacion Del Ajuste MarginalDocument6 pagesComparacion Del Ajuste MarginalXiomara Reyes palominoNo ratings yet
- Research And: Alaa El-Ashkar, BDS, MS, Maha Taymour, BDS, PHD, and Adel El-Tannir, BDS, MSDDocument8 pagesResearch And: Alaa El-Ashkar, BDS, MS, Maha Taymour, BDS, PHD, and Adel El-Tannir, BDS, MSDDiana TanasaNo ratings yet
- Evaluation of Adaptation of Ceramic Inlays Using Optical Coherence Tomography and Replica Technique PDFDocument10 pagesEvaluation of Adaptation of Ceramic Inlays Using Optical Coherence Tomography and Replica Technique PDFZardasht NajmadineNo ratings yet
- 10 1016@j Prosdent 2020 04 016Document7 pages10 1016@j Prosdent 2020 04 016Luis Miguel ValenciaNo ratings yet
- Inpection Procedure Pre-Dispatch (Extruder) PDFDocument1 pageInpection Procedure Pre-Dispatch (Extruder) PDFAthulya PallipurathNo ratings yet
- Plastic Reprocess Machine - Inpection ProcedureDocument1 pagePlastic Reprocess Machine - Inpection ProcedureAthulya PallipurathNo ratings yet
- Reprocess - Operators Manual PDFDocument2 pagesReprocess - Operators Manual PDFAthulya PallipurathNo ratings yet
- Operators Manual (Extruder) PDFDocument2 pagesOperators Manual (Extruder) PDFAthulya PallipurathNo ratings yet
- Restoration of Root Canal Treated Teeth (2016) PDFDocument262 pagesRestoration of Root Canal Treated Teeth (2016) PDFStef AleNo ratings yet
- Chaniotis Endodontic Practice UKDocument8 pagesChaniotis Endodontic Practice UKFebriani Seroja100% (1)
- Stanley1966 PDFDocument10 pagesStanley1966 PDFAthulya PallipurathNo ratings yet
- Immediate Dentin Sealing A Literature ReviewDocument24 pagesImmediate Dentin Sealing A Literature ReviewAmin RouhaniNo ratings yet
- ProTaper Universal Endodontic System Bibx9ea en 1402 PDFDocument7 pagesProTaper Universal Endodontic System Bibx9ea en 1402 PDFManoj KnNo ratings yet
- E AvulsionDocument9 pagesE Avulsionlilia ilyahNo ratings yet
- Workingwidth PDFDocument3 pagesWorkingwidth PDFAthulya PallipurathNo ratings yet
- (AB-ANI) Program SpecificationDocument8 pages(AB-ANI) Program SpecificationMycah EvangelistaNo ratings yet
- Alderamin On The Sky - Volume 7Document311 pagesAlderamin On The Sky - Volume 7Pedro SilvaNo ratings yet
- Lithospheric Evolution of The Pre-And Early Andean Convergent Margin, ChileDocument29 pagesLithospheric Evolution of The Pre-And Early Andean Convergent Margin, ChileAbdiel MuñozNo ratings yet
- 9A02505 Electrical Machines-IIIDocument4 pages9A02505 Electrical Machines-IIIsivabharathamurthyNo ratings yet
- PASSAGE ONE (Questions 1-4)Document5 pagesPASSAGE ONE (Questions 1-4)Vian LonkzeerNo ratings yet
- Da Insem AllDocument217 pagesDa Insem AllTECOA136TejasJadhavNo ratings yet
- Evolis User ManualDocument28 pagesEvolis User ManualIonmadalin1000No ratings yet
- Union Metal SemiconductorDocument4 pagesUnion Metal SemiconductorskinhugoNo ratings yet
- Secondary GeographyDocument127 pagesSecondary GeographyAbcdNo ratings yet
- UnitPlan (P.E) Grade 6Document13 pagesUnitPlan (P.E) Grade 6Lou At CamellaNo ratings yet
- Advanced Office Add-In DevelopmentDocument40 pagesAdvanced Office Add-In DevelopmentReadoneNo ratings yet
- BFISDocument1 pageBFISEverestNo ratings yet
- One Wavelength To Loop SkywireDocument2 pagesOne Wavelength To Loop SkywireRobert TurnerNo ratings yet
- Pepperl KFD2 STC4 EX1.20 DatasheetDocument2 pagesPepperl KFD2 STC4 EX1.20 DatasheetAhmed HusseinNo ratings yet
- MLAB 3 - BoilerDocument3 pagesMLAB 3 - BoilerReden LopezNo ratings yet
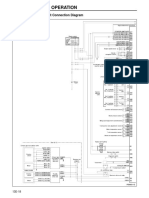
- Structure and Operation: 3. Electronic Control Unit Connection DiagramDocument16 pagesStructure and Operation: 3. Electronic Control Unit Connection DiagramAung Hlaing Min MyanmarNo ratings yet
- Ground Vehicle Operations ICAODocument31 pagesGround Vehicle Operations ICAOMohran HakimNo ratings yet
- Addressing Diversity Through The Years Special and Inclusive EducationDocument6 pagesAddressing Diversity Through The Years Special and Inclusive EducationJiezel SurinNo ratings yet
- Detailed Lesson Plan in Mathematics 10 I. ObjectivesDocument4 pagesDetailed Lesson Plan in Mathematics 10 I. ObjectivesLouis Fetilo FabunanNo ratings yet
- Mecanica MD - AZG-UDocument29 pagesMecanica MD - AZG-UStefanoViganóNo ratings yet
- WideScreen Code For PS2 GamesDocument78 pagesWideScreen Code For PS2 Gamesmarcus viniciusNo ratings yet
- Engine Torque Settings and Spec's 3.0L V6 SCDocument4 pagesEngine Torque Settings and Spec's 3.0L V6 SCMario MaravillaNo ratings yet
- Accommodating Expansion of Brickwork: Technical Notes 18ADocument13 pagesAccommodating Expansion of Brickwork: Technical Notes 18AWissam AlameddineNo ratings yet
- Rivers and Their Origin (Top MCQ)Document24 pagesRivers and Their Origin (Top MCQ)Anil Yadav100% (1)
- TM 9-1425-429-12-HR - Stinger - Training - Set - 1983 PDFDocument34 pagesTM 9-1425-429-12-HR - Stinger - Training - Set - 1983 PDFWurzel1946No ratings yet
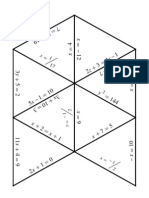
- Algebra1 Review PuzzleDocument3 pagesAlgebra1 Review PuzzleNicholas Yates100% (1)
- Inglês - Degrees of ComparisonDocument4 pagesInglês - Degrees of ComparisonVersehgi IINo ratings yet
- Motorola Talkabout T82 PDFDocument184 pagesMotorola Talkabout T82 PDFAlex TamayoNo ratings yet
- TCS3400 DS000411 4-00Document34 pagesTCS3400 DS000411 4-00Miguel_Angel92No ratings yet
- PienaDocument1 pagePienaMika Flores PedroNo ratings yet
- The Laws of Thermodynamics: A Very Short IntroductionFrom EverandThe Laws of Thermodynamics: A Very Short IntroductionRating: 4.5 out of 5 stars4.5/5 (10)
- Einstein's Fridge: How the Difference Between Hot and Cold Explains the UniverseFrom EverandEinstein's Fridge: How the Difference Between Hot and Cold Explains the UniverseRating: 4.5 out of 5 stars4.5/5 (51)
- Offshore Mechanics: Structural and Fluid Dynamics for Recent ApplicationsFrom EverandOffshore Mechanics: Structural and Fluid Dynamics for Recent ApplicationsNo ratings yet
- Pressure Vessels: Design, Formulas, Codes, and Interview Questions & Answers ExplainedFrom EverandPressure Vessels: Design, Formulas, Codes, and Interview Questions & Answers ExplainedRating: 5 out of 5 stars5/5 (1)
- Pilot's Handbook of Aeronautical Knowledge (2024): FAA-H-8083-25CFrom EverandPilot's Handbook of Aeronautical Knowledge (2024): FAA-H-8083-25CNo ratings yet
- Introduction to the Explicit Finite Element Method for Nonlinear Transient DynamicsFrom EverandIntroduction to the Explicit Finite Element Method for Nonlinear Transient DynamicsNo ratings yet
- Handbook of Mechanical and Materials EngineeringFrom EverandHandbook of Mechanical and Materials EngineeringRating: 5 out of 5 stars5/5 (4)
- Post Weld Heat Treatment PWHT: Standards, Procedures, Applications, and Interview Q&AFrom EverandPost Weld Heat Treatment PWHT: Standards, Procedures, Applications, and Interview Q&ANo ratings yet
- 1,001 Questions & Answers for the CWI Exam: Welding Metallurgy and Visual Inspection Study GuideFrom Everand1,001 Questions & Answers for the CWI Exam: Welding Metallurgy and Visual Inspection Study GuideRating: 3.5 out of 5 stars3.5/5 (7)
- Waves and Beaches: The Powerful Dynamics of Sea and CoastFrom EverandWaves and Beaches: The Powerful Dynamics of Sea and CoastRating: 4 out of 5 stars4/5 (1)
- The Art of Welding: Featuring Ryan Friedlinghaus of West Coast CustomsFrom EverandThe Art of Welding: Featuring Ryan Friedlinghaus of West Coast CustomsNo ratings yet
- Fuels, Furnaces and Refractories: International Series on Materials Science and TechnologyFrom EverandFuels, Furnaces and Refractories: International Series on Materials Science and TechnologyRating: 5 out of 5 stars5/5 (1)
- Advanced Computer-Aided Fixture DesignFrom EverandAdvanced Computer-Aided Fixture DesignRating: 5 out of 5 stars5/5 (1)
- Hyperspace: A Scientific Odyssey Through Parallel Universes, Time Warps, and the 10th DimensionFrom EverandHyperspace: A Scientific Odyssey Through Parallel Universes, Time Warps, and the 10th DimensionRating: 4.5 out of 5 stars4.5/5 (3)
- Airplane Flying Handbook: FAA-H-8083-3C (2024)From EverandAirplane Flying Handbook: FAA-H-8083-3C (2024)Rating: 4 out of 5 stars4/5 (12)
- Practical Hydraulic Systems: Operation and Troubleshooting for Engineers and TechniciansFrom EverandPractical Hydraulic Systems: Operation and Troubleshooting for Engineers and TechniciansRating: 4 out of 5 stars4/5 (8)
- Heat Exchanger Design Guide: A Practical Guide for Planning, Selecting and Designing of Shell and Tube ExchangersFrom EverandHeat Exchanger Design Guide: A Practical Guide for Planning, Selecting and Designing of Shell and Tube ExchangersRating: 4 out of 5 stars4/5 (13)
- Rolling Bearing Tribology: Tribology and Failure Modes of Rolling Element BearingsFrom EverandRolling Bearing Tribology: Tribology and Failure Modes of Rolling Element BearingsNo ratings yet