You might also like
- Comprehensive Sexuality Education OverviewDocument25 pagesComprehensive Sexuality Education OverviewMayda Rivera100% (5)
- HIV AIDS awareness workshopsDocument13 pagesHIV AIDS awareness workshopsDiana Laura Lei57% (7)
- 2021 RPRH Annual ReportDocument108 pages2021 RPRH Annual ReportVNo ratings yet
- HIV and AIDS in Malawi Groups Most Affected by HIV in Malawi HIV Disproportionately Affects Women in Malawi PDFDocument14 pagesHIV and AIDS in Malawi Groups Most Affected by HIV in Malawi HIV Disproportionately Affects Women in Malawi PDFJames ChinamasaNo ratings yet
- Around-World/sub-Saharan-Africa/zimb Abwe: Hiv and Aids in ZimbabweDocument10 pagesAround-World/sub-Saharan-Africa/zimb Abwe: Hiv and Aids in Zimbabweapi-347768366No ratings yet
- Trends of HIVDocument30 pagesTrends of HIVkimaniNo ratings yet
- China's Progress in Tackling HIV Despite ChallengesDocument7 pagesChina's Progress in Tackling HIV Despite Challengessaiful azis setyawanNo ratings yet
- HIV AIDS HandoutDocument11 pagesHIV AIDS HandoutMarius BuysNo ratings yet
- PR Weve Got The Power enDocument2 pagesPR Weve Got The Power enDavidNo ratings yet
- "Young African Women Are Especially Vulnerable To Hiv/Aids" by Jon Cohen (Nov. 21, 2016)Document3 pages"Young African Women Are Especially Vulnerable To Hiv/Aids" by Jon Cohen (Nov. 21, 2016)sartiniNo ratings yet
- HIV and AIDs Status in NigeriaDocument15 pagesHIV and AIDs Status in NigeriaRufai HarunaNo ratings yet
- 2 factors fueling PH's rising HIV risk: Early sex, lack of infoDocument5 pages2 factors fueling PH's rising HIV risk: Early sex, lack of infoErlinda PosadasNo ratings yet
- Are Societal Taboos Leading Us To An HIV Pandemic?Document2 pagesAre Societal Taboos Leading Us To An HIV Pandemic?Hira ShafqatNo ratings yet
- Southeast Asia Regional Program: Overall HIV TrendsDocument7 pagesSoutheast Asia Regional Program: Overall HIV TrendsAkbar TaufikNo ratings yet
- Ojsadmin, 406Document5 pagesOjsadmin, 406Frans LandiNo ratings yet
- HIV/AIDS in The Philippines: At-Risk GroupsDocument3 pagesHIV/AIDS in The Philippines: At-Risk GroupsChristian Punto FedereNo ratings yet
- Program Implementation Review - Block 5Document20 pagesProgram Implementation Review - Block 5jollyhotdog89No ratings yet
- A Qualitative Analysis of Multi Level Barriers To HIV Testing Among Women in LebanonDocument16 pagesA Qualitative Analysis of Multi Level Barriers To HIV Testing Among Women in LebanonMamadou WattNo ratings yet
- International AIDS Conference: Los Angeles TimesDocument23 pagesInternational AIDS Conference: Los Angeles TimesGomathi Sankar100% (1)
- Capstone Noreen 1Document45 pagesCapstone Noreen 1api-560728162No ratings yet
- UNAIDS - The Gap ReportDocument422 pagesUNAIDS - The Gap ReportAdrian ArizmendiNo ratings yet
- Christine Jean Ceridon-1 FINAL (Autosaved) - 1Document40 pagesChristine Jean Ceridon-1 FINAL (Autosaved) - 1Christine Jean CeredonNo ratings yet
- AvertDocument16 pagesAvertAdil razaNo ratings yet
- AIDS in IndiaDocument11 pagesAIDS in IndiavinothrengrajNo ratings yet
- Awareness of HIV/AIDS Among Grade 10 Students in Teofilo V. Fernandez National High SchoolDocument18 pagesAwareness of HIV/AIDS Among Grade 10 Students in Teofilo V. Fernandez National High SchoolChristine Jean CeredonNo ratings yet
- Final Version of HIV ResearchDocument29 pagesFinal Version of HIV ResearchJordan Abosama MamalumpongNo ratings yet
- Jurnal Fatimah Azzahra Fix Up1Document12 pagesJurnal Fatimah Azzahra Fix Up1Fatimah AzzahraNo ratings yet
- Ellect 100Document3 pagesEllect 100Hero SabanalNo ratings yet
- Navigating Disclosure Obstacles Encountered by Individuals With HIV at Kakomo Healing Centre IV in Kabale DistrictDocument15 pagesNavigating Disclosure Obstacles Encountered by Individuals With HIV at Kakomo Healing Centre IV in Kabale DistrictKIU PUBLICATION AND EXTENSIONNo ratings yet
- H I V / A I D S: Prevention and Care Strategies For HIVDocument7 pagesH I V / A I D S: Prevention and Care Strategies For HIVIin Ainur AnamNo ratings yet
- NGA 2020 CountryreportDocument46 pagesNGA 2020 Countryreportodetundehabeeb3No ratings yet
- Zambia HIV/AIDS Data IntegrityDocument1 pageZambia HIV/AIDS Data IntegrityReal KezeeNo ratings yet
- 2019 Global Aids Update - Key Messages - enDocument12 pages2019 Global Aids Update - Key Messages - enZahoor KhanNo ratings yet
- Report On Global Aids EpidemicDocument13 pagesReport On Global Aids Epidemictaizya cNo ratings yet
- Essay - Public HealthDocument15 pagesEssay - Public Healthtooba ShehzadNo ratings yet
- AIDS: 30 Years OnDocument1 pageAIDS: 30 Years OnMedlabs - Sehtak Bil DeniaNo ratings yet
- Sex Workers Research Paper Davie SimengwaDocument37 pagesSex Workers Research Paper Davie SimengwatarikNo ratings yet
- Article HealthDocument3 pagesArticle Healthkaii cutieNo ratings yet
- Aids PDFDocument5 pagesAids PDFmiguel gaquitNo ratings yet
- NORMINCORHD Final HIV AIDS Proposal For PCHRD SubmissionDocument11 pagesNORMINCORHD Final HIV AIDS Proposal For PCHRD SubmissionMyk Twentytwenty NBeyondNo ratings yet
- Overview of HIV Interventions For Young PeopleDocument8 pagesOverview of HIV Interventions For Young PeopleCrowdOutAIDSNo ratings yet
- How HIV Is DetectedDocument12 pagesHow HIV Is DetectedTaranisaNo ratings yet
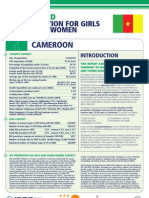
- Hiv Prevention Girls and Young Women Cameroon Report CardDocument8 pagesHiv Prevention Girls and Young Women Cameroon Report CardAsghar KhanNo ratings yet
- Chapter One 1.0 Background To The StudyDocument55 pagesChapter One 1.0 Background To The StudyAbiodun GideonNo ratings yet
- Interaction Between HIV Awareness, Knowledge, Safe Sex Practice and HIV Incidence: Evidence From BotswanaDocument25 pagesInteraction Between HIV Awareness, Knowledge, Safe Sex Practice and HIV Incidence: Evidence From BotswanaSiiPhie FithriNo ratings yet
- HIV/AIDS Awareness Evaluation in The Junior and Senior High School Students of University of The East Caloocan (UEC)Document11 pagesHIV/AIDS Awareness Evaluation in The Junior and Senior High School Students of University of The East Caloocan (UEC)Sebastian Miguel CarlosNo ratings yet
- Paper On HIV Widows FinalDocument5 pagesPaper On HIV Widows FinalAntriya DevarajNo ratings yet
- Aids Research Paper ConclusionDocument6 pagesAids Research Paper Conclusionjmforlwgf100% (1)
- JC2112 Synthesis Report enDocument112 pagesJC2112 Synthesis Report enPennapa KaweewongprassertNo ratings yet
- TBL Case 6 US StatisticsDocument6 pagesTBL Case 6 US StatisticsOmar RamadanNo ratings yet
- HIV: The Good News and The Bad NewsDocument1 pageHIV: The Good News and The Bad NewsCityPressNo ratings yet
- Predictors of HIV Positive Pregnant Women's Use of Sexual and Reproductive Health Services in Taraba State A Mixed Method ApproachDocument8 pagesPredictors of HIV Positive Pregnant Women's Use of Sexual and Reproductive Health Services in Taraba State A Mixed Method ApproachInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Uganda Still Dying of IgnoranceDocument2 pagesUganda Still Dying of Ignorancecar555No ratings yet
- (IJIT-V7I4P6) :smt. G. Santhalakshmi, Dr. M. MuninarayanappaDocument6 pages(IJIT-V7I4P6) :smt. G. Santhalakshmi, Dr. M. MuninarayanappaIJITJournalsNo ratings yet
- HSE2010 Ch6 Sexual HealthDocument29 pagesHSE2010 Ch6 Sexual HealthErin GallagherNo ratings yet
- Association of Hiv Knowledge Testing Attitudes and Risk AssessmentDocument8 pagesAssociation of Hiv Knowledge Testing Attitudes and Risk AssessmentALEXANDRANICOLE OCTAVIANONo ratings yet
- Final Aids Model 2Document10 pagesFinal Aids Model 2Vince VI Dacer GeneralaoNo ratings yet
- Strategies for Awareness & Prevention of Hiv/Aids Among African-Americans: A Hand BookFrom EverandStrategies for Awareness & Prevention of Hiv/Aids Among African-Americans: A Hand BookNo ratings yet
- Domestic Abuse and Violence in the COVID-19 Pandemic: The Dark Side of the LockdownFrom EverandDomestic Abuse and Violence in the COVID-19 Pandemic: The Dark Side of the LockdownNo ratings yet
- Negotiating Pharmaceutical Uncertainty: Women's Agency in a South African HIV Prevention TrialFrom EverandNegotiating Pharmaceutical Uncertainty: Women's Agency in a South African HIV Prevention TrialNo ratings yet
- 3A G1 Final Chapters 1 To 5Document125 pages3A G1 Final Chapters 1 To 5atozplockNo ratings yet
- Gender Responsive Legislator 062321Document76 pagesGender Responsive Legislator 062321Faye ReyesNo ratings yet
- The Use of Peer Support On Adolescent Health Among Senior High School StudentsDocument6 pagesThe Use of Peer Support On Adolescent Health Among Senior High School Studentsjunengsih poltek3jktNo ratings yet
- GenderDocument3 pagesGenderAlliah Juliana De TorresNo ratings yet
- Consumer Act of The PhilippinesDocument4 pagesConsumer Act of The PhilippinesFrancis PeñeroNo ratings yet
- BIYYA RP October 2023 ON RHDocument65 pagesBIYYA RP October 2023 ON RHBiyaNo ratings yet
- GE Elect 3 Module 13 14 MangiboaDocument8 pagesGE Elect 3 Module 13 14 MangiboaMary Loiesyl Camara Ubay-ubayNo ratings yet
- 2023 PREFINALS - Improving PH Thru PharmacyDocument141 pages2023 PREFINALS - Improving PH Thru PharmacyAnthony PamolinoNo ratings yet
- Adolescent Reproductive and Sexual HealthDocument42 pagesAdolescent Reproductive and Sexual HealthMuhammad Abbas WaliNo ratings yet
- Unsafe AbortionsDocument3 pagesUnsafe AbortionsIsleen CleofasNo ratings yet
- MCH Epidemiology Issues MagnitudeDocument25 pagesMCH Epidemiology Issues MagnitudeRatna KumariNo ratings yet
- 2020 Fertility, Sexuality Awarenes TrainingDocument23 pages2020 Fertility, Sexuality Awarenes TrainingPel Vincent CruzNo ratings yet
- Lesson 28 Gender and Other Cross-Cutting Issues (Education, General Health, Mental Health)Document14 pagesLesson 28 Gender and Other Cross-Cutting Issues (Education, General Health, Mental Health)Leny LayaNo ratings yet
- Concept PaperDocument3 pagesConcept PaperRogella Hamoy100% (1)
- Ahlam Na - BaldevaronaDocument29 pagesAhlam Na - BaldevaronaLos DesvalNo ratings yet
- GAD Code Working DocumentDocument36 pagesGAD Code Working DocumentJoemar CafrancaNo ratings yet
- Curriculum Health Grade07Document3 pagesCurriculum Health Grade07AlexNo ratings yet
- Research PaperDocument8 pagesResearch PaperLei Andrew BalmacedaNo ratings yet
- Health 10Document20 pagesHealth 10jenayadaNo ratings yet
- BEmONC - Facilitators Guide - v02Document60 pagesBEmONC - Facilitators Guide - v02lolemo kelbisoNo ratings yet
- Reproductive Health Course for Public Health StudentsDocument36 pagesReproductive Health Course for Public Health StudentsBehar AbdurahemanNo ratings yet
- Project Design Document - Model Answers-RAG ProjectDocument19 pagesProject Design Document - Model Answers-RAG ProjectGis ThaNo ratings yet
- TD - Reproductive Rights and Sexual and Reproductive Health - 0Document44 pagesTD - Reproductive Rights and Sexual and Reproductive Health - 0Al Francis Amper LongosNo ratings yet
- 2 Population GrowthDocument25 pages2 Population GrowthShane VeiraNo ratings yet
- Text of ACOG EndorsementDocument1 pageText of ACOG EndorsementJo InglesNo ratings yet
- Philippines AFHS - Standards and Implementation GuideDocument37 pagesPhilippines AFHS - Standards and Implementation GuideShardin Labawan-Juen,RNNo ratings yet
- 2011 Nowicka SRRand Human RightsDocument11 pages2011 Nowicka SRRand Human RightsÁlvaro FrancoNo ratings yet
- Early Marrige Practices and Perception of Badjao in Inognong Bataraza PalawanDocument38 pagesEarly Marrige Practices and Perception of Badjao in Inognong Bataraza PalawanJonalyn Adjarani DiazNo ratings yet