You might also like
- CVA Nursing Lesson PlanDocument6 pagesCVA Nursing Lesson Plansimonjosan60% (5)
- Ergonomics in Dentistry: By, DR - Rakesh R Nair P.G Student Cons & Endo KVG Dental CollegeDocument94 pagesErgonomics in Dentistry: By, DR - Rakesh R Nair P.G Student Cons & Endo KVG Dental Collegenur awanisNo ratings yet
- Meaning and Definition of Management DevelopmentDocument7 pagesMeaning and Definition of Management DevelopmentRiteshTirkey100% (2)
- Seminar Presentation On Stroke by Wubet & Worku: University of Gondar College of Medicine and Health ScienceDocument40 pagesSeminar Presentation On Stroke by Wubet & Worku: University of Gondar College of Medicine and Health Sciencealemante tafeseNo ratings yet
- The Operating TheatreDocument30 pagesThe Operating TheatrePrincewill SeiyefaNo ratings yet
- Stroke GuidelinesDocument60 pagesStroke GuidelinesMuhammad Agus NashirNo ratings yet
- #0、aneurysmDocument39 pages#0、aneurysmMargaret ThatcherNo ratings yet
- Pharmacological Treatment of Vertigo: Timothy C. Hain and Mohammed UddinDocument16 pagesPharmacological Treatment of Vertigo: Timothy C. Hain and Mohammed UddinFan AccountNo ratings yet
- 1 - Neuro Assessment 2021 - 336Document30 pages1 - Neuro Assessment 2021 - 336HADI BADWAN100% (2)
- Reducing Your Risk of Stroke: Don't Wait For It To Happen To YouDocument8 pagesReducing Your Risk of Stroke: Don't Wait For It To Happen To YouSavitri Maharani BudimanNo ratings yet
- What Is Cerebral Palsy PDFDocument1 pageWhat Is Cerebral Palsy PDFElaine BriososNo ratings yet
- Assist Patient From The Bed To Chair or WheelchairDocument1 pageAssist Patient From The Bed To Chair or WheelchairKryztalGhail Llanora100% (1)
- Braddoms 2020 - Capitulo 10 - Protesis Eeii y MarchaDocument38 pagesBraddoms 2020 - Capitulo 10 - Protesis Eeii y MarchaSergio Navarrete VidalNo ratings yet
- 10 Hip Replacement SurgeryDocument13 pages10 Hip Replacement SurgeryDIA PHONG THANGNo ratings yet
- A Systematic Review On Dementia CareDocument5 pagesA Systematic Review On Dementia CareInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- DystoniaDocument24 pagesDystoniaAyesha NasirNo ratings yet
- Atlas of Nerve Conduction Studies and Electromyography (2 Ed.)Document10 pagesAtlas of Nerve Conduction Studies and Electromyography (2 Ed.)rodrigocorcino899959No ratings yet
- UE 1 Clavicle FracturesDocument46 pagesUE 1 Clavicle FracturesDavidBeatonComuladaNo ratings yet
- Current Concepts in Elbow Fracture Dislocation: Adam C Watts, Jagwant Singh, Michael Elvey and Zaid HamoodiDocument8 pagesCurrent Concepts in Elbow Fracture Dislocation: Adam C Watts, Jagwant Singh, Michael Elvey and Zaid HamoodiJoão Artur BonadimanNo ratings yet
- Dystonia Is A Movement Disorder in Which A PersonDocument4 pagesDystonia Is A Movement Disorder in Which A Personsrirahmawahyuni sarahNo ratings yet
- Chapter 11: Pathophysiology of SciaticaDocument14 pagesChapter 11: Pathophysiology of SciaticaTraian UrsuNo ratings yet
- Compilation 2017Document842 pagesCompilation 2017Krystal Shine BalabboNo ratings yet
- Progressive Myoclonic Epilepsies - Practical Neurology 2015. MalekDocument8 pagesProgressive Myoclonic Epilepsies - Practical Neurology 2015. MalekchintanNo ratings yet
- HT CvaDocument10 pagesHT CvaTopeshwar TpkNo ratings yet
- Cerebrovascular AccidentDocument21 pagesCerebrovascular AccidentCJNo ratings yet
- CVABDocument4 pagesCVABRobby BanjarNo ratings yet
- Types and Symptoms of StrokesDocument4 pagesTypes and Symptoms of StrokesRobby BanjarNo ratings yet
- What Is A StrokeDocument2 pagesWhat Is A Strokenowrin05273815No ratings yet
- CVADocument11 pagesCVACla100% (4)
- Hemorrhagic Stroke Patient EducationDocument9 pagesHemorrhagic Stroke Patient EducationBhavana VNo ratings yet
- Emergency vs non-emergency situationsDocument8 pagesEmergency vs non-emergency situationsSitti NaifaNo ratings yet
- Ucm 309710Document2 pagesUcm 309710aster_dharmawanNo ratings yet
- StrokeDocument20 pagesStrokejawad_ahmedNo ratings yet
- PregnancyDocument20 pagesPregnancyjawad_ahmedNo ratings yet
- REPORTDocument34 pagesREPORTClaire GidoNo ratings yet
- Cerebrovascular AccidentDocument15 pagesCerebrovascular AccidentBeeshma BirjasinghNo ratings yet
- Stroke Case Study 3-Wendte 1Document18 pagesStroke Case Study 3-Wendte 1api-371766376No ratings yet
- 5 CS and 5 RSDocument54 pages5 CS and 5 RSKristine CatariningNo ratings yet
- Cerebrovascular Accident/Stroke: Rodney R. Reyes, RNDocument51 pagesCerebrovascular Accident/Stroke: Rodney R. Reyes, RNRodney ReyesNo ratings yet
- Living ThingsDocument24 pagesLiving ThingsAlfred PaltaoNo ratings yet
- Preventing Stroke PresentationDocument29 pagesPreventing Stroke PresentationIndira DebnathNo ratings yet
- What Is StrokeDocument14 pagesWhat Is StrokedindaNo ratings yet
- Cerebrovascular Accident (CVA)Document71 pagesCerebrovascular Accident (CVA)nur muizzah afifah hussinNo ratings yet
- F29 Dementia After StrokeDocument20 pagesF29 Dementia After StrokeAkhmad Ulil AlbabNo ratings yet
- Ems StrokeDocument29 pagesEms StrokeaathulNo ratings yet
- Case PresentationDocument34 pagesCase PresentationAdelle Fortunato100% (1)
- Understanding Stroke Preventative Care & Treatment Post-StrokeDocument12 pagesUnderstanding Stroke Preventative Care & Treatment Post-StrokeakamNo ratings yet
- CVA HEALTH TEACHING PLANDocument14 pagesCVA HEALTH TEACHING PLANArakama NurdalynNo ratings yet
- Neurologic Emergencies: Stroke & TIADocument10 pagesNeurologic Emergencies: Stroke & TIASamantha Lui100% (2)
- CVA and Hypertension Symptoms and ComplicationsDocument18 pagesCVA and Hypertension Symptoms and ComplicationsDoris BocanegraNo ratings yet
- Razonable Complete2.0 I.T Era - PPTX FinalDocument14 pagesRazonable Complete2.0 I.T Era - PPTX FinalJohn PiocoNo ratings yet
- Clipart StrokeDocument2 pagesClipart Strokekira0105No ratings yet
- Intan Purnamasari Stikes Surya Mitra Husada: StrokeDocument6 pagesIntan Purnamasari Stikes Surya Mitra Husada: StrokesrichusniahNo ratings yet
- STROKE TITLEDocument6 pagesSTROKE TITLEsrichusniahNo ratings yet
- Cerebrovascular Accident StrokeDocument3 pagesCerebrovascular Accident StrokeLuis LazaroNo ratings yet
- Understanding Strokes: Causes, Symptoms, and TreatmentDocument6 pagesUnderstanding Strokes: Causes, Symptoms, and TreatmentshaitabliganNo ratings yet
- Stroke PreventionDocument3 pagesStroke Preventionapi-27015740100% (2)
- STROKEDocument22 pagesSTROKEsyed saffwanNo ratings yet
- Cerebrovascular Accident ReportDocument16 pagesCerebrovascular Accident ReportAngelu Gabrielle CastroNo ratings yet
- Cerebrovascular Accident (Cva) : M.K. SastryDocument47 pagesCerebrovascular Accident (Cva) : M.K. SastryLupa IngatanNo ratings yet
- Intellectual DisabilityDocument25 pagesIntellectual DisabilityGhadeer AlomariNo ratings yet
- Understanding Tourette SyndromeDocument31 pagesUnderstanding Tourette SyndromeGhadeer AlomariNo ratings yet
- Understanding Tourette SyndromeDocument31 pagesUnderstanding Tourette SyndromeGhadeer AlomariNo ratings yet
- Marfan's SyndromeDocument8 pagesMarfan's SyndromeGhadeer AlomariNo ratings yet
- Practical Research 2: Quarter 1 - Module 2: Importance of Quantitative Research Across FieldsDocument16 pagesPractical Research 2: Quarter 1 - Module 2: Importance of Quantitative Research Across FieldsDivina Grace Rodriguez - LibreaNo ratings yet
- ArmourDocument5 pagesArmourBiju_PottayilNo ratings yet
- Sop Saad 3Document2 pagesSop Saad 3ZarmeenaGauharNo ratings yet
- India 2030 PDFDocument188 pagesIndia 2030 PDFGray HouserNo ratings yet
- Example Letter of Medical NecessityDocument4 pagesExample Letter of Medical Necessitystarlette.hara100% (1)
- Improve Balance and Coordination with Soccer LessonsDocument9 pagesImprove Balance and Coordination with Soccer LessonsAlvin Corpuz JrNo ratings yet
- Reducing Negativity in A WorkplaceDocument12 pagesReducing Negativity in A WorkplaceAna Jane Morales CasaclangNo ratings yet
- BCAA Powder MYPROTEIN™Document1 pageBCAA Powder MYPROTEIN™Cikgu Roxx RJNo ratings yet
- DSP 15-12-23Document36 pagesDSP 15-12-23Fu'ad ParkhaniNo ratings yet
- MCN ReviewerDocument3 pagesMCN ReviewerJunghoon YangParkNo ratings yet
- Pengumuman Jadwal Rapid Test Antigen Gratis Bagi Peserta Ujian SKB CPNS Pemerintah Kota Pangkalpinang 2021Document16 pagesPengumuman Jadwal Rapid Test Antigen Gratis Bagi Peserta Ujian SKB CPNS Pemerintah Kota Pangkalpinang 2021Syahrul SalehNo ratings yet
- November 2022 Philippine Nurse Licensure Examination ResultsDocument6 pagesNovember 2022 Philippine Nurse Licensure Examination ResultsRappler0% (1)
- SEMI FINAL FINAL NCM 113 NotesDocument1 pageSEMI FINAL FINAL NCM 113 Notesmblanco.dchNo ratings yet
- Experienced Pharmacist Seeking New OpportunityDocument3 pagesExperienced Pharmacist Seeking New OpportunityIman ElshafieNo ratings yet
- Meningioma Review of Epidemiology, Pathology, Diagnosis and TreatmentDocument15 pagesMeningioma Review of Epidemiology, Pathology, Diagnosis and Treatmentwibawa suryaNo ratings yet
- Pool Paint Safety Data SheetDocument9 pagesPool Paint Safety Data SheetNicholson Vhenz UyNo ratings yet
- Analysis of E. coli Bacteria in Coconut Water Sold in Medan TuntunganDocument10 pagesAnalysis of E. coli Bacteria in Coconut Water Sold in Medan TuntunganBenny SimanjuntakNo ratings yet
- Locate Indian Oil Petrol Pump in Belgaum District of Karnataka StateDocument20 pagesLocate Indian Oil Petrol Pump in Belgaum District of Karnataka StateDeva Chandra SekharNo ratings yet
- Reviewing Literature Learning Disability Fiction and The Social Work PerspectiveDocument13 pagesReviewing Literature Learning Disability Fiction and The Social Work Perspectiveauthor.avengingangelNo ratings yet
- Clinical Reasoning Evaluation Simulation Tool (CREST)Document3 pagesClinical Reasoning Evaluation Simulation Tool (CREST)BenToNo ratings yet
- 21 - Piriformis SyndromeDocument11 pages21 - Piriformis SyndromewatiNo ratings yet
- Bionic Final PDFDocument4 pagesBionic Final PDFJasmine RaoNo ratings yet
- Curriculam Vitae: ObjectiveDocument5 pagesCurriculam Vitae: ObjectiveGokul RajNo ratings yet
- Lesson 1:: Introduction To Science, Technology and SocietyDocument17 pagesLesson 1:: Introduction To Science, Technology and SocietyAlexis A. AguilarNo ratings yet
- Mother's HatredDocument835 pagesMother's HatredXoliswa Nakedi0% (1)
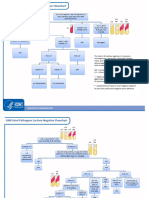
- GNR Stool Pathogens Lactose Negative FlowchartDocument2 pagesGNR Stool Pathogens Lactose Negative FlowchartKeithNo ratings yet
- SOP For Antimicrobial Effectiveness TestingDocument4 pagesSOP For Antimicrobial Effectiveness TestingGencay ErginNo ratings yet
- CareGroup Case Study QuestionsDocument1 pageCareGroup Case Study QuestionsEnrica Melissa PanjaitanNo ratings yet
- Pharmaceutical Marketing: Marketing Strategy Alternative Strategic ThrustsDocument29 pagesPharmaceutical Marketing: Marketing Strategy Alternative Strategic Thrustspremoshin100% (4)