You might also like
- Betty Blue Eyes Kotta PDFDocument306 pagesBetty Blue Eyes Kotta PDFCsóka Anita83% (6)
- Classification of Antibiotics For PrintingDocument4 pagesClassification of Antibiotics For PrintingMuthu Kumar100% (2)
- Assessment of Locomotive and Multi-Unit Fatigue Strength Considering The Results of Certifi Cation Tests in Ukraine and EU CountriesDocument8 pagesAssessment of Locomotive and Multi-Unit Fatigue Strength Considering The Results of Certifi Cation Tests in Ukraine and EU CountriesLeonardo Antônio Pereira100% (1)
- Chapter 28 Infections: Perioperative Antimicrobial PPXDocument10 pagesChapter 28 Infections: Perioperative Antimicrobial PPXDrashtibahen PatelNo ratings yet
- Building A Vacuum Forming TableDocument9 pagesBuilding A Vacuum Forming TableWil NelsonNo ratings yet
- Terraform AWSDocument1,531 pagesTerraform AWSTilted Mowa100% (1)
- Module 5 - Elements of Financial StatementsDocument34 pagesModule 5 - Elements of Financial StatementsRandolph ColladoNo ratings yet
- Infectious Disease - Antibiotic Ladder PDFDocument2 pagesInfectious Disease - Antibiotic Ladder PDFVaishali PrasharNo ratings yet
- WCDMA19 Prfile Descriptions W19P8 08A APPRDocument254 pagesWCDMA19 Prfile Descriptions W19P8 08A APPRoaguilar83No ratings yet
- Antibiotics in EndodonticsDocument74 pagesAntibiotics in EndodonticsdrishyaNo ratings yet
- Cpa Review School of The Philippines: Related Psas: Psa 700, 710, 720, 560, 570, 600 and 620Document49 pagesCpa Review School of The Philippines: Related Psas: Psa 700, 710, 720, 560, 570, 600 and 620Jasmine LimNo ratings yet
- Jean-Louis Cohen - Exhibitionist Revisionism - Exposing Architectural History (September 1999)Document10 pagesJean-Louis Cohen - Exhibitionist Revisionism - Exposing Architectural History (September 1999)Javier PerezNo ratings yet
- Drug of Abuse Substance of AbuseDocument10 pagesDrug of Abuse Substance of AbuseCARL ANGELA SISONNo ratings yet
- 2.2.4 - Cell Wall Inhibitors - Cephalosporines 2010-Oct 2014Document25 pages2.2.4 - Cell Wall Inhibitors - Cephalosporines 2010-Oct 2014tresorstephane669No ratings yet
- MICROBIO 1.2 Antimicrobial DrugsDocument3 pagesMICROBIO 1.2 Antimicrobial DrugsPatricia Elena ManaliliNo ratings yet
- Pharma Lecture Endterm ReviewerDocument32 pagesPharma Lecture Endterm ReviewerKristel RolloNo ratings yet
- Supporting Document of How To Choose Empirical Antibiotics in ICU Video LectureDocument7 pagesSupporting Document of How To Choose Empirical Antibiotics in ICU Video LectureNeha AgrawalNo ratings yet
- Pharma S03 SBR01 Le1Document15 pagesPharma S03 SBR01 Le1sky vallartaNo ratings yet
- Cefiget Range Leaflet PakistanDocument2 pagesCefiget Range Leaflet PakistanZafran KhanNo ratings yet
- Cell Wall Inhibitors - Cephalosporins Others 2Document32 pagesCell Wall Inhibitors - Cephalosporins Others 2Yosra AkashNo ratings yet
- Antimicrobials Drugs: Dr. Mohammed Al-KhawlaniDocument22 pagesAntimicrobials Drugs: Dr. Mohammed Al-Khawlaniخالد الشرعبيNo ratings yet
- Cephalosporins Quick ReviewDocument19 pagesCephalosporins Quick ReviewErinson Custodio PlasenciaNo ratings yet
- Cephalosporins GenerationDocument7 pagesCephalosporins GenerationSam SmileyNo ratings yet
- 1a Antiinfective DrugsDocument4 pages1a Antiinfective DrugsMaria Donabella OngueNo ratings yet
- Cell Wall Synthesis InhibitorsDocument57 pagesCell Wall Synthesis InhibitorsNica MendozaNo ratings yet
- 1 Generation: Cefalexin Cefradin Cefadroxil Cefachlor Yes Yes Yes Yes YesDocument67 pages1 Generation: Cefalexin Cefradin Cefadroxil Cefachlor Yes Yes Yes Yes YesadystiNo ratings yet
- Pediatric Hospital-Acquired and Ventilator-Associated Pneumonia Topic DiscussionDocument5 pagesPediatric Hospital-Acquired and Ventilator-Associated Pneumonia Topic Discussionapi-602288180No ratings yet
- USMLE Step 3 Lecture Notes 2017-2018Document74 pagesUSMLE Step 3 Lecture Notes 2017-2018kaelenNo ratings yet
- CeftriaxoneDocument2 pagesCeftriaxonegaatgaatNo ratings yet
- Drugs / Antibiotik: AntimicrobialDocument23 pagesDrugs / Antibiotik: AntimicrobialSania NadianisaNo ratings yet
- Pharma NotesDocument2 pagesPharma Notesanamuj8No ratings yet
- List of Cephalosporins + Uses, Types & Side EffectsDocument5 pagesList of Cephalosporins + Uses, Types & Side EffectsMd. Sabit Ahsan SarkerNo ratings yet
- Katzung Pharmacology Semester 5 TablesDocument29 pagesKatzung Pharmacology Semester 5 TablesfatimaNo ratings yet
- ELE - PID Treatment To Lower Respiratory Tract InfectionsDocument12 pagesELE - PID Treatment To Lower Respiratory Tract InfectionsJane DoeNo ratings yet
- Antibiotics: Lecture 6: Antibiotics For Anaerobic InfectionsDocument12 pagesAntibiotics: Lecture 6: Antibiotics For Anaerobic InfectionsMuath AlqarniNo ratings yet
- AntibioticsDocument17 pagesAntibioticsnehal.nehal92No ratings yet
- Antibacterial DrugsDocument48 pagesAntibacterial DrugsDarlington Dimitri (zeecomedy)No ratings yet
- PHARMA-R3.1-Specific AntibioticsDocument13 pagesPHARMA-R3.1-Specific Antibioticscharmainemargaret.parreno.medNo ratings yet
- Cephalosporins 2018Document33 pagesCephalosporins 2018Harsha MaheshwariNo ratings yet
- 1-Co - Trimoxazol: AntibioticsDocument66 pages1-Co - Trimoxazol: Antibioticsmohamed mahmoudNo ratings yet
- Cefalo Sporin AsDocument5 pagesCefalo Sporin AsErick ZataNo ratings yet
- Antibiotics PharmaDocument4 pagesAntibiotics PharmaJohn Dave V. VillarmenteNo ratings yet
- Treatment of Postpartum Endometritis: Hospital PracticeDocument8 pagesTreatment of Postpartum Endometritis: Hospital Practicefalon papalangiNo ratings yet
- Management of CAP in Adults - Ontario GovernmentDocument2 pagesManagement of CAP in Adults - Ontario GovernmentSukhvir AujlaNo ratings yet
- Session 2 - Antibiotic GeneralDocument14 pagesSession 2 - Antibiotic GeneralrekabmariamNo ratings yet
- CeftriaxoneDocument7 pagesCeftriaxoneGreats HalomoanNo ratings yet
- CephalosporinDocument34 pagesCephalosporinliamhenry9449No ratings yet
- SHC SurgProphylaxisGuidelinesDocument6 pagesSHC SurgProphylaxisGuidelinesDr shehwar100% (1)
- InfectionDocument96 pagesInfectionBassem Georguos LabibNo ratings yet
- CephalosporinsDocument35 pagesCephalosporinsPrasad SangishettyNo ratings yet
- ANTIBIOTICS Pharmacology NursingDocument10 pagesANTIBIOTICS Pharmacology NursingRalph Alfonse De JesusNo ratings yet
- Class: SS-Lactams: Review of Antibiotics (Fill in The Blanks!) Judith L. Rowen, M.DDocument9 pagesClass: SS-Lactams: Review of Antibiotics (Fill in The Blanks!) Judith L. Rowen, M.DNikita JacobsNo ratings yet
- CEPHALOSPORINSDocument14 pagesCEPHALOSPORINSMohan KrishnaNo ratings yet
- Cell Wall SynthesisDocument7 pagesCell Wall SynthesisKC PalattaoNo ratings yet
- Penicillins and CephalosporinsDocument30 pagesPenicillins and CephalosporinsSri RamNo ratings yet
- ChemotherapyDocument46 pagesChemotherapyErl D. Melitante100% (1)
- 6 - Antibacterial-Cell Wall Synthesis InhibitorsDocument29 pages6 - Antibacterial-Cell Wall Synthesis InhibitorsDr. SaniaNo ratings yet
- Antibiotic Classification Mechanism - Sheet1Document2 pagesAntibiotic Classification Mechanism - Sheet1api-329501044No ratings yet
- Antibiotic/Antiviral Policy - Paediatric PCF (EWMSCDocument9 pagesAntibiotic/Antiviral Policy - Paediatric PCF (EWMSCLizbet parrondoNo ratings yet
- L16 ANTIBIOTICS - IN - ORAL - MAXILLOFACIAL - SURGERY Copy 2Document19 pagesL16 ANTIBIOTICS - IN - ORAL - MAXILLOFACIAL - SURGERY Copy 2Ju JuNo ratings yet
- MarketingDocument31 pagesMarketingDodo NorNo ratings yet
- Seizures!!!!Document5 pagesSeizures!!!!ChaojaNo ratings yet
- Antibiotic Class by CoverageDocument3 pagesAntibiotic Class by Coverageayy1No ratings yet
- Fluconazole: ErthromycinDocument7 pagesFluconazole: ErthromycinAseel AlsheeshNo ratings yet
- PharmaDocument6 pagesPharmanoreentamer20No ratings yet
- Streptococcus Pneumoniae Haemophilus Influenzae: Click HereDocument3 pagesStreptococcus Pneumoniae Haemophilus Influenzae: Click HereSiti Hidayatul FitriNo ratings yet
- Antibacterial DR Mostafa Alfishawy AntibioticDocument64 pagesAntibacterial DR Mostafa Alfishawy Antibioticramzi MohamedNo ratings yet
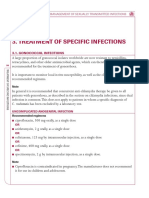
- WHO Guidelines - Management - Sti - Treatment - Specific - InfectionsDocument26 pagesWHO Guidelines - Management - Sti - Treatment - Specific - InfectionsChalwe HowardNo ratings yet
- Role of Recombinant DNA Technology To Improve LifeDocument2 pagesRole of Recombinant DNA Technology To Improve LifeCARL ANGELA SISONNo ratings yet
- Advertisement PaperDocument2 pagesAdvertisement PaperCARL ANGELA SISONNo ratings yet
- Transcription Workshop 4 PDFDocument2 pagesTranscription Workshop 4 PDFCARL ANGELA SISONNo ratings yet
- E Tool HA - Head To NeckDocument8 pagesE Tool HA - Head To NeckCARL ANGELA SISONNo ratings yet
- HA ChesttoAbdomenppt PDFDocument221 pagesHA ChesttoAbdomenppt PDFCARL ANGELA SISON100% (1)
- MT 6314 - Lesson 12 - Introduction To Antimicrobials Beta Lactam and Other Cell Wall InhibitorsDocument12 pagesMT 6314 - Lesson 12 - Introduction To Antimicrobials Beta Lactam and Other Cell Wall InhibitorsCARL ANGELA SISONNo ratings yet
- Educating The Literary Taste by Paz LatorenaDocument4 pagesEducating The Literary Taste by Paz LatorenaCARL ANGELA SISONNo ratings yet
- Conventions For TranscriptionDocument5 pagesConventions For TranscriptionCARL ANGELA SISONNo ratings yet
- 11.1 Introduction To Antimicrobials Beta Lactam Other Cell InhibitorsDocument12 pages11.1 Introduction To Antimicrobials Beta Lactam Other Cell InhibitorsCARL ANGELA SISONNo ratings yet
- Language Transcription Lecture - PDFDocument29 pagesLanguage Transcription Lecture - PDFCARL ANGELA SISONNo ratings yet
- Parafusos PT SemblexDocument10 pagesParafusos PT SemblexSBonderNo ratings yet
- Case AnalyzerDocument19 pagesCase AnalyzeranuragNo ratings yet
- Ecological Consideration of Site AnalysisDocument20 pagesEcological Consideration of Site AnalysisAUST BNo ratings yet
- Productstock 2021-01-18 (Produk Laku & Belum KinwatchDocument32 pagesProductstock 2021-01-18 (Produk Laku & Belum KinwatchKin WatchNo ratings yet
- Hitachi VSP Pricelist PeppmDocument57 pagesHitachi VSP Pricelist PeppmBahman MirNo ratings yet
- GFN Cired PaperDocument8 pagesGFN Cired PaperSukant BhattacharyaNo ratings yet
- Lesson 3 - Practical ResearchDocument17 pagesLesson 3 - Practical ResearchBenNo ratings yet
- Ibps RRB Po Scale - I Prelims Model Mock Test - 8Document7 pagesIbps RRB Po Scale - I Prelims Model Mock Test - 8Sanjay DasNo ratings yet
- Hypertension ESC 2013 PDFDocument32 pagesHypertension ESC 2013 PDFNar RungrojanarakNo ratings yet
- EmbOS GenericDocument324 pagesEmbOS Genericbogd33No ratings yet
- Determination of Iron in Water - SpectrophotometryDocument4 pagesDetermination of Iron in Water - Spectrophotometryhanif ahmadNo ratings yet
- Seminar ReportDocument15 pagesSeminar ReportNipesh MAHARJANNo ratings yet
- New Generation of Reinforcement For Transportation Infrastructure - tcm45-590833Document5 pagesNew Generation of Reinforcement For Transportation Infrastructure - tcm45-590833RevaNo ratings yet
- Catalogue Colorants TextilesDocument5 pagesCatalogue Colorants TextilesAs Des As BenedictionNo ratings yet
- A Randomised Clinical Trial Comparing Myoinositol and Metformin in PCOSDocument7 pagesA Randomised Clinical Trial Comparing Myoinositol and Metformin in PCOSAtika NajlaNo ratings yet
- Cultures of The West A History, Volume 1 To 1750 3rd PDFDocument720 pagesCultures of The West A History, Volume 1 To 1750 3rd PDFtonnyNo ratings yet
- Tescom Technical Training - Pressure Regulators Explained - Ver1.1Document19 pagesTescom Technical Training - Pressure Regulators Explained - Ver1.1Amod DeshpandeNo ratings yet
- Would You Like Eddy Current, Video & Strip Chart in One Portable Case?Document2 pagesWould You Like Eddy Current, Video & Strip Chart in One Portable Case?Daniel Jimenez MerayoNo ratings yet
- TSAR-1 Reverb Quick GuideDocument1 pageTSAR-1 Reverb Quick GuidedraenkNo ratings yet
- Cutting Conics AsDocument3 pagesCutting Conics Asbabe09No ratings yet
- Financial Statements Ias 1Document34 pagesFinancial Statements Ias 1Khalid AzizNo ratings yet
- Nonlinear Robust Control of High-Speed Supercavitating Vehicle in The Vertical PlaneDocument10 pagesNonlinear Robust Control of High-Speed Supercavitating Vehicle in The Vertical Planesamsaptak ghoshNo ratings yet