You might also like
- Optimizing Your Health: An Approachable Guide to Reducing Your Risk of Chronic DiseaseFrom EverandOptimizing Your Health: An Approachable Guide to Reducing Your Risk of Chronic DiseaseNo ratings yet
- 39 Patient Autonomy Informed ConsentDocument3 pages39 Patient Autonomy Informed ConsentMARICRIS NEBIARNo ratings yet
- Patient Autonomy and Informed ConsentDocument10 pagesPatient Autonomy and Informed ConsentShreeyaNo ratings yet
- Patient autonomy paternalismDocument4 pagesPatient autonomy paternalismJeibel BullecerNo ratings yet
- ME Lecture 1, Sept. 5, 20231Document50 pagesME Lecture 1, Sept. 5, 20231Helen Ziqi ZhangNo ratings yet
- PD PaperDocument4 pagesPD PaperMafie BarreiroNo ratings yet
- D. Orr, Robert - The Physicians Right of Refusal What Are The LimitsDocument11 pagesD. Orr, Robert - The Physicians Right of Refusal What Are The LimitsNolan HekhalNo ratings yet
- Ethical Issues in Geriatrics A Guide For CliniciansDocument9 pagesEthical Issues in Geriatrics A Guide For CliniciansThanc FishNo ratings yet
- Running Head: UNIT 9 ASSIGNMENT 1Document7 pagesRunning Head: UNIT 9 ASSIGNMENT 1brittabtNo ratings yet
- Truth-Telling in Medicine: Dra Frances AvilésDocument53 pagesTruth-Telling in Medicine: Dra Frances AvilésishlionNo ratings yet
- Bioethics Module For GE EthicsDocument11 pagesBioethics Module For GE EthicsErrol BuenaventuraNo ratings yet
- The Cost of Conscience CQDocument14 pagesThe Cost of Conscience CQmiguel5628No ratings yet
- Nursing EthicsDocument9 pagesNursing EthicsCord Covie Niluag HonculadaNo ratings yet
- Dashboard Library Study Plans Qbank Analysis Account Help Center & Legal InfoDocument42 pagesDashboard Library Study Plans Qbank Analysis Account Help Center & Legal InfoGauri SurnerNo ratings yet
- Moral Deliberation 2Document6 pagesMoral Deliberation 2christie clausNo ratings yet
- Clin. Cardiol. Vol. 23 (Suppl. 11): Medical Futility Definition DebateDocument11 pagesClin. Cardiol. Vol. 23 (Suppl. 11): Medical Futility Definition DebatecindyNo ratings yet
- 30 Pediatric Bioethics Materials 0518Document5 pages30 Pediatric Bioethics Materials 0518DoaaNo ratings yet
- NU 213 - Health Laws and EthicsDocument4 pagesNU 213 - Health Laws and Ethicsyen.pelaezNo ratings yet
- Summary of ArticleDocument8 pagesSummary of Articleجلال بولادNo ratings yet
- Miss Evers BoysDocument4 pagesMiss Evers Boysarij 20100% (4)
- Running Head: Telling The Truth To A Patient With Dementia 1Document8 pagesRunning Head: Telling The Truth To A Patient With Dementia 1fredrickkuria91No ratings yet
- BAPSDocument21 pagesBAPSayron600No ratings yet
- Autonomy & VeracityDocument3 pagesAutonomy & VeracityLovie Japhet LopezNo ratings yet
- Hafizah Hoshni Truth TellingDocument14 pagesHafizah Hoshni Truth TellinghafizahhoshniNo ratings yet
- Nursing EthicsDocument8 pagesNursing EthicsJam AicaNo ratings yet
- Ethical Principles Resource UnitDocument18 pagesEthical Principles Resource UnitCherry Louise O. SanvictoresNo ratings yet
- Jehovah's Witnesses rights in the emergency departmentDocument3 pagesJehovah's Witnesses rights in the emergency departmentMarco Aurélio Vogel Gomes de MelloNo ratings yet
- Ethical Aspects of Withholding and Withdrawing Life Sustaining TreatmentDocument15 pagesEthical Aspects of Withholding and Withdrawing Life Sustaining TreatmentwakldNo ratings yet
- From Ignorance To Informed Consent The Shift in Medical EthicsDocument13 pagesFrom Ignorance To Informed Consent The Shift in Medical Ethicsapi-665522344No ratings yet
- Rational discussion of blood refusal with Jehovah's WitnessesDocument7 pagesRational discussion of blood refusal with Jehovah's WitnessesMarco Aurélio Vogel Gomes de MelloNo ratings yet
- S1 Hippocratic Oath Seminar and Reading NotesDocument7 pagesS1 Hippocratic Oath Seminar and Reading NotesTaraSubba1995No ratings yet
- Activity 1Document4 pagesActivity 1KyleRepolidon MoralesNo ratings yet
- Introduction To Medical Ethics2147Document45 pagesIntroduction To Medical Ethics2147UsmanRandhawa31No ratings yet
- Ethics and Law For Advanced ModalitiesDocument6 pagesEthics and Law For Advanced ModalitiesJayneNo ratings yet
- Braley Ethics Paper Final March24Document7 pagesBraley Ethics Paper Final March24api-381438480No ratings yet
- Research Paper On Pro EuthanasiaDocument4 pagesResearch Paper On Pro Euthanasiazrpcnkrif100% (1)
- Doctor-Patient Relationship and Medical EthicsDocument19 pagesDoctor-Patient Relationship and Medical EthicsAdji SuwandonoNo ratings yet
- Lecture BioethicsDocument51 pagesLecture BioethicsElvis obajeNo ratings yet
- Ethics in The HospitalDocument4 pagesEthics in The HospitalAllthis ZeusNo ratings yet
- Week 13 AutonomyDocument27 pagesWeek 13 AutonomyRoxanne Ivy ViolaNo ratings yet
- Fiel Angelo G. Mallari, RNDocument68 pagesFiel Angelo G. Mallari, RNfiel mallariNo ratings yet
- Jalt 15 I 4 P 410Document5 pagesJalt 15 I 4 P 410via macarioNo ratings yet
- 2-3 Samillano-SamontegeronDocument19 pages2-3 Samillano-SamontegeronLance_Joshua_7907No ratings yet
- Thesis Statement Pro EuthanasiaDocument6 pagesThesis Statement Pro Euthanasiamizhesternewark100% (1)
- Alternative Medicine - What Is Scientific and Proven?: Click Here For Herbal RemediesDocument3 pagesAlternative Medicine - What Is Scientific and Proven?: Click Here For Herbal RemediesAngadNo ratings yet
- This I Believe 1Document3 pagesThis I Believe 1api-709406220No ratings yet
- This Is Me Now - Danielle SwartzDocument9 pagesThis Is Me Now - Danielle Swartzapi-508771384No ratings yet
- Assisted SuicideDocument8 pagesAssisted Suicideapi-406491631No ratings yet
- Lee-Ethics Paper-3 19 18Document6 pagesLee-Ethics Paper-3 19 18api-301947262No ratings yet
- Idiots, Infants, and The Insane'': Mental Illness and Legal Incompetence, by Thomas SzaszDocument4 pagesIdiots, Infants, and The Insane'': Mental Illness and Legal Incompetence, by Thomas SzaszNicolas MartinNo ratings yet
- Bioethics of Tuskegee Syphilis ExperimentDocument3 pagesBioethics of Tuskegee Syphilis ExperimentHALLEBERRY G. NIETESNo ratings yet
- Thesis On Physician Assisted DeathDocument5 pagesThesis On Physician Assisted Deathbnjkstgig100% (2)
- Important Medical Ethics CasesDocument28 pagesImportant Medical Ethics CasesVidya BalaNo ratings yet
- Decision Making in Incompetent PatientDocument2 pagesDecision Making in Incompetent PatientilhamokNo ratings yet
- Medical Ethics and ProfessionalismDocument10 pagesMedical Ethics and ProfessionalismAlexa MirandaNo ratings yet
- Nursing Ethics: Patient Rights and Informed ConsentDocument11 pagesNursing Ethics: Patient Rights and Informed ConsentJewell Nivera CarpioNo ratings yet
- Assessing Patient Decision Making: When Psychiatry and Bioethics DisagreeDocument4 pagesAssessing Patient Decision Making: When Psychiatry and Bioethics DisagreeLaura ValeroNo ratings yet
- AutonomyDocument22 pagesAutonomyRomelyn AngelNo ratings yet
- Ildefonso Vs SibalDocument4 pagesIldefonso Vs SibalLex LawNo ratings yet
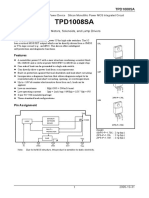
- TPD1008SA High-Side Power Switch GuideDocument11 pagesTPD1008SA High-Side Power Switch GuideOlga PlohotnichenkoNo ratings yet
- Robert Aldrich Greater France A HistoryDocument385 pagesRobert Aldrich Greater France A HistoryJan Zalewski100% (3)
- BOC Import License Documentary RequirementsDocument2 pagesBOC Import License Documentary RequirementsGabriel EmersonNo ratings yet
- S1-17 18 PDFDocument1 pageS1-17 18 PDFganeshp_eeeNo ratings yet
- Paul's Prison Epistles - Lesson 4 - Forum TranscriptDocument22 pagesPaul's Prison Epistles - Lesson 4 - Forum TranscriptThird Millennium MinistriesNo ratings yet
- Threats & Attacks To Information SecurityDocument48 pagesThreats & Attacks To Information SecurityboonandzipNo ratings yet
- OIC Claim FormDocument4 pagesOIC Claim FormPrashant SinghNo ratings yet
- National Bravery Awards - Sub GK 1 To 4Document4 pagesNational Bravery Awards - Sub GK 1 To 4lafdebazNo ratings yet
- NIYOGA Smita Sahgal PDFDocument36 pagesNIYOGA Smita Sahgal PDFAnshika SinghNo ratings yet
- Robin Lohre vs. Posh Maids, Et. Al.Document6 pagesRobin Lohre vs. Posh Maids, Et. Al.NickNo ratings yet
- Sustainable Development Goals (SDGS) : "Achieve Gender Equality and Empower All Women and Girls."Document3 pagesSustainable Development Goals (SDGS) : "Achieve Gender Equality and Empower All Women and Girls."Peter Odosamase OsifoNo ratings yet
- Ledesma v. Municipality of IloiloDocument2 pagesLedesma v. Municipality of IloilokathrynmaydevezaNo ratings yet
- Pleading PublicianaDocument2 pagesPleading Publicianaalfx21683% (6)
- Theories (Juvenile Delinquency) : Strain TheoryDocument15 pagesTheories (Juvenile Delinquency) : Strain TheoryJim CB LunagNo ratings yet
- Tumagan v. Kairuz G.R. No. 198124 September 12 2018 Intra Corporate DisputeDocument14 pagesTumagan v. Kairuz G.R. No. 198124 September 12 2018 Intra Corporate DisputecalmandpeaceNo ratings yet
- 200 SPANISH AND ENGLISH PAST TENSE VERBSDocument5 pages200 SPANISH AND ENGLISH PAST TENSE VERBSElvis Escobar VelasquezNo ratings yet
- Judgement Award ObjectionsDocument43 pagesJudgement Award ObjectionsAshok tiwari100% (1)
- Mecklenburg County DA's Office Concludes Investigation Into Officer-Involved Shooting Death of Frankie JenningsDocument76 pagesMecklenburg County DA's Office Concludes Investigation Into Officer-Involved Shooting Death of Frankie JenningsWCNC DigitalNo ratings yet
- Likong Vs LimDocument2 pagesLikong Vs LimRoosevelt Guerrero100% (2)
- Ipc ProjectDocument27 pagesIpc Projectkeerthi81% (16)
- ReadmeDocument68 pagesReadmeRezguiNo ratings yet
- The Electric Field of A Plane Polarized Electromagnetic Wave in Free Space at Timeâ T 0 Is Given by An ExpressionDocument3 pagesThe Electric Field of A Plane Polarized Electromagnetic Wave in Free Space at Timeâ T 0 Is Given by An ExpressionAshutosh PathakNo ratings yet
- Msds 51910419745 Titan SilverDocument6 pagesMsds 51910419745 Titan SilverAnonymous fXWzyInNo ratings yet
- TANSIDCODocument3 pagesTANSIDCOsanthosh.smtsNo ratings yet
- AssessingtheEffectivenessoftheInternalControlDocument6 pagesAssessingtheEffectivenessoftheInternalControlLeulNo ratings yet
- NCRP Report No. 177 PDFDocument245 pagesNCRP Report No. 177 PDFVivien FerradaNo ratings yet
- Law Reading For Executive Magistrate Volume IDocument235 pagesLaw Reading For Executive Magistrate Volume IManishNo ratings yet
- Political Caricature Analysis American PeriodDocument3 pagesPolitical Caricature Analysis American PeriodVenus SalgadoNo ratings yet
- General Provisions of Contract LawDocument4 pagesGeneral Provisions of Contract LawMika MolinaNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (16)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- CBT Strategies: CBT Strategies for Overcoming Panic, Fear, Depression, Anxiety, Worry, and AngerFrom EverandCBT Strategies: CBT Strategies for Overcoming Panic, Fear, Depression, Anxiety, Worry, and AngerNo ratings yet
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- How To Understand Your Anger For Better Mental Health: How To Control Emotions And Eliminate Stress In Your LifeFrom EverandHow To Understand Your Anger For Better Mental Health: How To Control Emotions And Eliminate Stress In Your LifeNo ratings yet
- Summary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (11)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Inmersion Into The Shadown Effective Method Of Dark Psychology: How To Use The Best Persuasion Techniques To Achieve Your Best Goals And How To Protect Yourself From Being ManipulatedFrom EverandInmersion Into The Shadown Effective Method Of Dark Psychology: How To Use The Best Persuasion Techniques To Achieve Your Best Goals And How To Protect Yourself From Being ManipulatedRating: 4 out of 5 stars4/5 (1)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisFrom EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisRating: 5 out of 5 stars5/5 (8)