You might also like
- Affidavit of Status As Secured Party,/ A Fictitious Corporation/not Responsible For Any Debt From The All Capital Legal NameDocument5 pagesAffidavit of Status As Secured Party,/ A Fictitious Corporation/not Responsible For Any Debt From The All Capital Legal Namestephanie harvey100% (6)
- Bail BondDocument5 pagesBail BondStephanie's World100% (1)
- Konica Minolta Bizhub C220 C280 C360 SERVICE MANUALDocument0 pagesKonica Minolta Bizhub C220 C280 C360 SERVICE MANUALYury Kobzar83% (24)
- Global Reinstatement Form (English)Document2 pagesGlobal Reinstatement Form (English)Demir Omerovic60% (5)
- SPE-183785-MS BreakdownDocument22 pagesSPE-183785-MS BreakdownMartin RylanceNo ratings yet
- Wiring Diagram For Elevonic® R-SeriesDocument12 pagesWiring Diagram For Elevonic® R-SeriesSamuel AcevedoNo ratings yet
- Customer Information SheetDocument1 pageCustomer Information SheetteliscopidesNo ratings yet
- Odsp Application Form FullDocument2 pagesOdsp Application Form FullPatricia EspirituNo ratings yet
- Global Reinstatement Form (English)Document2 pagesGlobal Reinstatement Form (English)last loveNo ratings yet
- 2nd Rev Polokwt Dole Akap FormDocument1 page2nd Rev Polokwt Dole Akap FormMeryam DalganNo ratings yet
- 2nd - Rev - POLOKWT DOLE AKAP Form PDFDocument1 page2nd - Rev - POLOKWT DOLE AKAP Form PDFReamelNo ratings yet
- Document Release Requirements (Client - Representative - Out of The Country)Document3 pagesDocument Release Requirements (Client - Representative - Out of The Country)Cassandra RamosNo ratings yet
- Passport Application Form 2015Document3 pagesPassport Application Form 2015mich48chinNo ratings yet
- Imm5476 Use of A Representative (2021-11) - 23Document3 pagesImm5476 Use of A Representative (2021-11) - 23farmangousiyaNo ratings yet
- Volunteer Registration at MSLRPDocument1 pageVolunteer Registration at MSLRPsanluisreyparishNo ratings yet
- De Luna Heinrich Theraja Recaña - MDRDocument1 pageDe Luna Heinrich Theraja Recaña - MDROcir TenorioNo ratings yet
- This Form Is Not For Sale: Overseas Wokers Welfare AdministrationDocument1 pageThis Form Is Not For Sale: Overseas Wokers Welfare AdministrationBahilar MaryJaneNo ratings yet
- Checklist of Requirements For SRRV Application PDF EDITABLEDocument1 pageChecklist of Requirements For SRRV Application PDF EDITABLEОлег ТимченкоNo ratings yet
- Adobe Scan 20 Feb 2024Document1 pageAdobe Scan 20 Feb 2024Saranyan SridharNo ratings yet
- Barbazza Membership FormDocument4 pagesBarbazza Membership FormJugger AfrondozaNo ratings yet
- Vendor Employee Agreement Moa (NCCC)Document2 pagesVendor Employee Agreement Moa (NCCC)Ghing-Ghing ZitaNo ratings yet
- Global Reinstatement Form (English)Document2 pagesGlobal Reinstatement Form (English)IFARATABAMINo ratings yet
- Affivadit CSGDocument1 pageAffivadit CSGjeswynnemartin67No ratings yet
- Imm5476 (1) MERCANDocument2 pagesImm5476 (1) MERCANNylana OzirNo ratings yet
- Las 120 Jornadas de Sodoma IDocument2 pagesLas 120 Jornadas de Sodoma ICesar MonzantNo ratings yet
- Whatley Health Services, IncDocument2 pagesWhatley Health Services, IncElla WardNo ratings yet
- General Form No. 58 (A) : Hon. Eleanor Villanueva TugnaDocument2 pagesGeneral Form No. 58 (A) : Hon. Eleanor Villanueva TugnaEdmundo SantosNo ratings yet
- Use of A Representative: N/A N/A N/ADocument2 pagesUse of A Representative: N/A N/A N/AAngel VNo ratings yet
- MDR PhilhealthDocument1 pageMDR Philhealthhannahpanaligan7No ratings yet
- 2022 EDSP App FormDocument2 pages2022 EDSP App FormKim JonginNo ratings yet
- Application Form No. 16Document3 pagesApplication Form No. 16Iskolar TimeNo ratings yet
- Member Info SheetDocument2 pagesMember Info Sheetbernaflor pacantaraNo ratings yet
- Buyer Info Sheet 1Document1 pageBuyer Info Sheet 1api-636430593No ratings yet
- Member Data Record: Philippine Health Insurance CorporationDocument1 pageMember Data Record: Philippine Health Insurance CorporationJenyza SyticoNo ratings yet
- Member Data Record: de Lara, Bianca Jesmine AlcantaraDocument1 pageMember Data Record: de Lara, Bianca Jesmine AlcantaraaliannaNo ratings yet
- CE Cash 2024.xlsx C.EDocument1 pageCE Cash 2024.xlsx C.Eappledelosreyes02142011No ratings yet
- Member Data Record: Philippine Health Insurance CorporationDocument1 pageMember Data Record: Philippine Health Insurance CorporationRO C KYNo ratings yet
- Member Data Record: Philippine Health Insurance CorporationDocument1 pageMember Data Record: Philippine Health Insurance CorporationRO C KYNo ratings yet
- Carlos Ruiz - Original - Ownership - PIG - 2014-07-30 - SignedDocument5 pagesCarlos Ruiz - Original - Ownership - PIG - 2014-07-30 - Signedib178057No ratings yet
- SASSA Affivadit For Disability GrantDocument1 pageSASSA Affivadit For Disability Grantolwethu moboNo ratings yet
- Group Sign On Sheet - CUB 2014Document2 pagesGroup Sign On Sheet - CUB 2014FutureCentreTrustNo ratings yet
- Affivadit For OAG v1.2Document1 pageAffivadit For OAG v1.2khwezishezi35No ratings yet
- Schedule 1applicationDocument2 pagesSchedule 1applicationBekeri TesfayeNo ratings yet
- WestJet ReligiousExemption-Form enDocument4 pagesWestJet ReligiousExemption-Form enDean AminNo ratings yet
- PhilHelath MDRDocument1 pagePhilHelath MDRDeanna GarciaNo ratings yet
- Pyramid FormDocument1 pagePyramid FormRavindraPatilNo ratings yet
- Scholarship Program: Overseas Workers Welfare AdministrationDocument1 pageScholarship Program: Overseas Workers Welfare AdministrationErica TanNo ratings yet
- BSP CertDocument1 pageBSP CertAngel May SarmientoNo ratings yet
- Application Form Incoming 1st Year CollegeDocument4 pagesApplication Form Incoming 1st Year Collegekrazy uwuNo ratings yet
- General Form 58aDocument2 pagesGeneral Form 58aRodelLaborNo ratings yet
- DocumentlindasDocument2 pagesDocumentlindasMelinda R. FranciscoNo ratings yet
- Member Data Record: Santos, Hershey Mae CasucoDocument1 pageMember Data Record: Santos, Hershey Mae CasucoHershey SantosNo ratings yet
- Edsp Application Form For 2022 2023Document1 pageEdsp Application Form For 2022 2023Nizea Camille Navarro JavierNo ratings yet
- Participants Application FormDocument1 pageParticipants Application FormAndro Brendo VillapandoNo ratings yet
- Member Data Record: Philippine Health Insurance CorporationDocument1 pageMember Data Record: Philippine Health Insurance CorporationJonjie MiladoNo ratings yet
- Patient Admission Form Sept2014Document1 pagePatient Admission Form Sept2014elmore kakaNo ratings yet
- Application For Insurance Agents Walk-In Examination FormDocument1 pageApplication For Insurance Agents Walk-In Examination FormAsisclo CastanedaNo ratings yet
- NEF Application Form 28nov2022Document11 pagesNEF Application Form 28nov2022NicolasNo ratings yet
- Acknowledgement Receipt Standard FormDocument6 pagesAcknowledgement Receipt Standard Formriolyncrissa.t.malapadNo ratings yet
- Manual Employment Application FormDocument1 pageManual Employment Application FormDafrosa Elleonora NamangNo ratings yet
- Appointing A Representative. Cancelling The Appointment of A RepresentativeDocument2 pagesAppointing A Representative. Cancelling The Appointment of A RepresentativeBiggsterNo ratings yet
- Bitcoin in India: A Deep Down Summary: October 2019Document6 pagesBitcoin in India: A Deep Down Summary: October 2019Sunny18No ratings yet
- Dynamic QR code User guideDocument7 pagesDynamic QR code User guidevinil vkNo ratings yet
- Business Analytics in The Banking IndustryDocument11 pagesBusiness Analytics in The Banking Industrykomal bajajNo ratings yet
- 2023 Interdict Application - MCEJO Vs Tendele - 5th To 8th Answering Affidavit & MCEJO's Replying AffidavitDocument190 pages2023 Interdict Application - MCEJO Vs Tendele - 5th To 8th Answering Affidavit & MCEJO's Replying AffidavitJanice TooleyNo ratings yet
- Arduino ReportDocument10 pagesArduino ReportSrinan MarvelNo ratings yet
- 40QB/QD Series: Floor Standing Split SystemDocument2 pages40QB/QD Series: Floor Standing Split SystemalexmilarNo ratings yet
- Data Mining Lecture 10B: ClassificationDocument62 pagesData Mining Lecture 10B: ClassificationArul Kumar VenugopalNo ratings yet
- Aggregation of Small Loads For Demand Response Programs - Implementation and Challenges - A ReviewDocument6 pagesAggregation of Small Loads For Demand Response Programs - Implementation and Challenges - A ReviewSergio RosenbergNo ratings yet
- Alia APF810 Oval Gear FlowmeterDocument4 pagesAlia APF810 Oval Gear FlowmeterRexCrazyMindNo ratings yet
- 7.1.6 Lab4 - Use Wireshark To Examine Ethernet FramesDocument8 pages7.1.6 Lab4 - Use Wireshark To Examine Ethernet FramesPham Quang Huy (K16HL)No ratings yet
- Ardora ReportDocument10 pagesArdora ReportJara Dominguez VanessaNo ratings yet
- On The Performance of Intrusion Detection Systems With Hidden Multilayer Neural Network Using DSD TrainingDocument21 pagesOn The Performance of Intrusion Detection Systems With Hidden Multilayer Neural Network Using DSD TrainingAIRCC - IJCNCNo ratings yet
- DB2 - SQL Error CodesDocument24 pagesDB2 - SQL Error CodesMudit RanaNo ratings yet
- PT2Document18 pagesPT2Quach Hoang Nam (K16HCM)No ratings yet
- IC Compiler IIICC II后端设计流程超详细 - 凳子花的博客-CSDN博客 - iccxdgrfDocument58 pagesIC Compiler IIICC II后端设计流程超详细 - 凳子花的博客-CSDN博客 - iccxdgrfRAZNo ratings yet
- Individual Assignment - PM PDFDocument3 pagesIndividual Assignment - PM PDFNaman BajajNo ratings yet
- Project Portfolio Management Dissertation TopicsDocument5 pagesProject Portfolio Management Dissertation TopicsWhereToBuyCollegePapersUK100% (1)
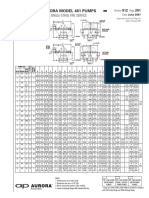
- Aurora Model 481 Pumps: Single-Stage Fire ServiceDocument20 pagesAurora Model 481 Pumps: Single-Stage Fire ServicenhacotungNo ratings yet
- Making Type 1 Fonts For VietnameseDocument6 pagesMaking Type 1 Fonts For VietnameseMihaiLeonteNo ratings yet
- Analysis of Pedestrian Vehicle Interactions and Delay PDFDocument5 pagesAnalysis of Pedestrian Vehicle Interactions and Delay PDFvalNo ratings yet
- Recommendations For The Safe Storage of Rice in A Silo 1612809155Document9 pagesRecommendations For The Safe Storage of Rice in A Silo 1612809155Humayoun Ali TahiriNo ratings yet
- Spatiotemporal Mining and Moving Object Data: Hafiz Danish NadeemDocument3 pagesSpatiotemporal Mining and Moving Object Data: Hafiz Danish Nadeemsyed bilalNo ratings yet
- 13.8 Water Supply Systems DesignDocument2 pages13.8 Water Supply Systems DesignAngelyn MarantalNo ratings yet
- MT / MTZ / MPZ / NTZ: Maneurop® Reciprocating CompressorsDocument19 pagesMT / MTZ / MPZ / NTZ: Maneurop® Reciprocating Compressorsomar leonNo ratings yet
- Stock Compression Spring CatalogDocument548 pagesStock Compression Spring CatalogRatno WijayaNo ratings yet
- AIASDocument5 pagesAIASAVMNo ratings yet
- Modul 2.02Document21 pagesModul 2.02izzatul islamNo ratings yet