You might also like
- Redlands' 2015 California Public Records RequestsDocument26 pagesRedlands' 2015 California Public Records RequestsBeau Yarbrough100% (1)
- HistotechniquesDocument47 pagesHistotechniquesJean VipinosaNo ratings yet
- Routine Histotechniques - Lecture 1Document47 pagesRoutine Histotechniques - Lecture 1Gerald John Paz100% (1)
- General Pathology Lecture Group 1 HandoutDocument6 pagesGeneral Pathology Lecture Group 1 HandoutCecille AnnNo ratings yet
- Preparation of Histological SpecimensDocument26 pagesPreparation of Histological SpecimensMuhammad RizkyNo ratings yet
- Training Sinal PDFDocument15 pagesTraining Sinal PDFlobitoferoz81No ratings yet
- His To PathologyDocument52 pagesHis To PathologyRathinaKumarNo ratings yet
- 5 - Introduction To Tissue ProcessingDocument9 pages5 - Introduction To Tissue Processingbsramos2023No ratings yet
- Introduction To Histological EquipmentsDocument106 pagesIntroduction To Histological Equipmentshenryjack1100% (3)
- Histological TechniqueDocument8 pagesHistological Techniqueاسماء زياد عبدالجبارNo ratings yet
- Histopath Review 2017 (3.0 Hrs Lecture) Notes PDFDocument111 pagesHistopath Review 2017 (3.0 Hrs Lecture) Notes PDFPerlieCaguete100% (1)
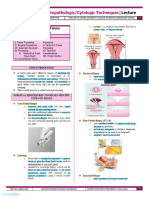
- Histopathology and CytologyDocument26 pagesHistopathology and CytologyKirsten ValenzuelaNo ratings yet
- 04 HistotechniquesDocument70 pages04 HistotechniquesJulliene Dadole100% (1)
- Principles and Practices of Contamination Control and CleanroomsFrom EverandPrinciples and Practices of Contamination Control and CleanroomsNo ratings yet
- Mtap - Special Histopath TechniquesDocument21 pagesMtap - Special Histopath TechniquesK-idol LiveNo ratings yet
- Part 3 Omni SetupDocument19 pagesPart 3 Omni SetupReem AwwadNo ratings yet
- Quarter3 English ModuleDocument6 pagesQuarter3 English ModuleIan Daquipil100% (2)
- Histology ReviewerDocument5 pagesHistology Reviewerkmdynasty_No ratings yet
- Flaps in Maxillofacial ReconstructionDocument29 pagesFlaps in Maxillofacial ReconstructionJaspreet Kaur33% (3)
- His To Tech FrozenDocument13 pagesHis To Tech Frozenjulo_05100% (1)
- Tissue Processing NoteDocument11 pagesTissue Processing NoteXty Wop100% (1)
- Frozen SectionDocument34 pagesFrozen SectionSnigdha Sinha100% (2)
- EmbeddingDocument6 pagesEmbeddingVikash KumarNo ratings yet
- Introduction MethodsDocument70 pagesIntroduction MethodsHohai ConcepcionNo ratings yet
- Histopath Lab Rules and RegulationsDocument4 pagesHistopath Lab Rules and RegulationsFedz FederisoNo ratings yet
- HISTOPATH FIXATIONdocx PDFDocument8 pagesHISTOPATH FIXATIONdocx PDFmaricel duque100% (1)
- Frozen SectionDocument9 pagesFrozen SectionBabatunde AjibolaNo ratings yet
- Health DigestDocument14 pagesHealth DigestKristina SabuNo ratings yet
- Cell Path 5Document6 pagesCell Path 5mcpaulfreemanNo ratings yet
- HistologyDocument8 pagesHistologyMark justine GamiaoNo ratings yet
- Fixation ImpregnationDocument18 pagesFixation ImpregnationKarla Mae Tolelis - BurlatNo ratings yet
- Act. 1 - Instrumentation in HistotechnologyDocument9 pagesAct. 1 - Instrumentation in HistotechnologyBSMLS TINGZNo ratings yet
- Biological TechniquesDocument9 pagesBiological Techniquesaaliya saaheenNo ratings yet
- Tissue Fixation, Embedding and Block Preparation: Nayan M BDocument27 pagesTissue Fixation, Embedding and Block Preparation: Nayan M BaziskfNo ratings yet
- Mod 2.1Document7 pagesMod 2.1Pauline Louise S. DURANNo ratings yet
- Fresh Tissue ExaminationDocument6 pagesFresh Tissue ExaminationChiizu iraNo ratings yet
- Micro Techniques 1Document38 pagesMicro Techniques 1يوسف إبراهيمNo ratings yet
- His To PathologyDocument2 pagesHis To PathologypixiedustNo ratings yet
- Gregorios-Histopathologic-Techniques Ch3 and 29Document78 pagesGregorios-Histopathologic-Techniques Ch3 and 29EllaineSonejaNo ratings yet
- Tissue ProcessingDocument34 pagesTissue Processingkeileykiel26No ratings yet
- Histology Its Methods of StudyDocument6 pagesHistology Its Methods of StudyA18- Jessa Mae DayagNo ratings yet
- Preparation of Histological SpecimensDocument4 pagesPreparation of Histological SpecimensAqilah HazwaniNo ratings yet
- Answersheet HistopathDocument3 pagesAnswersheet HistopathAlanah JaneNo ratings yet
- Special Technique On CytohistologyDocument36 pagesSpecial Technique On CytohistologyKecil DekNo ratings yet
- Preparation of Fresh TissueDocument3 pagesPreparation of Fresh TissueMaster ChiefNo ratings yet
- Trans Histopath 3Document5 pagesTrans Histopath 33A PEÑA AndreaNo ratings yet
- Final Histopath Notes.Document19 pagesFinal Histopath Notes.anneorigmtNo ratings yet
- Review Article: Intra-Operative Frozen Section Consultation: Concepts, Applications and LimitationsDocument9 pagesReview Article: Intra-Operative Frozen Section Consultation: Concepts, Applications and Limitationsfebri susantoNo ratings yet
- Histopathology: 1. Routine Histopathologic ExaminationDocument2 pagesHistopathology: 1. Routine Histopathologic ExaminationPat DazaNo ratings yet
- Histopath Activity 7Document4 pagesHistopath Activity 7Nico LokoNo ratings yet
- HPCT Lec Week 3 - Fresh Tissue Examination, Special Tissue Processing, Fixation.Document3 pagesHPCT Lec Week 3 - Fresh Tissue Examination, Special Tissue Processing, Fixation.Marc Jeff GabasaNo ratings yet
- Histotechnology Practices PDFDocument16 pagesHistotechnology Practices PDFNsanzimana JeromeNo ratings yet
- Instrumentasi Tissu Proces 2020Document39 pagesInstrumentasi Tissu Proces 2020Santi Ismatul AulaNo ratings yet
- Histopathology Manual 122144Document17 pagesHistopathology Manual 122144Eliariz Dela CruzNo ratings yet
- Histology - Wet Lab 1Document36 pagesHistology - Wet Lab 1Victoria RennaNo ratings yet
- Caderno UC1 HistologyDocument15 pagesCaderno UC1 HistologyantonietohNo ratings yet
- Intro To HistologyDocument29 pagesIntro To Histologybunniecaronan113003No ratings yet
- Modules 7 12 HistopathologyDocument9 pagesModules 7 12 HistopathologyKrystelle Anne PenaflorNo ratings yet
- Lab Diagnosis of Cancer: Staging and PrognosisDocument35 pagesLab Diagnosis of Cancer: Staging and PrognosisAuri ArlidenNo ratings yet
- Exam MicroscopicoDocument20 pagesExam Microscopicojuan carlosNo ratings yet
- 6.tissue Prcessing, PDFDocument10 pages6.tissue Prcessing, PDFDewi Masyithah Darlan50% (2)
- Atlas of Mohs and Frozen Section Cutaneous PathologyFrom EverandAtlas of Mohs and Frozen Section Cutaneous PathologyMichael B. MorganNo ratings yet
- Metallic ImpregnationDocument10 pagesMetallic ImpregnationVince Nicole MoraNo ratings yet
- Exercise 4cDocument6 pagesExercise 4cVince Nicole MoraNo ratings yet
- Exercise 3 4aDocument8 pagesExercise 3 4aVince Nicole MoraNo ratings yet
- Types of Fixatives 1Document12 pagesTypes of Fixatives 1Vince Nicole MoraNo ratings yet
- DSP Lab RecordDocument97 pagesDSP Lab RecordLikhita UttamNo ratings yet
- [Download pdf] Mastering Microsoft Fabric Saasification Of Analytics 1St Edition Debananda Ghosh online ebook all chapter pdfDocument42 pages[Download pdf] Mastering Microsoft Fabric Saasification Of Analytics 1St Edition Debananda Ghosh online ebook all chapter pdflinda.coles284100% (11)
- S800 SCL SR - 2CCC413009B0201 PDFDocument16 pagesS800 SCL SR - 2CCC413009B0201 PDFBalan PalaniappanNo ratings yet
- Laying Out Compoud Curve and Reverse by Deflection Angle MethodDocument10 pagesLaying Out Compoud Curve and Reverse by Deflection Angle MethodEljenColanggo0% (2)
- RymesDocument6 pagesRymesFarida YesminNo ratings yet
- Soal DescriptiveDocument4 pagesSoal DescriptiveLuh SetiawatiNo ratings yet
- Reglas Digitales Mitutoyo Scale Units Linear ScalesDocument31 pagesReglas Digitales Mitutoyo Scale Units Linear ScalesAngelmambrinNo ratings yet
- 4K Resolution: The Future of ResolutionsDocument15 pages4K Resolution: The Future of ResolutionsRavi JoshiNo ratings yet
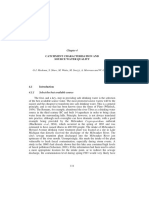
- Catchment CharacterisationDocument48 pagesCatchment CharacterisationSherlock BaileyNo ratings yet
- Apacer SV250 CFast BiCS5 AA2 XX5XXX XXXEX Spec v1 - 3107344Document25 pagesApacer SV250 CFast BiCS5 AA2 XX5XXX XXXEX Spec v1 - 3107344ManunoghiNo ratings yet
- Group 3 Aia ReportDocument26 pagesGroup 3 Aia ReportNAVAS E VNo ratings yet
- 15b. FANC - Focused Antenatal Care - Koros E.KDocument71 pages15b. FANC - Focused Antenatal Care - Koros E.KMercy KeruboNo ratings yet
- Installiation of Automatic Fire Sprinkler System and Design CalculationDocument8 pagesInstalliation of Automatic Fire Sprinkler System and Design CalculationSat AungNo ratings yet
- GD - 202011 - G2 Inverter - Sungrow Single Phase Inverter Commissioning Guide - V1.0Document13 pagesGD - 202011 - G2 Inverter - Sungrow Single Phase Inverter Commissioning Guide - V1.0AbbasNo ratings yet
- Farm Size Factor Productivity and Returns To ScaleDocument8 pagesFarm Size Factor Productivity and Returns To ScaleAkshay YadavNo ratings yet
- Ecs C42iix Rev C Vit m2400 1Document36 pagesEcs C42iix Rev C Vit m2400 1Victor Pic100% (1)
- Unit 2 SignalsDocument3 pagesUnit 2 SignalsDigitallogicdlNo ratings yet
- Valores de Laboratorio Harriet LaneDocument14 pagesValores de Laboratorio Harriet LaneRonald MoralesNo ratings yet
- Unicast Rotary Breaker Wear Parts: Cast To Last. Designed For Hassle-Free Removal and ReplacementDocument2 pagesUnicast Rotary Breaker Wear Parts: Cast To Last. Designed For Hassle-Free Removal and ReplacementAugusto TorresNo ratings yet
- MSC in Subsea Engineering - Flexible Pipe Analysis Lecture JP 2023Document67 pagesMSC in Subsea Engineering - Flexible Pipe Analysis Lecture JP 2023Fakey LaazNo ratings yet
- Vandex Plug: Rapid-Setting, Crystalline Hydraulic CementDocument2 pagesVandex Plug: Rapid-Setting, Crystalline Hydraulic CementQuerubin EboliNo ratings yet
- Outline On Dengue Fever - EDITEDDocument2 pagesOutline On Dengue Fever - EDITEDDavid Skeat0% (1)
- Amotec 12864Q DisplayDocument17 pagesAmotec 12864Q DisplayEdgarNo ratings yet
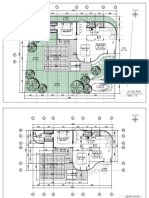
- 2023.01.25 Plan Pecatu Villa - FinishDocument3 pages2023.01.25 Plan Pecatu Villa - FinishTika AgungNo ratings yet
- Mechanics of Solids - (Riveted and Welded Joints)Document37 pagesMechanics of Solids - (Riveted and Welded Joints)TusherNo ratings yet
- Keeling 1960 PDFDocument4 pagesKeeling 1960 PDFErick AmâncioNo ratings yet




































































![[Download pdf] Mastering Microsoft Fabric Saasification Of Analytics 1St Edition Debananda Ghosh online ebook all chapter pdf](https://imgv2-2-f.scribdassets.com/img/document/732592422/149x198/f876884e8e/1716289284?v=1)